Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):453-458
DOI 10.1590/S0100-72032012001000004
PURPOSES: To assess the quality of life of breast cancer survivors compared to a sample of age-matched healthy women. METHODS: A cross-sectional design was conducted on 199 consecutive breast cancer survivors, one year or more after diagnosis, treated at two large hospitals. The patients were compared to age-matched healthy women consisting of employees and volunteers of the two hospitals. Quality of life was evaluated using the World Health Organization Quality of Life Questionnaire, version Bref (WHOQOL-bref) and socioeconomic, clinical, and treatment data were obtained. The χ² test and a generalized linear model were used for statistical analysis. The adopted level of significance was 5%. RESULTS: The mean age of breast cancer survivors was 54.4 years (SD=10.4) and the average length of time since diagnosis was 5.0 years (SD=4.6). The survivors reported a poorer overall quality of life (p=0.001), and for the physical (p<0.001), psychological (p=0.002) and environment (p=0.029) domains than the comparison group, after adjusting for potential confounders. There was no significant difference in the social relationships domain (p=0.929) between groups. CONCLUSION: The results suggest that many breast cancer survivors experienced worse quality of life assessment than healthy women. This information may be useful to establish strategies to improve the quality of life of women with breast cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):453-458
DOI 10.1590/S0100-72032012001000004
PURPOSES: To assess the quality of life of breast cancer survivors compared to a sample of age-matched healthy women. METHODS: A cross-sectional design was conducted on 199 consecutive breast cancer survivors, one year or more after diagnosis, treated at two large hospitals. The patients were compared to age-matched healthy women consisting of employees and volunteers of the two hospitals. Quality of life was evaluated using the World Health Organization Quality of Life Questionnaire, version Bref (WHOQOL-bref) and socioeconomic, clinical, and treatment data were obtained. The χ² test and a generalized linear model were used for statistical analysis. The adopted level of significance was 5%. RESULTS: The mean age of breast cancer survivors was 54.4 years (SD=10.4) and the average length of time since diagnosis was 5.0 years (SD=4.6). The survivors reported a poorer overall quality of life (p=0.001), and for the physical (p<0.001), psychological (p=0.002) and environment (p=0.029) domains than the comparison group, after adjusting for potential confounders. There was no significant difference in the social relationships domain (p=0.929) between groups. CONCLUSION: The results suggest that many breast cancer survivors experienced worse quality of life assessment than healthy women. This information may be useful to establish strategies to improve the quality of life of women with breast cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):466-472
DOI 10.1590/S0100-72032012001000006
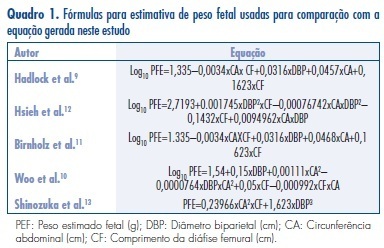
PURPOSES: To elaborate models for the estimation of fetal weight and longitudinal reference intervals of estimated fetal weight (EFW) using a sample of the Brazilian population. METHODS: Prospective observational study. Two groups of patients were evaluated: Group EFW (estimation of fetal weight): to elaborate (EFW-El) and validate (EFW-Val) a model for the prediction of fetal weight; Group LRI (longitudinal reference intervals): To elaborate (LRI-El) and validate (LRF-Val) conditional (longitudinal) percentiles of EFW. Polynomial regression analysis was applied to the data from subgroup EFW-El to elaborate a model for the estimation of fetal weight. The performance of this model was compared to those of previously published formulas. Linear mixed models were used for the elaboration of longitudinal reference intervals of EFW using data from subgroup LRI-El. Data obtained from subgroup LRI-Val were used to validate these intervals. RESULTS: Group EFW consisted of 458 patients (EFW-El: 367; EFW-Val: 91) and Group LRI consisted of 315 patients (LRI-El: 265; LRI-Val: 50). The model obtained for EFW was: EFW=-8.277+2.146xBPDxACxFL-2.449xFLxBPD². The performances of other models were significantly worse than those obtained with our formula. Equations for the prediction of conditional percentiles of EFW were derived from the longitudinal observation of patients of subgroup LRI-El and validated with data from subgroup LRI-Val. CONCLUSIONS: We described a method for customization of longitudinal reference intervals of EFW obtained using formulas generated from a sample of the Brazilian population.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):466-472
DOI 10.1590/S0100-72032012001000006
PURPOSES: To elaborate models for the estimation of fetal weight and longitudinal reference intervals of estimated fetal weight (EFW) using a sample of the Brazilian population. METHODS: Prospective observational study. Two groups of patients were evaluated: Group EFW (estimation of fetal weight): to elaborate (EFW-El) and validate (EFW-Val) a model for the prediction of fetal weight; Group LRI (longitudinal reference intervals): To elaborate (LRI-El) and validate (LRF-Val) conditional (longitudinal) percentiles of EFW. Polynomial regression analysis was applied to the data from subgroup EFW-El to elaborate a model for the estimation of fetal weight. The performance of this model was compared to those of previously published formulas. Linear mixed models were used for the elaboration of longitudinal reference intervals of EFW using data from subgroup LRI-El. Data obtained from subgroup LRI-Val were used to validate these intervals. RESULTS: Group EFW consisted of 458 patients (EFW-El: 367; EFW-Val: 91) and Group LRI consisted of 315 patients (LRI-El: 265; LRI-Val: 50). The model obtained for EFW was: EFW=-8.277+2.146xBPDxACxFL-2.449xFLxBPD². The performances of other models were significantly worse than those obtained with our formula. Equations for the prediction of conditional percentiles of EFW were derived from the longitudinal observation of patients of subgroup LRI-El and validated with data from subgroup LRI-Val. CONCLUSIONS: We described a method for customization of longitudinal reference intervals of EFW obtained using formulas generated from a sample of the Brazilian population.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):473-477
DOI 10.1590/S0100-72032012001000007
PURPOSES: To evaluate the hemodynamic patterns of the ophthalmic artery by Doppler analysis in women with gestational diabetes mellitus (GDM), comparing them to normal pregnant women. METHODS: A prospective case-control study that analyzed the ophthalmic artery Doppler indices in two groups: one consisting of 40 women diagnosed with GDM and the other of 40 normal pregnant women. Included were pregnant women with GDM criteria of the American Diabetes Association - 2012, with 27 weeks of pregnancy to term, and excluded were women with hypertension, use of vasoactive drugs on or previous diagnosis of diabetes. Doppler analysis was performed in one eye with a 10 MHz linear transducer and the Sonoace 8000 Live Medison® equipment . The following variables were analyzed: pulsatility index (PI), resistance index (RI), peak velocity ratio (PVR), peak systolic velocity (PSV) and end diastolic velocity (EDV). To analyze the normality of the samples we used the Lillefors test, and to compare means and medians we used the Student's t-test and Mann-Whitney test according to data normality, with the level of significance set at 95%. RESULTS: The median and mean values with standard deviation of the variables of the ophthalmic artery Dopplervelocimetry group GDM and normal pregnant women were: IP=1.7±0.6 and 1.6±0.4 (p=0.7); IR=0.7 and 0.7 (p=0.9); RPV=0.5±0.1 and 0.5±0.1 (p=0.1), PSV=33.6 and 31.9 cm/sec (p=0.7); VDF=6.3 and 7.9 cm/sec (p=0.4). There was no significant difference in the means and medians of these variables between the two groups of pregnant women. CONCLUSIONS: The ophthalmic artery hemodynamic patterns, analyzed by means of a Doppler technique remained unchanged in the group of pregnant women with GDM compared to the group of normal pregnant women, suggesting that the time of exposure to the disease during pregnancy was too short to cause significant vascular disorders in the central territory.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):473-477
DOI 10.1590/S0100-72032012001000007
PURPOSES: To evaluate the hemodynamic patterns of the ophthalmic artery by Doppler analysis in women with gestational diabetes mellitus (GDM), comparing them to normal pregnant women. METHODS: A prospective case-control study that analyzed the ophthalmic artery Doppler indices in two groups: one consisting of 40 women diagnosed with GDM and the other of 40 normal pregnant women. Included were pregnant women with GDM criteria of the American Diabetes Association - 2012, with 27 weeks of pregnancy to term, and excluded were women with hypertension, use of vasoactive drugs on or previous diagnosis of diabetes. Doppler analysis was performed in one eye with a 10 MHz linear transducer and the Sonoace 8000 Live Medison® equipment . The following variables were analyzed: pulsatility index (PI), resistance index (RI), peak velocity ratio (PVR), peak systolic velocity (PSV) and end diastolic velocity (EDV). To analyze the normality of the samples we used the Lillefors test, and to compare means and medians we used the Student's t-test and Mann-Whitney test according to data normality, with the level of significance set at 95%. RESULTS: The median and mean values with standard deviation of the variables of the ophthalmic artery Dopplervelocimetry group GDM and normal pregnant women were: IP=1.7±0.6 and 1.6±0.4 (p=0.7); IR=0.7 and 0.7 (p=0.9); RPV=0.5±0.1 and 0.5±0.1 (p=0.1), PSV=33.6 and 31.9 cm/sec (p=0.7); VDF=6.3 and 7.9 cm/sec (p=0.4). There was no significant difference in the means and medians of these variables between the two groups of pregnant women. CONCLUSIONS: The ophthalmic artery hemodynamic patterns, analyzed by means of a Doppler technique remained unchanged in the group of pregnant women with GDM compared to the group of normal pregnant women, suggesting that the time of exposure to the disease during pregnancy was too short to cause significant vascular disorders in the central territory.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):488-493
DOI 10.1590/S0100-72032012001100002
PURPOSE: To identify the accuracy of urinalysis in the diagnosis of urinary tract infection in pregnant women at high risk. METHODS: a prospective, cross-sectional study was conducted on 164 pregnant women admitted to the high-risk the ward of the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) during the period from January to June 2011. Patients who had been taking antibiotics in the last ten days were excluded. All patients were subjected to simple urine tests and urine culture at the beginning of their admission. The agreement between the results of the examinations was evaluated by Kappa indices (K), and accuracy, sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values were also determined. RESULTS: When only the presence of pus cells in urinalysis was used as a diagnostic criterion suggesting bacteriuria, there was a poor agreement when compared to uroculture (K=0.16). Accuracy was 61%, sensitivity 62.5%, and specificity 60.6%. PPV was 27.78% and NPV was 87%. CONCLUSION: The presence of alteration of urinalysis does not necessarily indicate an ongoing urinary tract infection, with urine culture being necessary. However, when urinalysis data are normal, uroculture may be avoided.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):488-493
DOI 10.1590/S0100-72032012001100002
PURPOSE: To identify the accuracy of urinalysis in the diagnosis of urinary tract infection in pregnant women at high risk. METHODS: a prospective, cross-sectional study was conducted on 164 pregnant women admitted to the high-risk the ward of the Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) during the period from January to June 2011. Patients who had been taking antibiotics in the last ten days were excluded. All patients were subjected to simple urine tests and urine culture at the beginning of their admission. The agreement between the results of the examinations was evaluated by Kappa indices (K), and accuracy, sensitivity, specificity, and positive (PPV) and negative (NPV) predictive values were also determined. RESULTS: When only the presence of pus cells in urinalysis was used as a diagnostic criterion suggesting bacteriuria, there was a poor agreement when compared to uroculture (K=0.16). Accuracy was 61%, sensitivity 62.5%, and specificity 60.6%. PPV was 27.78% and NPV was 87%. CONCLUSION: The presence of alteration of urinalysis does not necessarily indicate an ongoing urinary tract infection, with urine culture being necessary. However, when urinalysis data are normal, uroculture may be avoided.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):494-498
DOI 10.1590/S0100-72032012001100003
PURPOSE: To describe trends in prevalence, indicators of care and pregnancy outcomes for women with pre-existing type I or type II diabetes. METHODS: Cohort study of all consecutive singleton pregnancies complicated by pre-existing type I or type II diabetes followed from 2004 to 2011 at a tertiary perinatal care centre (n=194). We collected data from the medical records and described trends in demographics, clinical history, indicators of care before or during pregnancy and glycaemic control. We also studied perinatal outcomes, including gestational age at delivery, mode of delivery, and birthweight. RESULTS: The overall incidence of pregestational diabetes was 4.4 per 1000, with no significant changes throughout the study period. The number of type 2 diabetes cases also remained constant. In 67% of cases delivery occurred after 37 weeks (maximum 80% in 2010 - 11). During this period there was a significant reduction in rates of elective caesarean section (p=0.03) and in the incidence of large infants for gestational age (p=0.04). Indicators of glycaemic control were favorable throughout pregnancy, with no significant trends detected during the study period. However, preconceptional care indicators were substandard, with no significant improvement. CONCLUSIONS: A multidisciplinary approach to diabetic management and obstetric practice contributed to adequate glycaemic control throughout pregnancy and to improved pregnancy outcomes. Preconceptional care remains a key challenge.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):494-498
DOI 10.1590/S0100-72032012001100003
PURPOSE: To describe trends in prevalence, indicators of care and pregnancy outcomes for women with pre-existing type I or type II diabetes. METHODS: Cohort study of all consecutive singleton pregnancies complicated by pre-existing type I or type II diabetes followed from 2004 to 2011 at a tertiary perinatal care centre (n=194). We collected data from the medical records and described trends in demographics, clinical history, indicators of care before or during pregnancy and glycaemic control. We also studied perinatal outcomes, including gestational age at delivery, mode of delivery, and birthweight. RESULTS: The overall incidence of pregestational diabetes was 4.4 per 1000, with no significant changes throughout the study period. The number of type 2 diabetes cases also remained constant. In 67% of cases delivery occurred after 37 weeks (maximum 80% in 2010 - 11). During this period there was a significant reduction in rates of elective caesarean section (p=0.03) and in the incidence of large infants for gestational age (p=0.04). Indicators of glycaemic control were favorable throughout pregnancy, with no significant trends detected during the study period. However, preconceptional care indicators were substandard, with no significant improvement. CONCLUSIONS: A multidisciplinary approach to diabetic management and obstetric practice contributed to adequate glycaemic control throughout pregnancy and to improved pregnancy outcomes. Preconceptional care remains a key challenge.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):499-504
DOI 10.1590/S0100-72032012001100004
PURPOSE: To detect the presence of Human Cytomegalovirus (HCMV) and Herpes Simplex Virus type 2 (HSV-2) DNA in cervical samples from women assisted in a primary health care clinic in the city of Coari, Amazonas, Brazil. METHODS: Participated in this study 361 sexually active women between 18 and 78 years. They were been assisted in a Basic Health Care Clinic for routine gynecological exam. The cervical samples were collected using endocervical brush. The viruses were detected using real-time Polymerase Chain Reaction (PCR) technique. RESULTS: Mean age was 36.4 years (standard deviation (SD)=13.4). HCMV DNA was found in cervical samples from 30 women (8.3%; IC95% 5.8 - 11.8) and HSV 2 DNA in 2 women (0.6%; IC95% 0.1 - 2.2). Two women related being HIV positive, one of them infected with HCMV. There were no statistically significant associations between infections by the pathogens studied and socioeconomic, clinical or behavioral variables. CONCLUSIONS: The prevalence of the HCMV infection found in the sample points to the need for screening of the virus during pregnancy and surveillance in immunocompromised patients. The low prevalence of HSV-2 found is probably due to the fact that cervical sampling is not appropriate for this type of study because of the characteristics of viral biology related to neurovirulence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):499-504
DOI 10.1590/S0100-72032012001100004
PURPOSE: To detect the presence of Human Cytomegalovirus (HCMV) and Herpes Simplex Virus type 2 (HSV-2) DNA in cervical samples from women assisted in a primary health care clinic in the city of Coari, Amazonas, Brazil. METHODS: Participated in this study 361 sexually active women between 18 and 78 years. They were been assisted in a Basic Health Care Clinic for routine gynecological exam. The cervical samples were collected using endocervical brush. The viruses were detected using real-time Polymerase Chain Reaction (PCR) technique. RESULTS: Mean age was 36.4 years (standard deviation (SD)=13.4). HCMV DNA was found in cervical samples from 30 women (8.3%; IC95% 5.8 - 11.8) and HSV 2 DNA in 2 women (0.6%; IC95% 0.1 - 2.2). Two women related being HIV positive, one of them infected with HCMV. There were no statistically significant associations between infections by the pathogens studied and socioeconomic, clinical or behavioral variables. CONCLUSIONS: The prevalence of the HCMV infection found in the sample points to the need for screening of the virus during pregnancy and surveillance in immunocompromised patients. The low prevalence of HSV-2 found is probably due to the fact that cervical sampling is not appropriate for this type of study because of the characteristics of viral biology related to neurovirulence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):505-510
DOI 10.1590/S0100-72032012001100005
PURPOSE: To investigate the effect of adding biofeedback (BF) to the training of pelvic floor muscles (PFMT) for the treatment of stress urinary incontinence (SUI). METHODS: A prospective pilot study, randomized and controlled with women with SUI without sphincter deficiency, detected by urodynamic study and who performed the correct PFM contraction. Women with neuromuscular disorders and grade III and IV genital prolapse were excluded. Forty women were randomized into a Control Group and BF Group. The PFMT protocol with BF equipment consisted of three sets of ten slow contractions (tonic), with a holding time of six to eight seconds at each contraction followed by a rest period of equal duration. After each sustained contraction, they performed three to four fast contractions (phasic) in the supine and standing position twice a week, for a total of 12 sessions. We evaluated the effect of adding BF to PFMT on quality of life using King's Health Questionnaire (KHQ) regarding urinary symptoms based on a voiding diary and regarding the function of pelvic floor muscles by digital palpation. The evaluation was performed initially and after 12 treatment sessions. Data are reported as mean and standard deviation. The Mann-Whitney test was used for the analysis of homogeneity and to determine differences between groups, and the Wilcoxon test was used to determine possible differences between the times of observation, with the level of significance set at 0.05. RESULTS: A significant decrease in the scores of the domains assessed by the KHQ was observed in the comparison between groups, except for the general health domain (BF Group: 32.8±26.9 versus Control Group: 48.4±29.5, p<0.13). Accordingly, there was improvement in PFM function after treatment in the BF Group, regarding power (4.3±0.8, p= 0.001), endurance (6.0±2.2, p<0.001) and fast (9.3±1.9, p=0.001). When comparing the groups, the BF Group showed a positive result regarding power (BF Group 4.3±0.8 versus Control Group 2.5±0.9, p<0.001), endurance (6.0±2.2 BF Group versus Control Group 2.7±1.9, p<0.001) and fast (BF Group 9.3±1.9 versus Control Group 4.6 ± 3.2, p<0.001). Reduction of nocturnal urinary frequency (1.2±1.2 versus 0.7±0.9, p=0.02) and of effort urine loss (1.5±1.4 versus 0.6±0.8, p=0.001) was observed in the BF Group. CONCLUSION: The addition of BF to the PFMT for the treatment of SUI, applied according to the protocol described, improved PFM function, reduced urinary symptoms, and improved of the quality of life.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):505-510
DOI 10.1590/S0100-72032012001100005
PURPOSE: To investigate the effect of adding biofeedback (BF) to the training of pelvic floor muscles (PFMT) for the treatment of stress urinary incontinence (SUI). METHODS: A prospective pilot study, randomized and controlled with women with SUI without sphincter deficiency, detected by urodynamic study and who performed the correct PFM contraction. Women with neuromuscular disorders and grade III and IV genital prolapse were excluded. Forty women were randomized into a Control Group and BF Group. The PFMT protocol with BF equipment consisted of three sets of ten slow contractions (tonic), with a holding time of six to eight seconds at each contraction followed by a rest period of equal duration. After each sustained contraction, they performed three to four fast contractions (phasic) in the supine and standing position twice a week, for a total of 12 sessions. We evaluated the effect of adding BF to PFMT on quality of life using King's Health Questionnaire (KHQ) regarding urinary symptoms based on a voiding diary and regarding the function of pelvic floor muscles by digital palpation. The evaluation was performed initially and after 12 treatment sessions. Data are reported as mean and standard deviation. The Mann-Whitney test was used for the analysis of homogeneity and to determine differences between groups, and the Wilcoxon test was used to determine possible differences between the times of observation, with the level of significance set at 0.05. RESULTS: A significant decrease in the scores of the domains assessed by the KHQ was observed in the comparison between groups, except for the general health domain (BF Group: 32.8±26.9 versus Control Group: 48.4±29.5, p<0.13). Accordingly, there was improvement in PFM function after treatment in the BF Group, regarding power (4.3±0.8, p= 0.001), endurance (6.0±2.2, p<0.001) and fast (9.3±1.9, p=0.001). When comparing the groups, the BF Group showed a positive result regarding power (BF Group 4.3±0.8 versus Control Group 2.5±0.9, p<0.001), endurance (6.0±2.2 BF Group versus Control Group 2.7±1.9, p<0.001) and fast (BF Group 9.3±1.9 versus Control Group 4.6 ± 3.2, p<0.001). Reduction of nocturnal urinary frequency (1.2±1.2 versus 0.7±0.9, p=0.02) and of effort urine loss (1.5±1.4 versus 0.6±0.8, p=0.001) was observed in the BF Group. CONCLUSION: The addition of BF to the PFMT for the treatment of SUI, applied according to the protocol described, improved PFM function, reduced urinary symptoms, and improved of the quality of life.