Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):446-454
DOI 10.1590/SO100-720320150005264
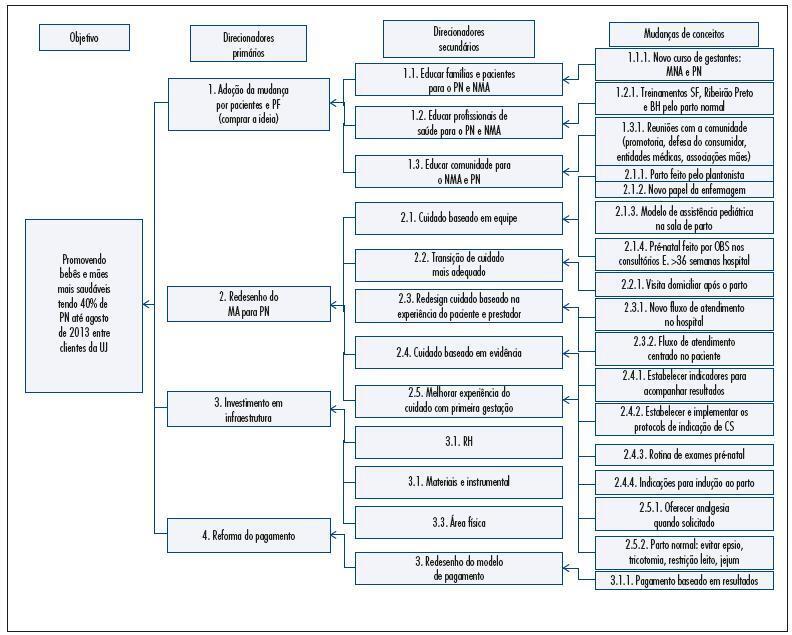
To reduce the percentage of cesareans among pregnant women at UNIMED Jaboticabal by redesigning the care delivery model.
Descriptive study conducted at an institution in São Paulo State starting in 2012 to propose the redesign of the care mode based on Continued Improvement Science adapted to the health area. To measure the results of changes we selected nine indicators and their targets.
The percentage of natural births reached the target of 40% after seven months of implementation of the interventions. The percentage of natural births reached 66% among pregnant women in SUS. The perinatal mortality rate decreased by 25% from 2012 to 2014, and the prematurity rate was 3 per 100 live births in 2014. The percentage of pregnant women from UNIMED with six or more prenatal consultations reached 95%. The hospital costs for childbirth care decreased by 27% compared to 2012 and 2013. This reduction was not sustainable and the per capita cost returned to the same level in 2014. The remuneration of all obstetricians increased by 72% from 2012 to 2014.Unimed's costs attributed to the neonatal intensive care unit (NICU) decreased by 61% from 2012 to 2013. The cost was the same for 2013 as it was for 2014 while the admission rate among newborns at UNIMED decreased by 55%. The percentage of pregnant women participating in courses to prepare for birth did not reach the goal set at 80%. The percentage of pregnant women satisfied and very satisfied with care delivery reached 86%.
This project achieved its objectives by reducing the percentage of C-sections among pregnant women of UNIMED Jaboticabal representing a concrete example of achieving the Triple Aim in health: to improve the experience of care and the health outcomes of populations and individuals and to perform these two tasks at a lower cost.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):446-454
DOI 10.1590/SO100-720320150005264
To reduce the percentage of cesareans among pregnant women at UNIMED Jaboticabal by redesigning the care delivery model.
Descriptive study conducted at an institution in São Paulo State starting in 2012 to propose the redesign of the care mode based on Continued Improvement Science adapted to the health area. To measure the results of changes we selected nine indicators and their targets.
The percentage of natural births reached the target of 40% after seven months of implementation of the interventions. The percentage of natural births reached 66% among pregnant women in SUS. The perinatal mortality rate decreased by 25% from 2012 to 2014, and the prematurity rate was 3 per 100 live births in 2014. The percentage of pregnant women from UNIMED with six or more prenatal consultations reached 95%. The hospital costs for childbirth care decreased by 27% compared to 2012 and 2013. This reduction was not sustainable and the per capita cost returned to the same level in 2014. The remuneration of all obstetricians increased by 72% from 2012 to 2014.Unimed's costs attributed to the neonatal intensive care unit (NICU) decreased by 61% from 2012 to 2013. The cost was the same for 2013 as it was for 2014 while the admission rate among newborns at UNIMED decreased by 55%. The percentage of pregnant women participating in courses to prepare for birth did not reach the goal set at 80%. The percentage of pregnant women satisfied and very satisfied with care delivery reached 86%.
This project achieved its objectives by reducing the percentage of C-sections among pregnant women of UNIMED Jaboticabal representing a concrete example of achieving the Triple Aim in health: to improve the experience of care and the health outcomes of populations and individuals and to perform these two tasks at a lower cost.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):460-466
DOI 10.1590/SO100-720320150005361
To evaluate the effectiveness of an illustrated home exercise guide targeting the pelvic floor muscles in promoting urinary continence during pregnancy.
A randomized clinical trial was performed with 87 participants, evaluated six times during pregnancy and divided into three groups: Gsup, supervised; Gobs, not supervised, and Gref, women who did not perform the home exercises program. A miction diary and perineometry were used to evaluate urinary incontinence (primary outcome) and pelvic floor muscle strength (secondary outcome), respectively. The Kruskal-Wallis test with post hoc Dunn's and chi-square and Z tests with Bonferroni correction were used for continuous variables and proportions, respectively, with the level of significance set at 5%.
At the end of the study, 6.9% of pregnant women in the Gsup and Gobs had urinary incontinence, while 96.6% of Gref women were incontinent. Regarding pelvic floor muscle function, Gsup and Gobs had mean contractions of 10 and 8.9 cmH2O, respectively, while Gref had a value of 4.7 cmH2O. Both results were significant.
An illustrated home exercise guide targeting the pelvic floor muscles is effective in promoting urinary continence during pregnancy, even without permanent supervision.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):460-466
DOI 10.1590/SO100-720320150005361
To evaluate the effectiveness of an illustrated home exercise guide targeting the pelvic floor muscles in promoting urinary continence during pregnancy.
A randomized clinical trial was performed with 87 participants, evaluated six times during pregnancy and divided into three groups: Gsup, supervised; Gobs, not supervised, and Gref, women who did not perform the home exercises program. A miction diary and perineometry were used to evaluate urinary incontinence (primary outcome) and pelvic floor muscle strength (secondary outcome), respectively. The Kruskal-Wallis test with post hoc Dunn's and chi-square and Z tests with Bonferroni correction were used for continuous variables and proportions, respectively, with the level of significance set at 5%.
At the end of the study, 6.9% of pregnant women in the Gsup and Gobs had urinary incontinence, while 96.6% of Gref women were incontinent. Regarding pelvic floor muscle function, Gsup and Gobs had mean contractions of 10 and 8.9 cmH2O, respectively, while Gref had a value of 4.7 cmH2O. Both results were significant.
An illustrated home exercise guide targeting the pelvic floor muscles is effective in promoting urinary continence during pregnancy, even without permanent supervision.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):467-472
DOI 10.1590/SO100-720320150005440
The administration of a single-course antenatal corticosteroid treatment is recommended for pregnant women between 24 and 34 weeks with risk of premature birth. The maximum effect is achieved when antenatal corticosteroids are administered between 24h and 7 days before delivery. The objective of this study was to evaluate the occurrence of birth within seven days of corticosteroid therapy in major obstetric situations with risk of preterm birth
Retrospective cohort study including 209 pregnant women hospitalized in risk of preterm delivery, submitted to corticosteroid therapy for fetal lung maturation. The study was carried out between January 2012 and March 2014 at a university hospital. Main outcome measure was the number of women who delivered within 7 da ys after antenatal corticosteroid administration. Two groups were defined according to the reason for starting corticosteroids: threatened preterm labour (Group APPT) and other indications for corticosteroid therapy (Group RPPT). A Kaplan-Meier survival analysis was performed and a p value <0.05 was considered statistically significant.
46.4% (n=97) of pregnant women gave birth in the seven days following corticosteroid administration. Delivery within 7 days occurred more frequently on group 2 in comparison to group 1 (57.3 versus42.4%; p=0.001). There is a statistically significant difference between the survival curve for groups 1 and 2, with a hazard ratio for delivery within 7 days 1.71 times higher for group 2 (95%CI 1.23-2.37; p<0.001)
It can be concluded that the probability of an event (birth within 7 days after corticosteroids) is smaller in the group of pregnant women admitted in the context of threatened preterm labor than for other indications. The use of corticosteroids in pregnant women admitted for suspected preterm labor should be subject to rigorous clinical evaluation
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):467-472
DOI 10.1590/SO100-720320150005440
The administration of a single-course antenatal corticosteroid treatment is recommended for pregnant women between 24 and 34 weeks with risk of premature birth. The maximum effect is achieved when antenatal corticosteroids are administered between 24h and 7 days before delivery. The objective of this study was to evaluate the occurrence of birth within seven days of corticosteroid therapy in major obstetric situations with risk of preterm birth
Retrospective cohort study including 209 pregnant women hospitalized in risk of preterm delivery, submitted to corticosteroid therapy for fetal lung maturation. The study was carried out between January 2012 and March 2014 at a university hospital. Main outcome measure was the number of women who delivered within 7 da ys after antenatal corticosteroid administration. Two groups were defined according to the reason for starting corticosteroids: threatened preterm labour (Group APPT) and other indications for corticosteroid therapy (Group RPPT). A Kaplan-Meier survival analysis was performed and a p value <0.05 was considered statistically significant.
46.4% (n=97) of pregnant women gave birth in the seven days following corticosteroid administration. Delivery within 7 days occurred more frequently on group 2 in comparison to group 1 (57.3 versus42.4%; p=0.001). There is a statistically significant difference between the survival curve for groups 1 and 2, with a hazard ratio for delivery within 7 days 1.71 times higher for group 2 (95%CI 1.23-2.37; p<0.001)
It can be concluded that the probability of an event (birth within 7 days after corticosteroids) is smaller in the group of pregnant women admitted in the context of threatened preterm labor than for other indications. The use of corticosteroids in pregnant women admitted for suspected preterm labor should be subject to rigorous clinical evaluation
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):480-485
DOI 10.1590/SO100-720320150005279
To determine the prevalence of HPV-induced lesions in the anal canal of women with cervical intraepithelial neoplasia (CIN) grade 2/3.
A cross-sectional study was carried out from December 2008 to June 2009, in Pernambuco, northeastern Brazil. Only women with grade 2/3 CIN were included, and those who could not undergo anoscopy during their first visit were excluded. A cyttobrush was used for sample collection in order to identify HPV DNA through PCR and anal cytology. An anal biopsy was obtained in cases of abnormal anal cytology or major alterations in high resolution anoscopy (HRA).
Thirty-two percent (n=37/115) of HRA were normal and 63.5% (n=73/115) showed acetowhite epithelium. Twenty-two percent (n=26/115) of anal cytologies were abnormal. Among the latter, 12.2% (n=14/26) were low-grade anal intraepithelial lesions and 3.4% (n=4/26) were high-grade anal intraepithelial lesions. Twenty-two anal biopsies were performed, 13.7% of which (n=3/22) were grade 2 anal intraepithelial neoplasia (AIN2) and 9% (n=2/22) were grade 3 AIN. Th HPV DNA was identified in 72.1% of cases (n=83/115).
Women with CIN grade 2/3 showed a high prevalence of anal HPV infection and HPV-induced lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):480-485
DOI 10.1590/SO100-720320150005279
To determine the prevalence of HPV-induced lesions in the anal canal of women with cervical intraepithelial neoplasia (CIN) grade 2/3.
A cross-sectional study was carried out from December 2008 to June 2009, in Pernambuco, northeastern Brazil. Only women with grade 2/3 CIN were included, and those who could not undergo anoscopy during their first visit were excluded. A cyttobrush was used for sample collection in order to identify HPV DNA through PCR and anal cytology. An anal biopsy was obtained in cases of abnormal anal cytology or major alterations in high resolution anoscopy (HRA).
Thirty-two percent (n=37/115) of HRA were normal and 63.5% (n=73/115) showed acetowhite epithelium. Twenty-two percent (n=26/115) of anal cytologies were abnormal. Among the latter, 12.2% (n=14/26) were low-grade anal intraepithelial lesions and 3.4% (n=4/26) were high-grade anal intraepithelial lesions. Twenty-two anal biopsies were performed, 13.7% of which (n=3/22) were grade 2 anal intraepithelial neoplasia (AIN2) and 9% (n=2/22) were grade 3 AIN. Th HPV DNA was identified in 72.1% of cases (n=83/115).
Women with CIN grade 2/3 showed a high prevalence of anal HPV infection and HPV-induced lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):486-491
DOI 10.1590/SO100-720320150005347
To determine adherence to dual contraception using depot-medroxyprogesterone acetate (DMPA) and condom among HIV-infected women.
A cross-sectional study carried out from December 2013 to September 2014 at a local reference center, with application of questionnaire elaborated after Delphi panel and content validation to 114 HIV(+) women aged 15 to 49 years, using DMPA plus condom for contraception.
Mean age was 33.2±7.2 years, mean time since HIV detection was 8.1±5.2 years, mean time of antiretroviral use was 6.8±5 years and mean CD4 cells/mm count was 737.6±341.1. Sexual HIV acquisition was reported by 98.2% (112/114), antiretroviral use by 85.9% (98/114), and 77.7% (84/114) had a CD4>500/mm count. Having a single sex partner was reported by 78.9% (90/114), with HIV serodiscordance in 41.2% (47/114) of couples, 21.9% did not know the serological status of their partner and in 37.7% of cases (43/114) the partner was unaware of the HIV(+) status of the woman. The last pregnancy was unplanned in 71.9% of cases (82/114) and 14.9% of the women had become pregnant the year before, with pregnancy being unplanned in 70.5% (12/17) of cases. Current use of DMPA was reported by 64.9% (74/114), with genital bleeding in 48.2% (55/114) and weight gain in 67.5% (77/114). Use of a male condom was reported by 62.2% of the subjects (71/114). Three reported that they always used a female condom and ten that they eventually used it. Unprotected vaginal sex was reported by 37.7% (43/114) and unprotected anal intercourse was reported by 32.4% (37/114). Partner resistance to use a condom occurred in 30.7% of cases (35/114). Dual contraception using DMPA with condom was reported by 42.9% (49/114). A partner who resisted wearing a condom was associated with poor adhesion (PR=0.3; 95%CI 0.2-0.7; p<0.001). A partner who was unaware that a woman was infected with HIV favored adherence (PR=1.8; 95%CI 1.2-2.7; p=0.013).
The percentage of dual contraception using DMPA plus condom was 42.9%, maintaining unplanned pregnancies and unprotected sex. Resistance of partners to use a condom increased three times the chance of a woman not adhering to dual contraception, and the partner not knowing women's HIV infection almost doubled the chance to adhere to safe contraception. Goals: to offer new hormonal contraceptives and to involve the partners in contraception and serologic detection tests.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(10):486-491
DOI 10.1590/SO100-720320150005347
To determine adherence to dual contraception using depot-medroxyprogesterone acetate (DMPA) and condom among HIV-infected women.
A cross-sectional study carried out from December 2013 to September 2014 at a local reference center, with application of questionnaire elaborated after Delphi panel and content validation to 114 HIV(+) women aged 15 to 49 years, using DMPA plus condom for contraception.
Mean age was 33.2±7.2 years, mean time since HIV detection was 8.1±5.2 years, mean time of antiretroviral use was 6.8±5 years and mean CD4 cells/mm count was 737.6±341.1. Sexual HIV acquisition was reported by 98.2% (112/114), antiretroviral use by 85.9% (98/114), and 77.7% (84/114) had a CD4>500/mm count. Having a single sex partner was reported by 78.9% (90/114), with HIV serodiscordance in 41.2% (47/114) of couples, 21.9% did not know the serological status of their partner and in 37.7% of cases (43/114) the partner was unaware of the HIV(+) status of the woman. The last pregnancy was unplanned in 71.9% of cases (82/114) and 14.9% of the women had become pregnant the year before, with pregnancy being unplanned in 70.5% (12/17) of cases. Current use of DMPA was reported by 64.9% (74/114), with genital bleeding in 48.2% (55/114) and weight gain in 67.5% (77/114). Use of a male condom was reported by 62.2% of the subjects (71/114). Three reported that they always used a female condom and ten that they eventually used it. Unprotected vaginal sex was reported by 37.7% (43/114) and unprotected anal intercourse was reported by 32.4% (37/114). Partner resistance to use a condom occurred in 30.7% of cases (35/114). Dual contraception using DMPA with condom was reported by 42.9% (49/114). A partner who resisted wearing a condom was associated with poor adhesion (PR=0.3; 95%CI 0.2-0.7; p<0.001). A partner who was unaware that a woman was infected with HIV favored adherence (PR=1.8; 95%CI 1.2-2.7; p=0.013).
The percentage of dual contraception using DMPA plus condom was 42.9%, maintaining unplanned pregnancies and unprotected sex. Resistance of partners to use a condom increased three times the chance of a woman not adhering to dual contraception, and the partner not knowing women's HIV infection almost doubled the chance to adhere to safe contraception. Goals: to offer new hormonal contraceptives and to involve the partners in contraception and serologic detection tests.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):397-401
DOI 10.1590/SO100-720320150005353
To evaluate the frequency and risk factors for the development of phantom breast syndrome in patients submitted to mastectomy after breast cancer treatment.
A cohort study of women undergoing treatment at the Hospital of Cancer III, National Cancer Institute José Alencar Gomes da Silva (INCA) from September 2008 to June 2009. PBS was considered based on report of phantom breast sensation and/or phantom breast pain. The study was approved by the Research Ethics Committee of the INCA (015/08). Descriptive analysis using absolute and relative frequency was performed. To evaluate the association between PBS and potential risk factors, univariate analysis was performed by means of odds ratios (OR) with respective 95% confidence intervals (95%CI).
A total of 88 patients were included. The frequency of PBS observed was 44.3 at 45 days (first follow-up) and 18.2% at 2 years (last follow-up). Most women reported phantom breast syndrome in all segments (37.1; 30.1 and 22%). During the six month follow-up, women under the age of 60 years had a 3.93 times higher risk of PBS (OR=3.9; 95%CI 1.4-10.5) and those with higher education (8 years or more of study) had a higher risk of developing PBS (OR=2.6; 95%CI 1.01-6.8).
The study population had a high frequency of PBS, which decreased over postoperative follow-up. Its occurrence after six months was higher among younger and more educated women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):397-401
DOI 10.1590/SO100-720320150005353
To evaluate the frequency and risk factors for the development of phantom breast syndrome in patients submitted to mastectomy after breast cancer treatment.
A cohort study of women undergoing treatment at the Hospital of Cancer III, National Cancer Institute José Alencar Gomes da Silva (INCA) from September 2008 to June 2009. PBS was considered based on report of phantom breast sensation and/or phantom breast pain. The study was approved by the Research Ethics Committee of the INCA (015/08). Descriptive analysis using absolute and relative frequency was performed. To evaluate the association between PBS and potential risk factors, univariate analysis was performed by means of odds ratios (OR) with respective 95% confidence intervals (95%CI).
A total of 88 patients were included. The frequency of PBS observed was 44.3 at 45 days (first follow-up) and 18.2% at 2 years (last follow-up). Most women reported phantom breast syndrome in all segments (37.1; 30.1 and 22%). During the six month follow-up, women under the age of 60 years had a 3.93 times higher risk of PBS (OR=3.9; 95%CI 1.4-10.5) and those with higher education (8 years or more of study) had a higher risk of developing PBS (OR=2.6; 95%CI 1.01-6.8).
The study population had a high frequency of PBS, which decreased over postoperative follow-up. Its occurrence after six months was higher among younger and more educated women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):421-427
DOI 10.1590/SO100-720320150005355
To evaluate the prevalence of toxoplasmosis, rubella, cytomegalovirus, hepatitis B&C and syphilis (Torchs) in a cohort pregnant women and to identify the sociodemographic, clinical and laboratory factors.
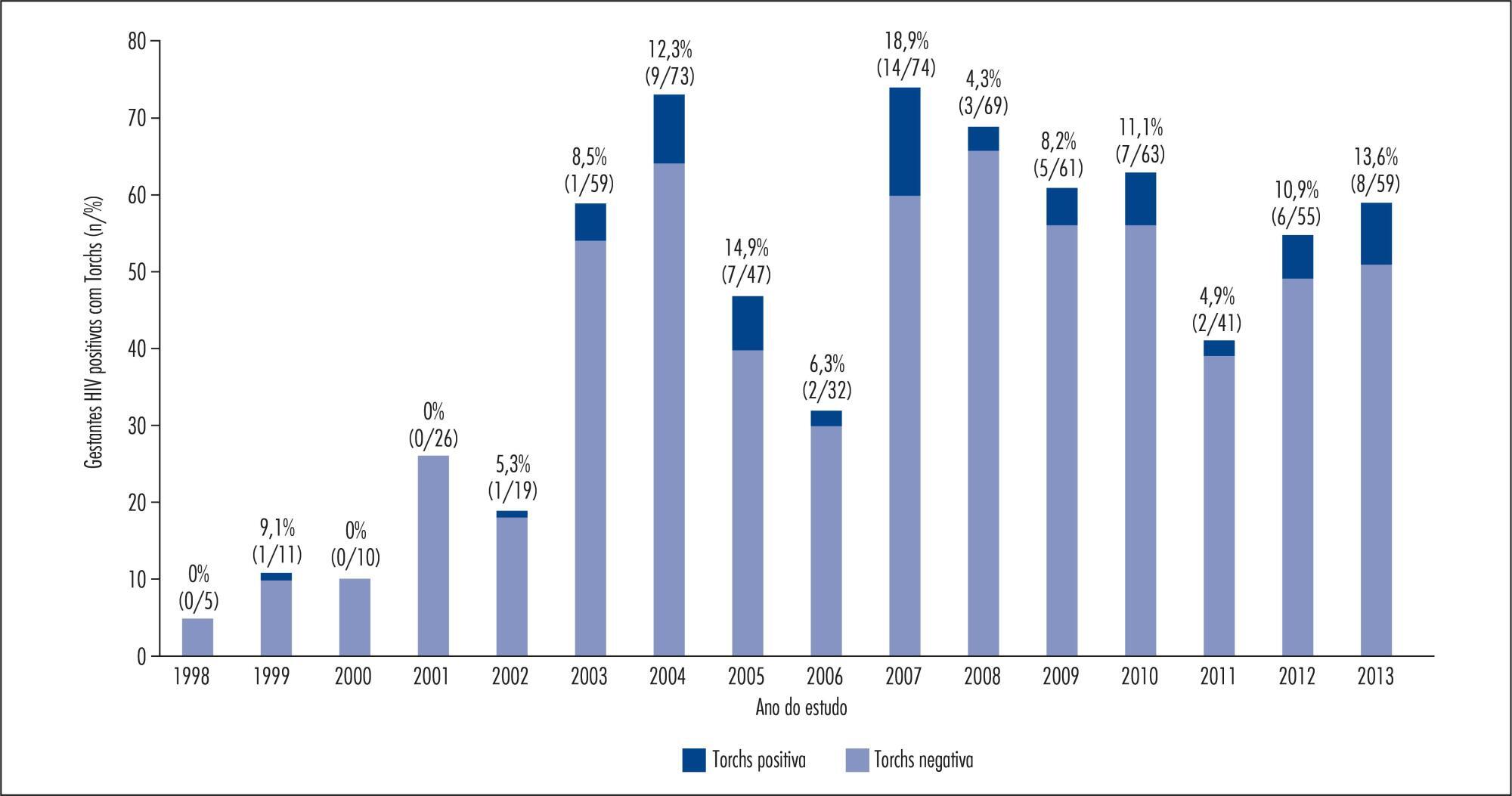
A total of 1,573 HIV-infected pregnant women from a Brazilian metropolitan region were studied between 1998 and 2013. The results of serological tests were available for 704 (44.8%) pregnant women. Pregnant women were considered to be Torchs positive (Gtp) when they had positive results for at least one of these infections, and to be Torchs negative (Gtn) when they had negative results for all of them. Maternal covariables were: age, marital status, educational level, time and mode of infection, CD4 lymphocyte count, viral load at delivery, and use of antiretroviral therapy (ARV). Neonatal covariables were: HIV infection, prematurity, low birth weight, neonatal complications, abortion and neonatal death. Odds ratios with 95% confidence interval were used to quantify the association between maternal and neonatal variables and the presence of Torchs.
Among 704 pregnant women, 70 (9.9%; 95%CI 7.8-12.4) had positive serological tests for any Torchs factor. The individual prevalence rates were: 1.5% (10/685) for toxoplasmosis; 1.3% (8/618) for rubella; 1.3% (8/597) for cytomegalovirus; 0.9% (6/653) for hepatitis B and 3.7% (20/545) for hepatitis C; and 3.8% (25/664) for syphilis. The HIV Vertical HIV transmission was 4.6% among Gtp pregnant women and 1.2% among Gtn women. Antiretroviral therapy (ARV), vertical transmission, low birth weight and neonatal complications were significantly associated with Torchs positivity in univariate analysis.
The Torchs prevalence found in the study was high for some infections. These findings emphasize the need to promote serological Torchs screening for all pregnant women, especially HIV-infected women, so that an early diagnosis can be made and treatment interventions can be implemented to prevent vertical HIV transmission.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):421-427
DOI 10.1590/SO100-720320150005355
To evaluate the prevalence of toxoplasmosis, rubella, cytomegalovirus, hepatitis B&C and syphilis (Torchs) in a cohort pregnant women and to identify the sociodemographic, clinical and laboratory factors.
A total of 1,573 HIV-infected pregnant women from a Brazilian metropolitan region were studied between 1998 and 2013. The results of serological tests were available for 704 (44.8%) pregnant women. Pregnant women were considered to be Torchs positive (Gtp) when they had positive results for at least one of these infections, and to be Torchs negative (Gtn) when they had negative results for all of them. Maternal covariables were: age, marital status, educational level, time and mode of infection, CD4 lymphocyte count, viral load at delivery, and use of antiretroviral therapy (ARV). Neonatal covariables were: HIV infection, prematurity, low birth weight, neonatal complications, abortion and neonatal death. Odds ratios with 95% confidence interval were used to quantify the association between maternal and neonatal variables and the presence of Torchs.
Among 704 pregnant women, 70 (9.9%; 95%CI 7.8-12.4) had positive serological tests for any Torchs factor. The individual prevalence rates were: 1.5% (10/685) for toxoplasmosis; 1.3% (8/618) for rubella; 1.3% (8/597) for cytomegalovirus; 0.9% (6/653) for hepatitis B and 3.7% (20/545) for hepatitis C; and 3.8% (25/664) for syphilis. The HIV Vertical HIV transmission was 4.6% among Gtp pregnant women and 1.2% among Gtn women. Antiretroviral therapy (ARV), vertical transmission, low birth weight and neonatal complications were significantly associated with Torchs positivity in univariate analysis.
The Torchs prevalence found in the study was high for some infections. These findings emphasize the need to promote serological Torchs screening for all pregnant women, especially HIV-infected women, so that an early diagnosis can be made and treatment interventions can be implemented to prevent vertical HIV transmission.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):428-433
DOI 10.1590/SO100-720320150005283
Evaluation of maternal, obstetrics e neonatal features in both spontaneous preterm births (PTB) with or without preterm premature rupture of membranes (PPROM).
Retrospective study of single fetus pregnancies with PTB between 2003 and 2012. Inclusion criteria: PTB associated with ou without PPROM. Exclusion criterias: PTB by medical indication due to fetal/maternal disease and all non accessible or incomplete clinical files. Different characteristics were compared between two groups of PTB: spontaneous PTB without PPROM (sPTB) versus PPROM. Kolmogorov-Smirnov, Levene, χ2, t Student and Mann-Withney tests were used for statistical analysis.
From 2,393 PTB of single fetus, 1,432 files were analysed, from which 596 were sPTB and 836 PPROM. The socioeconomic conditions were similar in both groups. Multiparity (50.7versus 40.3%), personal history of previous PTB (20.8 versus 10.2%), cervical length (18.2 versus 27.2 mm), lower body index mass (23.4 versus 24.3 kg/m2) and higher infectious parameters (Protein C Reactive: 2.2 versus 1.2 mg/L; Leukocytes: 13.3 versus 12.4x109) were more frequent in PBTs (p<0,001). Neonatal outcomes, specially neurologic outcomes (4.7 versus 2.8%, p<0,001), were worst in PBTs.
PTB with or without PPROM has a complex etiology. From all evaluated features in our study, only maternal thinness, multiparity with a previous PTB, the cervical length and worst systemic infections parameters were significant in sPTB. This group also showed worst neonatal outcomes, specially on neurological outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):428-433
DOI 10.1590/SO100-720320150005283
Evaluation of maternal, obstetrics e neonatal features in both spontaneous preterm births (PTB) with or without preterm premature rupture of membranes (PPROM).
Retrospective study of single fetus pregnancies with PTB between 2003 and 2012. Inclusion criteria: PTB associated with ou without PPROM. Exclusion criterias: PTB by medical indication due to fetal/maternal disease and all non accessible or incomplete clinical files. Different characteristics were compared between two groups of PTB: spontaneous PTB without PPROM (sPTB) versus PPROM. Kolmogorov-Smirnov, Levene, χ2, t Student and Mann-Withney tests were used for statistical analysis.
From 2,393 PTB of single fetus, 1,432 files were analysed, from which 596 were sPTB and 836 PPROM. The socioeconomic conditions were similar in both groups. Multiparity (50.7versus 40.3%), personal history of previous PTB (20.8 versus 10.2%), cervical length (18.2 versus 27.2 mm), lower body index mass (23.4 versus 24.3 kg/m2) and higher infectious parameters (Protein C Reactive: 2.2 versus 1.2 mg/L; Leukocytes: 13.3 versus 12.4x109) were more frequent in PBTs (p<0,001). Neonatal outcomes, specially neurologic outcomes (4.7 versus 2.8%, p<0,001), were worst in PBTs.
PTB with or without PPROM has a complex etiology. From all evaluated features in our study, only maternal thinness, multiparity with a previous PTB, the cervical length and worst systemic infections parameters were significant in sPTB. This group also showed worst neonatal outcomes, specially on neurological outcomes.