-
Original Articles
Postpartum Reclassification of Glycemic Status in Women with Gestational Diabetes Mellitus and Associated Risk Factors
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):381-390
08-01-2016
Summary
Original ArticlesPostpartum Reclassification of Glycemic Status in Women with Gestational Diabetes Mellitus and Associated Risk Factors
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):381-390
08-01-2016Views183See moreAbstract
Objective
The aims of the study were to evaluate, after pregnancy, the glycemic status of women with history of gestational diabetes mellitus (GDM) and to identify clinical variables associated with the development of type 2 diabetes mellitus (T2DM), impaired fasting glucose (IFG), and impaired glucose tolerance (IGT).
Methods
Retrospective cohort of 279 women with GDM who were reevaluated with an oral glucose tolerance test (OGTT) after pregnancy. Characteristics of the index pregnancy were analyzed as risk factors for the future development of prediabetes (IFG or IGT), and T2DM.
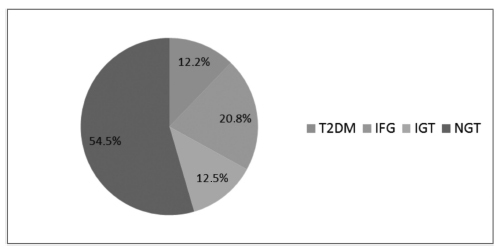
Results:
T2DM was diagnosed in 34 (12.2%) patients, IFG in 58 (20.8%), and IGT in 35 (12.5%). Women with postpartum T2DM showed more frequently a family history of T2DM, higher pre-pregnancy body mass index (BMI), lower gestational age, higher fasting and 2-hour plasma glucose levels on the OGTT at the diagnosis of GDM, higher levels of hemoglobin A1c, and a more frequent insulin requirement during pregnancy. Paternal history of T2DM (odds ratio [OR] =5.67; 95% confidence interval [95%CI] =1.64-19.59; p =0.006), first trimester fasting glucose value (OR =1.07; 95%CI =1.03-1.11; p =0.001), and insulin treatment during pregnancy (OR =15.92; 95%CI =5.54-45.71; p < 0.001) were significant independent risk factors for the development of T2DM.
Conclusion
A high rate of abnormal glucose tolerance was found in women with previous GDM. Family history of T2DM, higher pre-pregnancy BMI, early onset of GDM, higher glucose levels, and insulin requirement during pregnancy were important risk factors for the early identification of women at high risk of developing T2DM. These findings may be useful for developing preventive strategies.
Views183

This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticlesPostpartum Reclassification of Glycemic Status in Women with Gestational Diabetes Mellitus and Associated Risk Factors
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):381-390
08-01-2016Views183See moreAbstract
Objective
The aims of the study were to evaluate, after pregnancy, the glycemic status of women with history of gestational diabetes mellitus (GDM) and to identify clinical variables associated with the development of type 2 diabetes mellitus (T2DM), impaired fasting glucose (IFG), and impaired glucose tolerance (IGT).
Methods
Retrospective cohort of 279 women with GDM who were reevaluated with an oral glucose tolerance test (OGTT) after pregnancy. Characteristics of the index pregnancy were analyzed as risk factors for the future development of prediabetes (IFG or IGT), and T2DM.
Results:
T2DM was diagnosed in 34 (12.2%) patients, IFG in 58 (20.8%), and IGT in 35 (12.5%). Women with postpartum T2DM showed more frequently a family history of T2DM, higher pre-pregnancy body mass index (BMI), lower gestational age, higher fasting and 2-hour plasma glucose levels on the OGTT at the diagnosis of GDM, higher levels of hemoglobin A1c, and a more frequent insulin requirement during pregnancy. Paternal history of T2DM (odds ratio [OR] =5.67; 95% confidence interval [95%CI] =1.64-19.59; p =0.006), first trimester fasting glucose value (OR =1.07; 95%CI =1.03-1.11; p =0.001), and insulin treatment during pregnancy (OR =15.92; 95%CI =5.54-45.71; p < 0.001) were significant independent risk factors for the development of T2DM.
Conclusion
A high rate of abnormal glucose tolerance was found in women with previous GDM. Family history of T2DM, higher pre-pregnancy BMI, early onset of GDM, higher glucose levels, and insulin requirement during pregnancy were important risk factors for the early identification of women at high risk of developing T2DM. These findings may be useful for developing preventive strategies.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.