Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo85
To evaluate the role of being human immunodeficiency virus (HIV) positive for predicting the risk of recurrence in women with a cervical high grade squamous intraepithelial lesion (HSIL) diagnosis.
Retrospective observational case-control study, comprising HIV positive (case) and HIV negative (control) women in a 1:4 ratio. Women assisted by the Erasto Gaertner Hospital, between 2009-2018, with cervical HSIL diagnosis, submitted to treatment by Loop electrosurgical excision procedure (LEEP), and with a minimum follow-up of 18 months, were included. The immunological status, number and time to recurrence were analyzed, with p<0.05 considered significant. In a second analysis, only patients with free margins were evaluated.
The sample consisted of 320 women (64 cases and 256 controls). Presence of HIV, CD4 levels <200 and detectable viral load (CV) were associated with high risk of recurrence, with odds ratio (OR) of 5.4 (p<0.001/95CI:2.8-10); 3.6 (p<0.001 /IC95:0.6-21.1) and 1.8 (p=0.039 /IC95:0.3-9.3), respectively. In the sample with free margins (n=271), this risk was also higher among seropositive patients, with OR 4.18 (p=0.001/95CI:1.8-9.2).
HIV is an independent risk factor for cervical HSIL recurrence and reduced disease-free survival time. Glandular involvement, compromised margins, undetectable CV and CD4<200 also increase the risk of relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo85
To evaluate the role of being human immunodeficiency virus (HIV) positive for predicting the risk of recurrence in women with a cervical high grade squamous intraepithelial lesion (HSIL) diagnosis.
Retrospective observational case-control study, comprising HIV positive (case) and HIV negative (control) women in a 1:4 ratio. Women assisted by the Erasto Gaertner Hospital, between 2009-2018, with cervical HSIL diagnosis, submitted to treatment by Loop electrosurgical excision procedure (LEEP), and with a minimum follow-up of 18 months, were included. The immunological status, number and time to recurrence were analyzed, with p<0.05 considered significant. In a second analysis, only patients with free margins were evaluated.
The sample consisted of 320 women (64 cases and 256 controls). Presence of HIV, CD4 levels <200 and detectable viral load (CV) were associated with high risk of recurrence, with odds ratio (OR) of 5.4 (p<0.001/95CI:2.8-10); 3.6 (p<0.001 /IC95:0.6-21.1) and 1.8 (p=0.039 /IC95:0.3-9.3), respectively. In the sample with free margins (n=271), this risk was also higher among seropositive patients, with OR 4.18 (p=0.001/95CI:1.8-9.2).
HIV is an independent risk factor for cervical HSIL recurrence and reduced disease-free survival time. Glandular involvement, compromised margins, undetectable CV and CD4<200 also increase the risk of relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(6):319-324
Reporting our experience of the management and treatment of Idiopathic granulomatous mastitis (IGM) in a low-income country by describing patients characteristics and therapy with emphasis on conservative surgical excision and postoperative care as the cornerstone of treatment.
A retrospective cohort of women with histopathological diagnosis of IGM from 2014 to 2018 at Instituto Nacional Materno Perinatal in Lima, Peru. Patients' characteristics, clinical presentation, treatment, management, postoperative care, and follow-up were analyzed.
Thirty-eight patients with histopathological diagnosis of IGM were identified. Their average age was 35.9 years and 23 (60.5%) reported previous use of hormonal contraceptives. Nine (23.7%) patients had chronic mastitis with previous treatment. The time from the onset of symptoms to the first clinic consult was 5.1 months on average. Twenty-one (55.3%) patients had the lesion in the right breast, with a mean size of 6.9 cm. Conservative surgical excision was performed in all patients. Additionally, 86.8% required corticosteroids and 78.9% were treated with antibiotics. Complete remission was obtained at 141 days on average (range 44 to 292 days). Six (15.8%) women reported ipsilateral recurrence and 5 (13.2%), contralateral. The latency time was 25.5 months on average.
The conservative surgical treatment demonstrated and close follow-up made for a high cure rate, but with recurrence similar to that reported in the literature. Use of gloves is an alternative to manage post operative wounds in a low-income country. The most frequent adverse effect was breast surgical scar.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(6):319-324
Reporting our experience of the management and treatment of Idiopathic granulomatous mastitis (IGM) in a low-income country by describing patients characteristics and therapy with emphasis on conservative surgical excision and postoperative care as the cornerstone of treatment.
A retrospective cohort of women with histopathological diagnosis of IGM from 2014 to 2018 at Instituto Nacional Materno Perinatal in Lima, Peru. Patients' characteristics, clinical presentation, treatment, management, postoperative care, and follow-up were analyzed.
Thirty-eight patients with histopathological diagnosis of IGM were identified. Their average age was 35.9 years and 23 (60.5%) reported previous use of hormonal contraceptives. Nine (23.7%) patients had chronic mastitis with previous treatment. The time from the onset of symptoms to the first clinic consult was 5.1 months on average. Twenty-one (55.3%) patients had the lesion in the right breast, with a mean size of 6.9 cm. Conservative surgical excision was performed in all patients. Additionally, 86.8% required corticosteroids and 78.9% were treated with antibiotics. Complete remission was obtained at 141 days on average (range 44 to 292 days). Six (15.8%) women reported ipsilateral recurrence and 5 (13.2%), contralateral. The latency time was 25.5 months on average.
The conservative surgical treatment demonstrated and close follow-up made for a high cure rate, but with recurrence similar to that reported in the literature. Use of gloves is an alternative to manage post operative wounds in a low-income country. The most frequent adverse effect was breast surgical scar.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(1):35-42
To evaluate the outcomes of surgical treatment in patients with chemoradiotherapy (CRT)-resistant and locally advanced cervical cancer (LACC).
Patients with LACC who underwent surgery due to resistance to CRT between 2005 and 2015 were reviewed retrospectively. Disease-free survival (DFS) and overall survival (OS) related factors were analyzed.
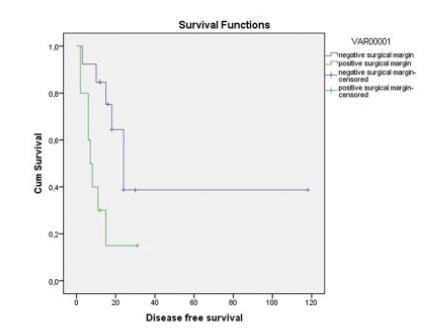
A total of 23 patients were included in the study and the median age was 51 years old. A total of 14 patients (60.8%) experienced recurrence; among these recurrences, 8 of them were local, 5 were distant, 1 was both distant and local. A total of 9 patients (39%) died. The Median DFS and OS durations were 15 and 32 months, respectively. A total of 17 patients (74%) had undergone simple hysterectomy, 4 (17%) radical hysterectomy, and 2 (9%) total pelvic exenteration. Postoperative grade 3 and 4 complications were seen in 12 patients (52%). Macroscopic tumor presence in the pathology specimen was associated with distant recurrence and positive surgical margins with local recurrence (Log-Rank test p = 0.029 and p = 0.048, respectively). The only factor associated with OS was surgical margin positivity (Log-Rank test p = 0.008). The type of surgery, grades 3 and 4 postoperative complications, brachytherapy, and tumor histology were not associated with recurrence.
In patients with LACC, hysterectomy is an option in the presence of a central residual tumor after CRT. However, the risk of grades 3 and 4 complications of performed surgery is high. The presence of macroscopic tumor in the pathology specimen and positive surgical margins are poor prognostic factors. The goal of the surgeon should be to achieve a negative surgical margin. It does not seem important if the surgery is simple or radical.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(1):35-42
To evaluate the outcomes of surgical treatment in patients with chemoradiotherapy (CRT)-resistant and locally advanced cervical cancer (LACC).
Patients with LACC who underwent surgery due to resistance to CRT between 2005 and 2015 were reviewed retrospectively. Disease-free survival (DFS) and overall survival (OS) related factors were analyzed.
A total of 23 patients were included in the study and the median age was 51 years old. A total of 14 patients (60.8%) experienced recurrence; among these recurrences, 8 of them were local, 5 were distant, 1 was both distant and local. A total of 9 patients (39%) died. The Median DFS and OS durations were 15 and 32 months, respectively. A total of 17 patients (74%) had undergone simple hysterectomy, 4 (17%) radical hysterectomy, and 2 (9%) total pelvic exenteration. Postoperative grade 3 and 4 complications were seen in 12 patients (52%). Macroscopic tumor presence in the pathology specimen was associated with distant recurrence and positive surgical margins with local recurrence (Log-Rank test p = 0.029 and p = 0.048, respectively). The only factor associated with OS was surgical margin positivity (Log-Rank test p = 0.008). The type of surgery, grades 3 and 4 postoperative complications, brachytherapy, and tumor histology were not associated with recurrence.
In patients with LACC, hysterectomy is an option in the presence of a central residual tumor after CRT. However, the risk of grades 3 and 4 complications of performed surgery is high. The presence of macroscopic tumor in the pathology specimen and positive surgical margins are poor prognostic factors. The goal of the surgeon should be to achieve a negative surgical margin. It does not seem important if the surgery is simple or radical.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(3):176-182
The aim of the present study was to describe and analyze data of 57 women with borderline ovarian tumors (BOTs) regarding histological characteristics, clinical features and treatment management at the Department of Obstetrics and Gynecology of the Universidade Estadual de Campinas (Unicamp, in the Portuguese acronym).
The present retrospective study analyzed data obtained from clinical and histopathological reports of women with BOTs treated in a single cancer center between 2010 and 2018.
A total of 57 women were included, with a mean age of 48.42 years old (15.43- 80.77), of which 30 (52.63%) were postmenopausal, and 18 (31.58%) were < 40 years old. All of the women underwent surgery. A total of 37 women (64.91%) were submitted to complete surgical staging for BOT, and none (0/57) were submitted to pelvic or paraortic lymphadenectomy. Chemotherapy was administered for two patients who recurred. The final histological diagnoses were: serous in 20 (35.09%) cases, mucinous in 26 (45.61%), seromucinous in 10 (17.54%), and endometrioid in 1 (1.75%) case. Intraoperative analyses of frozen sections were obtained in 42 (73.68%) women, of which 28 (66.67%) matched with the final diagnosis. The mean follow-up was of 42.79 months (range: 2.03-104.87 months). Regard ingthe current status of the women, 45(78.95%) are alive without disease, 2(3.51%) arealive with disease, 9 (15.79%) had their last follow-up visit > 1 year beforethe performanceof the present study but arealive, and 1 patient(1.75%) died of another cause.
Women in the present study were treated according to the current guidelines and only two patients recurred.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(3):176-182
The aim of the present study was to describe and analyze data of 57 women with borderline ovarian tumors (BOTs) regarding histological characteristics, clinical features and treatment management at the Department of Obstetrics and Gynecology of the Universidade Estadual de Campinas (Unicamp, in the Portuguese acronym).
The present retrospective study analyzed data obtained from clinical and histopathological reports of women with BOTs treated in a single cancer center between 2010 and 2018.
A total of 57 women were included, with a mean age of 48.42 years old (15.43- 80.77), of which 30 (52.63%) were postmenopausal, and 18 (31.58%) were < 40 years old. All of the women underwent surgery. A total of 37 women (64.91%) were submitted to complete surgical staging for BOT, and none (0/57) were submitted to pelvic or paraortic lymphadenectomy. Chemotherapy was administered for two patients who recurred. The final histological diagnoses were: serous in 20 (35.09%) cases, mucinous in 26 (45.61%), seromucinous in 10 (17.54%), and endometrioid in 1 (1.75%) case. Intraoperative analyses of frozen sections were obtained in 42 (73.68%) women, of which 28 (66.67%) matched with the final diagnosis. The mean follow-up was of 42.79 months (range: 2.03-104.87 months). Regard ingthe current status of the women, 45(78.95%) are alive without disease, 2(3.51%) arealive with disease, 9 (15.79%) had their last follow-up visit > 1 year beforethe performanceof the present study but arealive, and 1 patient(1.75%) died of another cause.
Women in the present study were treated according to the current guidelines and only two patients recurred.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):403-407
To determine the clinical and epidemiological characteristics of abdominal wall endometriosis (AWE), as well as the rate and recurrence factors for the disease.
A retrospective study of 52 women with AWE was performed at Universidade Estadual de Campinas from 2004 to 2014. Of the 231 surgeries performed for the diagnosis of endometriosis, 52 women were found to have abdominal wall endometriosis (AWE). The frequencies, means and standard deviations of the clinical characteristics of these women were calculated, as well as the recurrence rate of AWE. To determine the risk factors for disease recurrence, Fisher’s exact test was used.
The mean age of the patients was 30.71 ± 5.91 years. The main clinical manifestations were pain (98%) and sensation of a mass (36.5%).We observed that 94% of these women had undergone at least 1 cesarean section, and 73% had used medication for the postoperative control of endometriosis. The lesion was most commonly located in the cesarean section scar (65%). The recurrence rate of the disease was of 26.9%. All 14 women who had relapsed had surgical margins compromised in the previous surgery. There was no correlation between recurrent AWE and a previous cesarean section (p = 0.18), previous laparotomy (p = 0.11), previous laparoscopy (p = 0.12) and postoperative hormone therapy (p = 0.51).
Women with previous cesarean sections with local pain or lumps should be investigated for AWE. The recurrence of AWE is high, especially when the first surgery is not appropriate and leaves compromised surgical margins.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):403-407
To determine the clinical and epidemiological characteristics of abdominal wall endometriosis (AWE), as well as the rate and recurrence factors for the disease.
A retrospective study of 52 women with AWE was performed at Universidade Estadual de Campinas from 2004 to 2014. Of the 231 surgeries performed for the diagnosis of endometriosis, 52 women were found to have abdominal wall endometriosis (AWE). The frequencies, means and standard deviations of the clinical characteristics of these women were calculated, as well as the recurrence rate of AWE. To determine the risk factors for disease recurrence, Fisher’s exact test was used.
The mean age of the patients was 30.71 ± 5.91 years. The main clinical manifestations were pain (98%) and sensation of a mass (36.5%).We observed that 94% of these women had undergone at least 1 cesarean section, and 73% had used medication for the postoperative control of endometriosis. The lesion was most commonly located in the cesarean section scar (65%). The recurrence rate of the disease was of 26.9%. All 14 women who had relapsed had surgical margins compromised in the previous surgery. There was no correlation between recurrent AWE and a previous cesarean section (p = 0.18), previous laparotomy (p = 0.11), previous laparoscopy (p = 0.12) and postoperative hormone therapy (p = 0.51).
Women with previous cesarean sections with local pain or lumps should be investigated for AWE. The recurrence of AWE is high, especially when the first surgery is not appropriate and leaves compromised surgical margins.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(6):288-293
To evaluate the expressions of biomarkers p16 and Ki-67 in low-grade (LG) or high-grade (HG) lesions, and to relate them to risk factors and the recurrence of these lesions.
A retrospective case-control study of 86 patients with LG and HG lesions who underwent a loop electrosurgical excision procedure (LEEP) between 1999 and 2004. The control group was composed of 69 women with no recurrence, and the study group, of 17 patients with recurrence. All patients were followed-up over a two-year period after surgery, and screened every six months, including cytology and colposcopy. Biopsy samples collected from LEEP were submitted to immunohistochemical analysis for p16 and Ki-67. The statistical analysis was performed using the Statistical Package for the Social Sciences software (SPSS, IBM-SPSS, Inc., Chicago, IL, US), with a significant p < 0.05.
The biomarkers p16 and Ki-67, separately or combined, showed no relation to recurrence on the total analysis. However, evaluating specifically HG lesions, the positive expression (2+ and 3 + ) of p16/Ki-67 was associated with recurrence (0.010). In addition, p16 isolated was also more expressive in HG lesions (2+ and 3 + , p= 0.018), but it was unrelated to recurrence.
Proteins p16 and Ki-67, both isolated and combined, are not reliable primary markers for the recurrence of cervical lesions in the majority of LG lesions. However, analyzing only the group with prior diagnosis of HG lesions, the expressions of p16 and of p16/Ki-67 were associated with recurrence, and they may be useful in monitoring these cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(6):288-293
To evaluate the expressions of biomarkers p16 and Ki-67 in low-grade (LG) or high-grade (HG) lesions, and to relate them to risk factors and the recurrence of these lesions.
A retrospective case-control study of 86 patients with LG and HG lesions who underwent a loop electrosurgical excision procedure (LEEP) between 1999 and 2004. The control group was composed of 69 women with no recurrence, and the study group, of 17 patients with recurrence. All patients were followed-up over a two-year period after surgery, and screened every six months, including cytology and colposcopy. Biopsy samples collected from LEEP were submitted to immunohistochemical analysis for p16 and Ki-67. The statistical analysis was performed using the Statistical Package for the Social Sciences software (SPSS, IBM-SPSS, Inc., Chicago, IL, US), with a significant p < 0.05.
The biomarkers p16 and Ki-67, separately or combined, showed no relation to recurrence on the total analysis. However, evaluating specifically HG lesions, the positive expression (2+ and 3 + ) of p16/Ki-67 was associated with recurrence (0.010). In addition, p16 isolated was also more expressive in HG lesions (2+ and 3 + , p= 0.018), but it was unrelated to recurrence.
Proteins p16 and Ki-67, both isolated and combined, are not reliable primary markers for the recurrence of cervical lesions in the majority of LG lesions. However, analyzing only the group with prior diagnosis of HG lesions, the expressions of p16 and of p16/Ki-67 were associated with recurrence, and they may be useful in monitoring these cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(7):314-318
DOI 10.1590/S0100-720320150005098
To identify the predominant species and the role of sexual partners in the maintenance of recurrent vulvovaginitis by Candida spp.
A prospective study of 830 patients aged 18 to 65 years with yeast vaginitis was performed between August 2007 and March 2012. Patients with diabetes mellitus, AIDS or taking corticosteroids, antibiotics or hormone therapy and immunosuppressed patients, patients using vaginal douches, spermicides or intrauterine devices were excluded from the study. Candida species were identified by phenotypic and genotypic methods. The chi-square test was used to correlate the presence of Candida spp. in male partners with the recurrence of vaginitis.
The fungal agent was isolated from a total of 40 women, 24 with recurrent vaginitis and from 15 of their sexual partners, 10 of whom were asymptomatic while 5 were symptomatic. There was agreement of the species found in the couple in 100% of recurrences. C. albicans (62.4 and 60%), C. glabrata (29.1 and 33.3%) and C. guilliermondii species were identified. Candida tropicalis (4.1%) was isolated from only one patient. Candida albicans was isolated from the remaining 16 women who had uncomplicated vaginitis. C. glabrata was isolated from only two of the asymptomatic partners.
There was a predominance of C. albicans and symptomatic or asymptomatic partners can play an important role as a reservoir and source of transmission of yeast, especially in cases of recurrent vulvovaginitis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(7):314-318
DOI 10.1590/S0100-720320150005098
To identify the predominant species and the role of sexual partners in the maintenance of recurrent vulvovaginitis by Candida spp.
A prospective study of 830 patients aged 18 to 65 years with yeast vaginitis was performed between August 2007 and March 2012. Patients with diabetes mellitus, AIDS or taking corticosteroids, antibiotics or hormone therapy and immunosuppressed patients, patients using vaginal douches, spermicides or intrauterine devices were excluded from the study. Candida species were identified by phenotypic and genotypic methods. The chi-square test was used to correlate the presence of Candida spp. in male partners with the recurrence of vaginitis.
The fungal agent was isolated from a total of 40 women, 24 with recurrent vaginitis and from 15 of their sexual partners, 10 of whom were asymptomatic while 5 were symptomatic. There was agreement of the species found in the couple in 100% of recurrences. C. albicans (62.4 and 60%), C. glabrata (29.1 and 33.3%) and C. guilliermondii species were identified. Candida tropicalis (4.1%) was isolated from only one patient. Candida albicans was isolated from the remaining 16 women who had uncomplicated vaginitis. C. glabrata was isolated from only two of the asymptomatic partners.
There was a predominance of C. albicans and symptomatic or asymptomatic partners can play an important role as a reservoir and source of transmission of yeast, especially in cases of recurrent vulvovaginitis.