-
Original Articles
The Association between N-terminal Pro-Brain Natriuretic Peptide Levels in the Umbilical Vein and Amniotic Fluid Volume Abnormalities
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):177-182
04-01-2016
Summary
Original ArticlesThe Association between N-terminal Pro-Brain Natriuretic Peptide Levels in the Umbilical Vein and Amniotic Fluid Volume Abnormalities
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):177-182
04-01-2016Views125See moreAbstract
Purpose
The amniotic fluid volume (AFV) is known as a predictor for the wellness of a fetus. We aimed to investigate whether N-terminal pro-brain natriuretic peptide (NTproBNP) levels reflect AFV abnormalities in otherwise normal fetuses.
Methods
We recruited 24 women with isolated oligohydramnios, 23 women with isolated polyhydramnios, and 36 women with normal AFV at a tertiary referral center. NT-proBNP levels in umbilical venous samples and the individual characteristics of the three groups were compared. One-way ANOVA and Kruskal-Wallis analysis of variance were used for multi-group comparisons of continuous variables. When a significant difference was detected, the Scheffe test was performed as a post-hoc analysis. Proportions were compared using the Chi-square (2) test.
Results
Maternal age, body mass indices, weight gained in pregnancy and NT-proBNP levels were similar among the three groups. Apgar scores at 1 and 5 minutes significantly correlated with NT-proBNP levels in all newborns (Spearman's r = 0.23 ; p = 0.03 and Spearman's r = 0.24; p = 0.02, respectively). The umbilical venous NTproBNP levels did not differ between newborns who needed mechanical ventilation and those who didn't (p = 0.595).
Conclusions
NT-proBNP is a biomolecule that may provide insights into the pathogenesis of fetal circulatory problems and subsequent renal failure. Further investigations are warranted.
Views125

This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticlesThe Association between N-terminal Pro-Brain Natriuretic Peptide Levels in the Umbilical Vein and Amniotic Fluid Volume Abnormalities
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):177-182
04-01-2016Views125See moreAbstract
Purpose
The amniotic fluid volume (AFV) is known as a predictor for the wellness of a fetus. We aimed to investigate whether N-terminal pro-brain natriuretic peptide (NTproBNP) levels reflect AFV abnormalities in otherwise normal fetuses.
Methods
We recruited 24 women with isolated oligohydramnios, 23 women with isolated polyhydramnios, and 36 women with normal AFV at a tertiary referral center. NT-proBNP levels in umbilical venous samples and the individual characteristics of the three groups were compared. One-way ANOVA and Kruskal-Wallis analysis of variance were used for multi-group comparisons of continuous variables. When a significant difference was detected, the Scheffe test was performed as a post-hoc analysis. Proportions were compared using the Chi-square (2) test.
Results
Maternal age, body mass indices, weight gained in pregnancy and NT-proBNP levels were similar among the three groups. Apgar scores at 1 and 5 minutes significantly correlated with NT-proBNP levels in all newborns (Spearman's r = 0.23 ; p = 0.03 and Spearman's r = 0.24; p = 0.02, respectively). The umbilical venous NTproBNP levels did not differ between newborns who needed mechanical ventilation and those who didn't (p = 0.595).
Conclusions
NT-proBNP is a biomolecule that may provide insights into the pathogenesis of fetal circulatory problems and subsequent renal failure. Further investigations are warranted.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 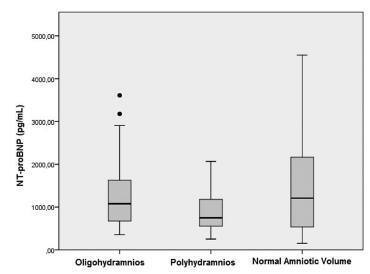
-
Artigos Originais
Maternal and perinatal outcomes in women with decreased amniotic fluid
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(8):342-348
10-10-2013
Summary
Artigos OriginaisMaternal and perinatal outcomes in women with decreased amniotic fluid
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(8):342-348
10-10-2013DOI 10.1590/S0100-72032013000800002
Views96PURPOSE: To determine maternal and perinatal outcomes in pregnant women with low amniotic fluid, according to the amniotic fluid index (AFI). METHODS: A cohort study conducted on 176 patients admitted to the high risk ward of Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), in Recife, Pernambuco, Brazil. Amniotic fluid was measured by the amniotic fluid index, and classified as low when between 5.1 and 7.9 cm, moderate oligohydramnios between 3.1 and 5.0 cm, and severe oligohydramnios when less than or equal to 3.0 cm. To determine the difference between the three groups of categorical variables studied the chi-square and Fisher exact tests were used, when applicable, and for the numerical variables the Mann-Whitney test was applied, with the level of significance set at 5%. RESULTS: Fetal malformation more frequently occurred when oligohydramnios was severe. Hypertensive disorders, however, were associated with moderate oligohydramnios. There was similarity between the three groups in relation to premature rupture of membranes and other causes. Low amniotic fluid was more frequently diagnosed when tested at the gestational age of 32 weeks or earlier. Regarding the perinatal outcomes, the incidence of Apgar score <7 in the 1st and 5th minutes, perinatal death, neonatal jaundice and pulmonary hypoplasia was higher when oligohydramnios was moderate to severe. CONCLUSIONS: Maternal and perinatal causes and outcomes in pregnant women with low amniotic fluid vary with respect to their AFI, severe oligohydramnios being associated with fetal malformation and other adverse perinatal outcomes.
Key-words Amniotic fluidFetal membranes, premature ruptureHypertensionOligohydramniosPrenatal ultrasonographySee moreViews96This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Artigos OriginaisMaternal and perinatal outcomes in women with decreased amniotic fluid
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(8):342-348
10-10-2013DOI 10.1590/S0100-72032013000800002
Views96PURPOSE: To determine maternal and perinatal outcomes in pregnant women with low amniotic fluid, according to the amniotic fluid index (AFI). METHODS: A cohort study conducted on 176 patients admitted to the high risk ward of Instituto de Medicina Integral Prof. Fernando Figueira (IMIP), in Recife, Pernambuco, Brazil. Amniotic fluid was measured by the amniotic fluid index, and classified as low when between 5.1 and 7.9 cm, moderate oligohydramnios between 3.1 and 5.0 cm, and severe oligohydramnios when less than or equal to 3.0 cm. To determine the difference between the three groups of categorical variables studied the chi-square and Fisher exact tests were used, when applicable, and for the numerical variables the Mann-Whitney test was applied, with the level of significance set at 5%. RESULTS: Fetal malformation more frequently occurred when oligohydramnios was severe. Hypertensive disorders, however, were associated with moderate oligohydramnios. There was similarity between the three groups in relation to premature rupture of membranes and other causes. Low amniotic fluid was more frequently diagnosed when tested at the gestational age of 32 weeks or earlier. Regarding the perinatal outcomes, the incidence of Apgar score <7 in the 1st and 5th minutes, perinatal death, neonatal jaundice and pulmonary hypoplasia was higher when oligohydramnios was moderate to severe. CONCLUSIONS: Maternal and perinatal causes and outcomes in pregnant women with low amniotic fluid vary with respect to their AFI, severe oligohydramnios being associated with fetal malformation and other adverse perinatal outcomes.
Key-words Amniotic fluidFetal membranes, premature ruptureHypertensionOligohydramniosPrenatal ultrasonographySee moreThis is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Artigos Originais
Is uterine height able to diagnose amniotic fluid volume deviations?
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(2):49-54
02-07-2013
Summary
Artigos OriginaisIs uterine height able to diagnose amniotic fluid volume deviations?
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(2):49-54
02-07-2013DOI 10.1590/S0100-72032013000200002
Views96See morePURPOSE: To evaluate the performance of a Brazilian reference curve of fundal height (FH) regarding its capacity of screening the deviations of volume of amniotic fluid using a Brazilian reference curve of amniotic fluid index (AFI) as gold standard. METHODS: This was a cross-sectional study evaluating 753 pregnant women receiving prenatal care at the public health services of João Pessoa (PB), from March to October 2006, who had a routine ultrasound exam scheduled for after 26 weeks of gestational age. Cases with diagnoses of twin pregnancy, intrauterine fetal death and major fetal malformations were excluded. Besides socio-demographic information, data regarding fundal height measured in a standard way, estimated fetal weight, AFI and gestational age at the time of the ultrasound exam were also collected. The capacity of the FH curve to predict deviations of the amniotic fluid volume was assessed using the Brazilian curve of AFI according to gestational age as the gold standard. For this purpose, sensitivity, specificity, positive and negative predictive values were estimated for different cut-off points. RESULTS: The measurement of FH identified 10.5% of women as having low FH possibly associated with oligohydramnios and 25.2% as having high FH possibly associated with polyhydramnios. Using a Brazilian reference curve of AFI, the FH was able to poorly predict the occurrence of oligohydramnios (sensitivity ranging from 37 to 28%) and to reasonably predict the occurrence of polyhydramnios (sensitivity ranging from 88 to 69%). CONCLUSIONS: The measurement of fundal height showed a poor performance for predicting oligohydramnios and a reasonable performance for predicting polyhydramnios. Its use for this purpose is then only supported in settings where the ultrasound exam is not easily or routinely available in order to help define priorities for cases that should have this exam performed.
Views96This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Artigos OriginaisIs uterine height able to diagnose amniotic fluid volume deviations?
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(2):49-54
02-07-2013DOI 10.1590/S0100-72032013000200002
Views96See morePURPOSE: To evaluate the performance of a Brazilian reference curve of fundal height (FH) regarding its capacity of screening the deviations of volume of amniotic fluid using a Brazilian reference curve of amniotic fluid index (AFI) as gold standard. METHODS: This was a cross-sectional study evaluating 753 pregnant women receiving prenatal care at the public health services of João Pessoa (PB), from March to October 2006, who had a routine ultrasound exam scheduled for after 26 weeks of gestational age. Cases with diagnoses of twin pregnancy, intrauterine fetal death and major fetal malformations were excluded. Besides socio-demographic information, data regarding fundal height measured in a standard way, estimated fetal weight, AFI and gestational age at the time of the ultrasound exam were also collected. The capacity of the FH curve to predict deviations of the amniotic fluid volume was assessed using the Brazilian curve of AFI according to gestational age as the gold standard. For this purpose, sensitivity, specificity, positive and negative predictive values were estimated for different cut-off points. RESULTS: The measurement of FH identified 10.5% of women as having low FH possibly associated with oligohydramnios and 25.2% as having high FH possibly associated with polyhydramnios. Using a Brazilian reference curve of AFI, the FH was able to poorly predict the occurrence of oligohydramnios (sensitivity ranging from 37 to 28%) and to reasonably predict the occurrence of polyhydramnios (sensitivity ranging from 88 to 69%). CONCLUSIONS: The measurement of fundal height showed a poor performance for predicting oligohydramnios and a reasonable performance for predicting polyhydramnios. Its use for this purpose is then only supported in settings where the ultrasound exam is not easily or routinely available in order to help define priorities for cases that should have this exam performed.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Artigos Originais
Fetal bilateral obstructive uropathies: ultrasound findings during pregnancy and postnatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(11):540-546
01-12-2009
Summary
Artigos OriginaisFetal bilateral obstructive uropathies: ultrasound findings during pregnancy and postnatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(11):540-546
01-12-2009DOI 10.1590/S0100-72032009001100003
Views101PURPOSE: to verify the association between ultrasonographic signs during gestation and post-delivery evolution in fetuses with bilateral obstructive uropathies, followed up in an expectant way. METHODS: fetuses with bilateral obstructive uropathies presenting severe oligoamnios and narrow thorax have been compared with fetuses with bilateral obstructive uropathies without those alterations, concerning the presence or absence of cysts in both kidneys, and the presence or absence of parenchymal hyperechogenicity in both kidneys. Cases of neonatal death were compared with cases of neonatal discharge from the nursery, regarding the same renal echographic aspects mentioned above, the presence of severe oligoamnios and narrow thorax. The sensitivity, specificity, positive and negative predictive value of the presence of bilateral renal cysts, bilateral renal hyperechogenicity, severe oligoamnios and narrow fetal thorax for the neonatal death were calculated. RESULTS: severe oligoamnios and narrow thorax were more frequent (p=0.03; p<0.001) in fetuses with bilateral renal cysts, as compared to those with echographically normal renal parenchyma. Neonatal death was more frequent among cases with severe oligoamnios (p<0.001), narrow thorax (p<0.001) and bilateral renal cysts (p<0.002), when respectively compared with cases without those alterations. The best values of sensitivity, specificity, positive and negative predictive value for the death of neonatal/breastfeeding infants were obtained using the echographic aspect of narrow thorax, and were 81.8, 100, 100 and 79.3%, respectively. CONCLUSIONS: in cases of fetuses with bilateral obstructive uropathies followed up in an expectant way, the ultrasonographic signs more associated to bad prognosis are severe oligoamnios, narrow fetal thorax and presence of bilateral renal cysts.
Key-words Fetal diseasesHydronephrosisInfant, newbornKidney diseases, cysticNatural history of diseasesOligohydramniosUltrasonography, prenatalUrethral diseasesUrinary tractSee moreViews101This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Artigos OriginaisFetal bilateral obstructive uropathies: ultrasound findings during pregnancy and postnatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(11):540-546
01-12-2009DOI 10.1590/S0100-72032009001100003
Views101PURPOSE: to verify the association between ultrasonographic signs during gestation and post-delivery evolution in fetuses with bilateral obstructive uropathies, followed up in an expectant way. METHODS: fetuses with bilateral obstructive uropathies presenting severe oligoamnios and narrow thorax have been compared with fetuses with bilateral obstructive uropathies without those alterations, concerning the presence or absence of cysts in both kidneys, and the presence or absence of parenchymal hyperechogenicity in both kidneys. Cases of neonatal death were compared with cases of neonatal discharge from the nursery, regarding the same renal echographic aspects mentioned above, the presence of severe oligoamnios and narrow thorax. The sensitivity, specificity, positive and negative predictive value of the presence of bilateral renal cysts, bilateral renal hyperechogenicity, severe oligoamnios and narrow fetal thorax for the neonatal death were calculated. RESULTS: severe oligoamnios and narrow thorax were more frequent (p=0.03; p<0.001) in fetuses with bilateral renal cysts, as compared to those with echographically normal renal parenchyma. Neonatal death was more frequent among cases with severe oligoamnios (p<0.001), narrow thorax (p<0.001) and bilateral renal cysts (p<0.002), when respectively compared with cases without those alterations. The best values of sensitivity, specificity, positive and negative predictive value for the death of neonatal/breastfeeding infants were obtained using the echographic aspect of narrow thorax, and were 81.8, 100, 100 and 79.3%, respectively. CONCLUSIONS: in cases of fetuses with bilateral obstructive uropathies followed up in an expectant way, the ultrasonographic signs more associated to bad prognosis are severe oligoamnios, narrow fetal thorax and presence of bilateral renal cysts.
Key-words Fetal diseasesHydronephrosisInfant, newbornKidney diseases, cysticNatural history of diseasesOligohydramniosUltrasonography, prenatalUrethral diseasesUrinary tractSee moreThis is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Trabalhos Originais
Diagnostic capacity of oligohydramnios by ultrasound using different measures of the maximum pool depth of amniotic fluid in comparison to AFI
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(1):7-12
10-13-2000
Summary
Trabalhos OriginaisDiagnostic capacity of oligohydramnios by ultrasound using different measures of the maximum pool depth of amniotic fluid in comparison to AFI
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(1):7-12
10-13-2000DOI 10.1590/S0100-72032000000100002
Views81See morePurpose: to compare the capacity of diagnosing oligohy-dramnios by ultrasound using different measures of the maximum pool depth of amniotic fluid in comparison to the amniotic fluid index among normal pregnant women from the 36th to the 42nd week of gestation. Methods: a descriptive study of diagnostic validity was perfomed, on 875 normal pregnant women who were studied through routine obstetric ultrasound examinations, including the measure of the maximum pool depth for the diagnosis of oligohydramnios, using the amniotic fluid index as the gold standard. The data were analyzed through sensitivity and specificity of the maximum pool depth of amniotic fluid using 10, 20 and 30 mm cut-offs, in comparison to the amniotic fluid index values of the normal curve in percentiles 2.5 and 10 for different gestational ages. Results: the maximum pool depth had a poor sensitivity to diagnose oligohydramnios when 10 and 20 mm were used as cut-offs, and good sensitivity and specificity when 30 mm was used, in comparison to the amniotic fluid values in percentiles 2.5 and 10. The best sensitivity and specificity of the maximum pool depth were when found using a 30 mm cut-off in comparison to 2.5 percentile to diagnose oligohydramnios. Conclusions: the capacity to diagnose oligohydramnios by the measure of the maximum pool depth is satisfactory only with the cut-off of 30 mm
Views81This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Trabalhos OriginaisDiagnostic capacity of oligohydramnios by ultrasound using different measures of the maximum pool depth of amniotic fluid in comparison to AFI
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(1):7-12
10-13-2000DOI 10.1590/S0100-72032000000100002
Views81See morePurpose: to compare the capacity of diagnosing oligohy-dramnios by ultrasound using different measures of the maximum pool depth of amniotic fluid in comparison to the amniotic fluid index among normal pregnant women from the 36th to the 42nd week of gestation. Methods: a descriptive study of diagnostic validity was perfomed, on 875 normal pregnant women who were studied through routine obstetric ultrasound examinations, including the measure of the maximum pool depth for the diagnosis of oligohydramnios, using the amniotic fluid index as the gold standard. The data were analyzed through sensitivity and specificity of the maximum pool depth of amniotic fluid using 10, 20 and 30 mm cut-offs, in comparison to the amniotic fluid index values of the normal curve in percentiles 2.5 and 10 for different gestational ages. Results: the maximum pool depth had a poor sensitivity to diagnose oligohydramnios when 10 and 20 mm were used as cut-offs, and good sensitivity and specificity when 30 mm was used, in comparison to the amniotic fluid values in percentiles 2.5 and 10. The best sensitivity and specificity of the maximum pool depth were when found using a 30 mm cut-off in comparison to 2.5 percentile to diagnose oligohydramnios. Conclusions: the capacity to diagnose oligohydramnios by the measure of the maximum pool depth is satisfactory only with the cut-off of 30 mm
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Artigos Originais
Oligohydramnios without premature rupture of membranes: perinatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(2):75-79
07-06-2005
Summary
Artigos OriginaisOligohydramnios without premature rupture of membranes: perinatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(2):75-79
07-06-2005DOI 10.1590/S0100-72032005000200006
Views111See morePURPOSE: to evaluate perinatal outcomes in cases of oligohydramnios without premature rupture of membranes. METHODS: a total of 51 consecutive cases of oligohydramnios (amniotic fluid index, AFI < 5 cm) born between March 1998 and September 2001 were studied retrospectively. Data were compared to 61 cases with intermediate and normal volume of amniotic fluid AFI >5). Maternal and neonatal variables, as well as fetal mortality, early neonatal, and perinatal mortality rates were analyzed. For statistical analysis the c² test with Yates correction and Student's t test were used with level of signicance set at 5%. RESULTS: there were no significant differences between groups when the presence of gestational hypertensive syndromes, meconium-stained amniotic fluid, 1- and 5-minute Apgar score, need of neonatal intensive center unit, and preterm birth were analyzed. Oligohydramnios was associated with the way of delivery (p<0.0002; RR=0.3), fetal distress (p<0.0004; RR=2.2) and fetal malformations (p<0.01; RR=5.4). Fetal malformation rates were 17.6 and 3.3% in oligohydramnios and normal groups, respectively. Fetal mortality (2.0 vs 1.6%), early neonatal (5.9 vs 1.6%) and perinatal mortality (7.8 vs 3.3%) rates in both groups did not show statistical significance. CONCLUSION: Oligohydramnios was related to increased risk factor for cesarean section, fetal distress and fetal malformations.
Views111This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Artigos OriginaisOligohydramnios without premature rupture of membranes: perinatal outcomes
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(2):75-79
07-06-2005DOI 10.1590/S0100-72032005000200006
Views111See morePURPOSE: to evaluate perinatal outcomes in cases of oligohydramnios without premature rupture of membranes. METHODS: a total of 51 consecutive cases of oligohydramnios (amniotic fluid index, AFI < 5 cm) born between March 1998 and September 2001 were studied retrospectively. Data were compared to 61 cases with intermediate and normal volume of amniotic fluid AFI >5). Maternal and neonatal variables, as well as fetal mortality, early neonatal, and perinatal mortality rates were analyzed. For statistical analysis the c² test with Yates correction and Student's t test were used with level of signicance set at 5%. RESULTS: there were no significant differences between groups when the presence of gestational hypertensive syndromes, meconium-stained amniotic fluid, 1- and 5-minute Apgar score, need of neonatal intensive center unit, and preterm birth were analyzed. Oligohydramnios was associated with the way of delivery (p<0.0002; RR=0.3), fetal distress (p<0.0004; RR=2.2) and fetal malformations (p<0.01; RR=5.4). Fetal malformation rates were 17.6 and 3.3% in oligohydramnios and normal groups, respectively. Fetal mortality (2.0 vs 1.6%), early neonatal (5.9 vs 1.6%) and perinatal mortality (7.8 vs 3.3%) rates in both groups did not show statistical significance. CONCLUSION: Oligohydramnios was related to increased risk factor for cesarean section, fetal distress and fetal malformations.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Trabalhos Originais
Perinatal outcomes of oligohydramnios without premature rupture of membranes detected until the 26th week of pregnancy
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):419-423
10-07-2003
Summary
Trabalhos OriginaisPerinatal outcomes of oligohydramnios without premature rupture of membranes detected until the 26th week of pregnancy
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):419-423
10-07-2003DOI 10.1590/S0100-72032003000600006
Views66See morePURPOSE: to evaluate the perinatal outcomes of pregnancies complicated by oligohydramnios, not due to premature rupture of membranes (PRM), diagnosed until the 26th week of gestation. PATIENTS AND METHODS: we analyzed retrospectively the cases of oligohydramnios that occurred from January 1994 to December 2000, and were diagnosed until the 26th week of gestation. Oligohydramnios was present when the amniotic fluid index was less or equal to 5.0 cm. After diagnosis the patients were followed-up with serial ultrasound evaluation, with emphasis on the maintenance of the oligohydramnios state. When remission of the oligohydramnios occurred, patients remained in the study. Cases due to PRM, fetal death detected on the first examination and the women who gave birth in another institution were excluded from the study. Concerning the patients, the presence of clinical and obstetric diseases was investigated. As regards the newborns, we evaluated birth weight, time of admission/death, occurrence of death or malformations. RESULTS: twenty-seven cases of oligohydramnios were analyzed. Thirteen fetuses had congenital anomalies, and among them, eight had anomalies of the urinary tract, four of the nervous system and one had cystic hygroma. Fourteen patients had a clinical or an obstetric disease, mainly hypertension (10 cases). In addition, we found three cases of placenta previa and one case of thyropathy. There were thirteen fetal deaths and fourteen neonatal deaths. CONCLUSION: oligohydramnios not due to PRM, occurring in the second trimester of gestation, independent of the etiology or the presence of congenital anomalies, was associated with a fatal perinatal result.
Views66This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Trabalhos OriginaisPerinatal outcomes of oligohydramnios without premature rupture of membranes detected until the 26th week of pregnancy
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):419-423
10-07-2003DOI 10.1590/S0100-72032003000600006
Views66See morePURPOSE: to evaluate the perinatal outcomes of pregnancies complicated by oligohydramnios, not due to premature rupture of membranes (PRM), diagnosed until the 26th week of gestation. PATIENTS AND METHODS: we analyzed retrospectively the cases of oligohydramnios that occurred from January 1994 to December 2000, and were diagnosed until the 26th week of gestation. Oligohydramnios was present when the amniotic fluid index was less or equal to 5.0 cm. After diagnosis the patients were followed-up with serial ultrasound evaluation, with emphasis on the maintenance of the oligohydramnios state. When remission of the oligohydramnios occurred, patients remained in the study. Cases due to PRM, fetal death detected on the first examination and the women who gave birth in another institution were excluded from the study. Concerning the patients, the presence of clinical and obstetric diseases was investigated. As regards the newborns, we evaluated birth weight, time of admission/death, occurrence of death or malformations. RESULTS: twenty-seven cases of oligohydramnios were analyzed. Thirteen fetuses had congenital anomalies, and among them, eight had anomalies of the urinary tract, four of the nervous system and one had cystic hygroma. Fourteen patients had a clinical or an obstetric disease, mainly hypertension (10 cases). In addition, we found three cases of placenta previa and one case of thyropathy. There were thirteen fetal deaths and fourteen neonatal deaths. CONCLUSION: oligohydramnios not due to PRM, occurring in the second trimester of gestation, independent of the etiology or the presence of congenital anomalies, was associated with a fatal perinatal result.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Trabalhos Originais
The use of Diagnostic Amnioinfusion in Severe Oligohydramnios
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):383-387
09-23-2002
Summary
Trabalhos OriginaisThe use of Diagnostic Amnioinfusion in Severe Oligohydramnios
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):383-387
09-23-2002DOI 10.1590/S0100-72032002000600005
Views130See morePurpose: to evaluate the effectiveness of diagnostic amnioinfusion in severe oligohydramnios. Methods: twelve patients with severe oligohydramnios in the second and third trimester of pregnancy were submitted to amnioinfusion. The procedure was done using a warm physiological saline at a rate of 20 mL/min followed by the instillation of 5 mL of dye. The amniotic fluid index (AFI) was measured before the procedure and 30 min afterwards and in case of fetal anomalies, it was documented. The gestational age ranged from 18 to 34 weeks (average 25 ± 4 weeks). The average of the initial ILA was 10.3cm and after the procedure was 16.4 cm. The volume of saline solution infused ranged from 300 to 1000 mL (605.4 ± 224.1 mL). Results: in nine patients (75%) the procedure led to an etiologic diagnosis: four cases of premature rupture of membranes and major malformations in five fetuses. In two patients the oligohydramnios was considered idiopathic and in one patient the pathological examination revealed a placental infarct. Nine pregnancies (75%) were interrupted after the diagnosis and in three cases it was maintained for 8.8 weeks after the amnioinfusion. All fetuses died, seven of them had neonatal death and the remaining had intrauterine death. Conclusion: amnioinfusion is an effective method with high precision, enabling the etiologic diagnosis of severe oligohydramnios in 75% of the cases.
Views130This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Trabalhos OriginaisThe use of Diagnostic Amnioinfusion in Severe Oligohydramnios
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):383-387
09-23-2002DOI 10.1590/S0100-72032002000600005
Views130See morePurpose: to evaluate the effectiveness of diagnostic amnioinfusion in severe oligohydramnios. Methods: twelve patients with severe oligohydramnios in the second and third trimester of pregnancy were submitted to amnioinfusion. The procedure was done using a warm physiological saline at a rate of 20 mL/min followed by the instillation of 5 mL of dye. The amniotic fluid index (AFI) was measured before the procedure and 30 min afterwards and in case of fetal anomalies, it was documented. The gestational age ranged from 18 to 34 weeks (average 25 ± 4 weeks). The average of the initial ILA was 10.3cm and after the procedure was 16.4 cm. The volume of saline solution infused ranged from 300 to 1000 mL (605.4 ± 224.1 mL). Results: in nine patients (75%) the procedure led to an etiologic diagnosis: four cases of premature rupture of membranes and major malformations in five fetuses. In two patients the oligohydramnios was considered idiopathic and in one patient the pathological examination revealed a placental infarct. Nine pregnancies (75%) were interrupted after the diagnosis and in three cases it was maintained for 8.8 weeks after the amnioinfusion. All fetuses died, seven of them had neonatal death and the remaining had intrauterine death. Conclusion: amnioinfusion is an effective method with high precision, enabling the etiologic diagnosis of severe oligohydramnios in 75% of the cases.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.