-
Original Article
Impact of doula’s continuous support on serotonin release in parturients: a pilot randomized clinical trial
- Eleonora de Deus Vieira de Moraes
 ,
, - Mayara Segundo Ribeiro ,
- Cíntia Erbert ,
- Caio Antonio de Campos Prado ,
- Elaine Christine Dantas Moisés
04-09-2024
Summary
Original ArticleImpact of doula’s continuous support on serotonin release in parturients: a pilot randomized clinical trial
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo27
04-09-2024- Eleonora de Deus Vieira de Moraes ,
- Mayara Segundo Ribeiro ,
- Cíntia Erbert ,
- Caio Antonio de Campos Prado ,
- Elaine Christine Dantas Moisés
Views371See moreAbstract
Objective:
To evaluate whether the continuous support provided by doulas influences the endogenous release of serotonin in parturients.
Methods:
This pilot study included 24 primigravidae at term. Of these, 12 women received continuous doula support (Experimental Group), whereas the other 12 received the usual assistance without doula support (Control Group). Blood samples were collected from all the women at the active and expulsion stages of labor and at the fourth period of labor (Greenberg period) for evaluation of their serotonin levels using high-performance liquid chromatography.
Results:
The average serotonin concentrations in the control and experimental groups were respectively 159.33 and 150.02 ng/mL at the active stage, 179.13 and 162.65 ng/mL at the expulsion stage, and 198.94 and 221.21 ng/mL at the Greenberg period. There were no statistically significant differences in serotonin concentrations between the two groups at the active and expulsion stages of labor. By contrast, within the experimental group, a significant increase in serotonin concentration was observed in the Greenberg period compared with the levels in the active and expulsion stages (p < 0.05).
Conclusion:
The novelty of this study relies on the ability to correlate the influence of the continuous support offered by doulas with the release of serotonin in parturients, with the results suggesting that the assistance received during labor can modulate the levels of hormone release in the Greenberg period.
Brazilian Registry of Clinical Trials:
RBR-4zjjm4h
Views371

This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticleImpact of doula’s continuous support on serotonin release in parturients: a pilot randomized clinical trial
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo27
04-09-2024- Eleonora de Deus Vieira de Moraes ,
- Mayara Segundo Ribeiro ,
- Cíntia Erbert ,
- Caio Antonio de Campos Prado ,
- Elaine Christine Dantas Moisés
Views371See moreAbstract
Objective:
To evaluate whether the continuous support provided by doulas influences the endogenous release of serotonin in parturients.
Methods:
This pilot study included 24 primigravidae at term. Of these, 12 women received continuous doula support (Experimental Group), whereas the other 12 received the usual assistance without doula support (Control Group). Blood samples were collected from all the women at the active and expulsion stages of labor and at the fourth period of labor (Greenberg period) for evaluation of their serotonin levels using high-performance liquid chromatography.
Results:
The average serotonin concentrations in the control and experimental groups were respectively 159.33 and 150.02 ng/mL at the active stage, 179.13 and 162.65 ng/mL at the expulsion stage, and 198.94 and 221.21 ng/mL at the Greenberg period. There were no statistically significant differences in serotonin concentrations between the two groups at the active and expulsion stages of labor. By contrast, within the experimental group, a significant increase in serotonin concentration was observed in the Greenberg period compared with the levels in the active and expulsion stages (p < 0.05).
Conclusion:
The novelty of this study relies on the ability to correlate the influence of the continuous support offered by doulas with the release of serotonin in parturients, with the results suggesting that the assistance received during labor can modulate the levels of hormone release in the Greenberg period.
Brazilian Registry of Clinical Trials:
RBR-4zjjm4h
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Eleonora de Deus Vieira de Moraes
-
Review Article
How to Reach the Best Ultrasound Performance in the Delivery Room
- Eduardo Félix Martins Santana ,
- Renata Gomes Castello ,
- Maria Eduarda Tenório Passos ,
- Gabriela Carneiro Freitas Ribeiro ,
- Edward Araujo Júnior
01-23-2022
Summary
Review ArticleHow to Reach the Best Ultrasound Performance in the Delivery Room
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1070-1077
01-23-2022- Eduardo Félix Martins Santana ,
- Renata Gomes Castello ,
- Maria Eduarda Tenório Passos ,
- Gabriela Carneiro Freitas Ribeiro ,
- Edward Araujo Júnior
Views167See moreAbstract
Ultrasonography is an instrument that is present in the maternal-fetal assessment throughout pregnancy and with widely documented benefits, but its use in intrapartum is becoming increasingly relevant. From the assessment of labor progression to the assessment of placental disorders, ultrasound can be used to correlate with physiological findings and physical examination, as its benefit in the delivery room cannot yet be proven. There are still few professionals with adequate training for its use in the delivery room and for the correct interpretation of data. Thus, this article aims to present a review of the entire applicability of ultrasound in the delivery room, considering the main stages of labor. There is still limited research in evidence-based medicine of its various possible uses in intrapartum, but it is expected that further studies can bring improvements in the quality of maternal and neonatal health during labor.
Views167This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Review ArticleHow to Reach the Best Ultrasound Performance in the Delivery Room
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1070-1077
01-23-2022- Eduardo Félix Martins Santana ,
- Renata Gomes Castello ,
- Maria Eduarda Tenório Passos ,
- Gabriela Carneiro Freitas Ribeiro ,
- Edward Araujo Júnior
Views167See moreAbstract
Ultrasonography is an instrument that is present in the maternal-fetal assessment throughout pregnancy and with widely documented benefits, but its use in intrapartum is becoming increasingly relevant. From the assessment of labor progression to the assessment of placental disorders, ultrasound can be used to correlate with physiological findings and physical examination, as its benefit in the delivery room cannot yet be proven. There are still few professionals with adequate training for its use in the delivery room and for the correct interpretation of data. Thus, this article aims to present a review of the entire applicability of ultrasound in the delivery room, considering the main stages of labor. There is still limited research in evidence-based medicine of its various possible uses in intrapartum, but it is expected that further studies can bring improvements in the quality of maternal and neonatal health during labor.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Eduardo Félix Martins Santana
-
Original Article
Robson’s Ten Group Classification System to Evaluate Cesarean Section Rates in Honduras: The Relevance of Labor Induction
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):830-837
01-06-2022
Summary
Original ArticleRobson’s Ten Group Classification System to Evaluate Cesarean Section Rates in Honduras: The Relevance of Labor Induction
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):830-837
01-06-2022Views148See moreAbstract
Objective
To use the Robson Ten Group Classification (RTGC) to analyze cesarean section (CS) rates in a Honduran maternity hospital, with focus in groups that consider induction of labor.
Methods
Cross-sectional study. Women admitted for childbirth (August 2017 to October 2018) were classified according to the RTGC. The CS rate for each group and the contribution to the overall CS rate was calculated, with further analyses of the induction of labor among term primiparous (group 2a), term multiparous (group 4a), and cases with one previous CS (group 5.1).
Results
A total of 4,356 women were considered, with an overall CS rate of 26.1%. Group 3 was the largest group, with 38.6% (1,682/4,356) of the cases, followed by Group 1, with 30.8% (1,342/4,356), and Group 5, with 10.3% (450/4,356). Considering the contribution to overall CS rates per group, Group 5 contributed with 30.4% (345/1,136) of the CSs and within this group, 286/345 (82.9%) had 1 previous CS, with a CS rate > 70%. Groups 1 and 3, with 26.6% (291/1,136) and 13.5% (153/1,136), respectively, were the second and third larger contributors to the CS rate. Groups 2a and 4a had high induction success, with low CS rates (18.4 and 16.9%, respectively).
Conclusion
The RTGC is a useful tool to assess CS rates in different healthcare facilities. Groups 5, 1, and 3 were the main contributors to the CS rate, and groups 2 and 4 showed the impact and importance of induction of labor. These findings may support future interventions to reduce unnecessary CS, especially among primiparous and in women with previous CS.
Views148This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticleRobson’s Ten Group Classification System to Evaluate Cesarean Section Rates in Honduras: The Relevance of Labor Induction
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):830-837
01-06-2022Views148See moreAbstract
Objective
To use the Robson Ten Group Classification (RTGC) to analyze cesarean section (CS) rates in a Honduran maternity hospital, with focus in groups that consider induction of labor.
Methods
Cross-sectional study. Women admitted for childbirth (August 2017 to October 2018) were classified according to the RTGC. The CS rate for each group and the contribution to the overall CS rate was calculated, with further analyses of the induction of labor among term primiparous (group 2a), term multiparous (group 4a), and cases with one previous CS (group 5.1).
Results
A total of 4,356 women were considered, with an overall CS rate of 26.1%. Group 3 was the largest group, with 38.6% (1,682/4,356) of the cases, followed by Group 1, with 30.8% (1,342/4,356), and Group 5, with 10.3% (450/4,356). Considering the contribution to overall CS rates per group, Group 5 contributed with 30.4% (345/1,136) of the CSs and within this group, 286/345 (82.9%) had 1 previous CS, with a CS rate > 70%. Groups 1 and 3, with 26.6% (291/1,136) and 13.5% (153/1,136), respectively, were the second and third larger contributors to the CS rate. Groups 2a and 4a had high induction success, with low CS rates (18.4 and 16.9%, respectively).
Conclusion
The RTGC is a useful tool to assess CS rates in different healthcare facilities. Groups 5, 1, and 3 were the main contributors to the CS rate, and groups 2 and 4 showed the impact and importance of induction of labor. These findings may support future interventions to reduce unnecessary CS, especially among primiparous and in women with previous CS.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Review Article
Intermittent versus Continuous Catheterization and Differences in the Evolution of Labor: Systematic Review and Meta-analysis
- Inês Reis ,
- Sara Cunha ,
- Matilde Martins ,
- Luísa Sousa ,
- Adérito Seixas , [ ... ],
- Cátia Rasteiro
01-24-2021
Summary
Review ArticleIntermittent versus Continuous Catheterization and Differences in the Evolution of Labor: Systematic Review and Meta-analysis
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(12):961-967
01-24-2021Views166See moreAbstract
Objective
To evaluate the differences between bladder emptying options (permanent catheterization and intermittent bladder emptying/spontaneous urination) regarding the effects on labor length, need of operative vaginal deliveries, and cesarean section rate.
Data Sources
The search was conducted in MEDLINE, Scopus, Web of Science, and The Cochrane Central Register of Controlled Trials databases.
Selection of Studies
The survey returned 964 studies. A total of 719 studies were evaluated by title and abstract, of which 4 were selected for inclusion.
Data Collection
All references were inserted in the Rayyan QCRI tool (Rayyan Systems Inc., Cambridge, MA, USA). The full text of the selected articles was obtained so we could later decide whether or not to include them in this systematic review.
Data Synthesis
No differences were found in the number of instrumented deliveries or in cesarean section rate between groups.
Conclusions
After evaluating the studies performed on the topic, we concluded that there is no clear advantage to either method, although continuous catheterization was associated with a greater occurrence of eutocic births. In the remaining outcomes, there were no differences between catheterization types.
Views166This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Review ArticleIntermittent versus Continuous Catheterization and Differences in the Evolution of Labor: Systematic Review and Meta-analysis
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(12):961-967
01-24-2021Views166See moreAbstract
Objective
To evaluate the differences between bladder emptying options (permanent catheterization and intermittent bladder emptying/spontaneous urination) regarding the effects on labor length, need of operative vaginal deliveries, and cesarean section rate.
Data Sources
The search was conducted in MEDLINE, Scopus, Web of Science, and The Cochrane Central Register of Controlled Trials databases.
Selection of Studies
The survey returned 964 studies. A total of 719 studies were evaluated by title and abstract, of which 4 were selected for inclusion.
Data Collection
All references were inserted in the Rayyan QCRI tool (Rayyan Systems Inc., Cambridge, MA, USA). The full text of the selected articles was obtained so we could later decide whether or not to include them in this systematic review.
Data Synthesis
No differences were found in the number of instrumented deliveries or in cesarean section rate between groups.
Conclusions
After evaluating the studies performed on the topic, we concluded that there is no clear advantage to either method, although continuous catheterization was associated with a greater occurrence of eutocic births. In the remaining outcomes, there were no differences between catheterization types.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 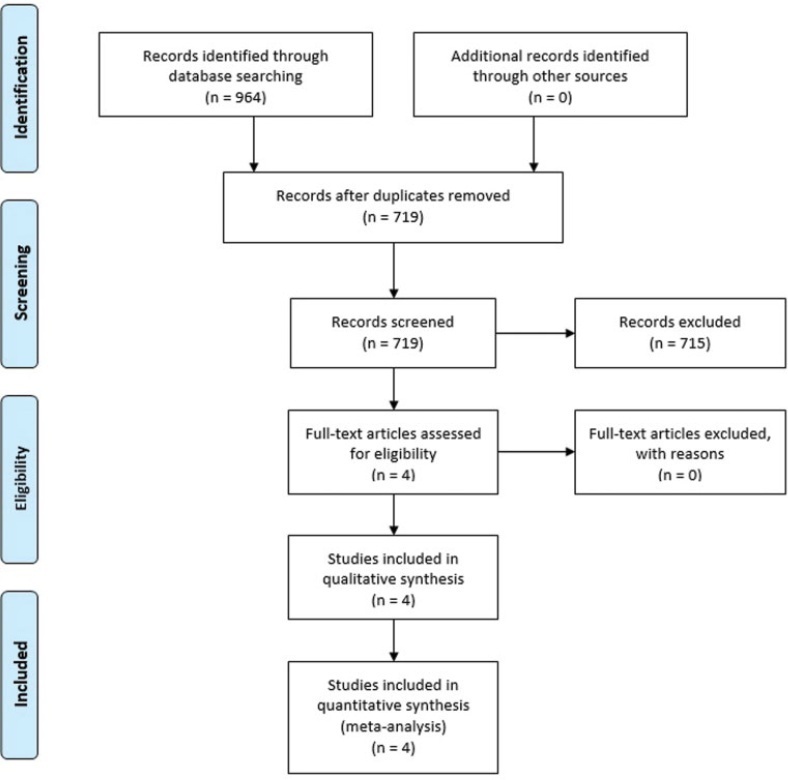
- Inês Reis
-
Original Article
Pubic Arch Angle Measurement by Transperineal Ultrasonography: A Prospective Cross-Sectional Study
- Raimundo Homero Carvalho Neto ,
- Antonio Brazil Viana Junior ,
- Antonio Fernandes Moron ,
- Edward Araujo Júnior ,
- Francisco Herlânio Costa Carvalho , [ ... ],
- Helvécio Neves Feitosa
05-18-2020
Summary
Original ArticlePubic Arch Angle Measurement by Transperineal Ultrasonography: A Prospective Cross-Sectional Study
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):181-187
05-18-2020- Raimundo Homero Carvalho Neto ,
- Antonio Brazil Viana Junior ,
- Antonio Fernandes Moron ,
- Edward Araujo Júnior ,
- Francisco Herlânio Costa Carvalho ,
- Helvécio Neves Feitosa
Views154See moreAbstract
Objective
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
Methods
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Results
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Conclusion
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.
Views154This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticlePubic Arch Angle Measurement by Transperineal Ultrasonography: A Prospective Cross-Sectional Study
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):181-187
05-18-2020- Raimundo Homero Carvalho Neto ,
- Antonio Brazil Viana Junior ,
- Antonio Fernandes Moron ,
- Edward Araujo Júnior ,
- Francisco Herlânio Costa Carvalho ,
- Helvécio Neves Feitosa
Views154See moreAbstract
Objective
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
Methods
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Results
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Conclusion
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Raimundo Homero Carvalho Neto
-
Original Article
Do We Know How to Avoid OASIs in Non-Supine Birth Positions? A Retrospective Cohort Analysis
- Zilma Silveira Nogueira Reis ,
- Glaucia Miranda Varella Pereira ,
- Anna Laura Freitas Vianini,
- Marilene Vale Castro Monteiro,
- Regina Amélia Lopes Pessoa Aguiar
11-07-2019
Summary
Original ArticleDo We Know How to Avoid OASIs in Non-Supine Birth Positions? A Retrospective Cohort Analysis
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(10):581-587
11-07-2019- Zilma Silveira Nogueira Reis ,
- Glaucia Miranda Varella Pereira ,
- Anna Laura Freitas Vianini,
- Marilene Vale Castro Monteiro,
- Regina Amélia Lopes Pessoa Aguiar
Views129See moreAbstract
Objective
To evaluate the association between the upright and supine maternal positions for birth and the incidence of obstetric anal sphincter injuries (OASIs).
Methods
Retrospective cohort study analyzed the data of 1,728 pregnant women who vaginally delivered live single cephalic newborns with a birth weight of 2,500 g. Multiple regression analyses were used to investigate the effect of the supine and upright positions on the incidence of OASIs after adjusting for risk factors and obstetric interventions.
Results
In total, 239 (13.8%) births occurred in upright positions, and 1,489 (86.2%) in supine positions. Grade-III lacerations occurred in 43 (2.5%) patients, and grade-IV lacerations occurred in 3 (0.2%) women. Supine positions had a significant protective effect against severe lacerations, odds ratio [95% confidence interval]: 0,47 [0.22- 0.99], adjusted for the use of forceps 4.80 [2.15-10.70], nulliparity 2.86 [1.44-5.69], and birth weight 3.30 [1.56-7.00]. Anesthesia (p<0.070), oxytocin augmentation (p<0.228), shoulder dystocia (p<0.670), and episiotomy (p<0.559) were not associated with the incidence of severe lacerations.
Conclusion
Upright birth positions were not associated with a lower rate of perineal tears. The interpretation of the findings regarding these positions raised doubts about perineal protection that are still unanswered.
Views129This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticleDo We Know How to Avoid OASIs in Non-Supine Birth Positions? A Retrospective Cohort Analysis
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(10):581-587
11-07-2019- Zilma Silveira Nogueira Reis ,
- Glaucia Miranda Varella Pereira ,
- Anna Laura Freitas Vianini,
- Marilene Vale Castro Monteiro,
- Regina Amélia Lopes Pessoa Aguiar
Views129See moreAbstract
Objective
To evaluate the association between the upright and supine maternal positions for birth and the incidence of obstetric anal sphincter injuries (OASIs).
Methods
Retrospective cohort study analyzed the data of 1,728 pregnant women who vaginally delivered live single cephalic newborns with a birth weight of 2,500 g. Multiple regression analyses were used to investigate the effect of the supine and upright positions on the incidence of OASIs after adjusting for risk factors and obstetric interventions.
Results
In total, 239 (13.8%) births occurred in upright positions, and 1,489 (86.2%) in supine positions. Grade-III lacerations occurred in 43 (2.5%) patients, and grade-IV lacerations occurred in 3 (0.2%) women. Supine positions had a significant protective effect against severe lacerations, odds ratio [95% confidence interval]: 0,47 [0.22- 0.99], adjusted for the use of forceps 4.80 [2.15-10.70], nulliparity 2.86 [1.44-5.69], and birth weight 3.30 [1.56-7.00]. Anesthesia (p<0.070), oxytocin augmentation (p<0.228), shoulder dystocia (p<0.670), and episiotomy (p<0.559) were not associated with the incidence of severe lacerations.
Conclusion
Upright birth positions were not associated with a lower rate of perineal tears. The interpretation of the findings regarding these positions raised doubts about perineal protection that are still unanswered.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 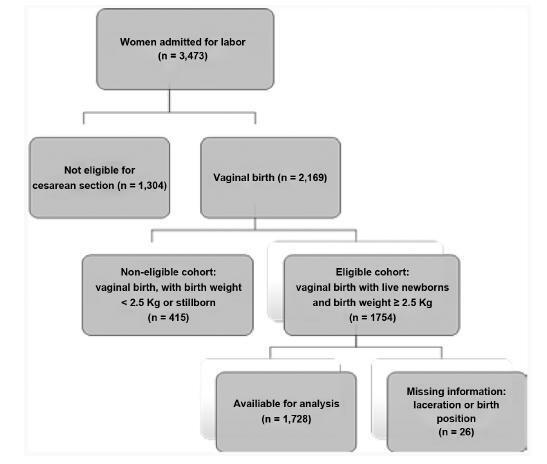
- Zilma Silveira Nogueira Reis
-
Original Article
Factors Associated with Intrapartum Cesarean Section in Women Submitted to Labor Induction
- Glaucia Regina Pfützenreuter,
- Juliana Coutinho Cavalieri,
- Ana Paula de Oliveira Fragoso,
- Karine Souza Da Corregio,
- Paulo Fontoura Freitas, [ ... ],
- Alberto Trapani Júnior
07-22-2019
Summary
Original ArticleFactors Associated with Intrapartum Cesarean Section in Women Submitted to Labor Induction
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(6):363-370
07-22-2019- Glaucia Regina Pfützenreuter,
- Juliana Coutinho Cavalieri,
- Ana Paula de Oliveira Fragoso,
- Karine Souza Da Corregio,
- Paulo Fontoura Freitas,
- Alberto Trapani Júnior
Views147See moreAbstract
Objective
To evaluate the results of induced labor and to determine the main factors associated with intrapartum cesarean section after patients being submitted to this procedure at the Hospital Universitário of the Universidade Federal de Santa Catarina (HU/UFSC, in the Portuguese acronym), Florianópolis, state of Santa Catarina, Brazil.
Methods
A retrospective cross-sectional study that included all the pregnancies that resulted in single-fetus births, whose gestational-age was > 22 weeks and that had been submitted to labor induction at the HU/UFSC in the period from 2013 to 2016.
Results
During the proposed period, 1,491 pregnant women were submitted to the labor induction protocol. In 1,264 cases (84.8%), induction resulted in labor, with 830 (65.7%) progressing to vaginal delivery. Gestational age ≥ 41 + 0 weekswas themost common indication for induced labor (55.2%), and vaginal administration of misoprostol was themost commonly usedmethod (72.0%). Among these pregnant women, the cesarean section rate was of 34.3%. Considering the cases of induction failure, the cesarean section rate rose to 44.3%. The factors associated with cesarean section were: previous history of cesarean delivery (PR [prevalence ratio] = 1.48; 95%CI [confidence interval]: 1.51-1.88), fetuses with intrauterine growth restriction (IUGR) (PR = 1.82; 95%CI: 1.32-2.19), Bishop score ≤ 6 (PR = 1.33; 95%CI: 1.01-1.82), and induction time either < 12 hours (PR = 1.44; 95%CI: 1.17-1.66) or > 36 hours (PR = 1.51; 95% CI 1.22-1.92) between the beginning of the induction and the birth.
Conclusion
Labor induction was successful inmost patients. In the cases in which the final outcome was a cesarean section, the most strongly associated factors were: previous history of cesarean delivery, presence of fetuses with IUGR, and either excessively short or excessively long periods of induction.
Views147This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticleFactors Associated with Intrapartum Cesarean Section in Women Submitted to Labor Induction
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(6):363-370
07-22-2019- Glaucia Regina Pfützenreuter,
- Juliana Coutinho Cavalieri,
- Ana Paula de Oliveira Fragoso,
- Karine Souza Da Corregio,
- Paulo Fontoura Freitas,
- Alberto Trapani Júnior
Views147See moreAbstract
Objective
To evaluate the results of induced labor and to determine the main factors associated with intrapartum cesarean section after patients being submitted to this procedure at the Hospital Universitário of the Universidade Federal de Santa Catarina (HU/UFSC, in the Portuguese acronym), Florianópolis, state of Santa Catarina, Brazil.
Methods
A retrospective cross-sectional study that included all the pregnancies that resulted in single-fetus births, whose gestational-age was > 22 weeks and that had been submitted to labor induction at the HU/UFSC in the period from 2013 to 2016.
Results
During the proposed period, 1,491 pregnant women were submitted to the labor induction protocol. In 1,264 cases (84.8%), induction resulted in labor, with 830 (65.7%) progressing to vaginal delivery. Gestational age ≥ 41 + 0 weekswas themost common indication for induced labor (55.2%), and vaginal administration of misoprostol was themost commonly usedmethod (72.0%). Among these pregnant women, the cesarean section rate was of 34.3%. Considering the cases of induction failure, the cesarean section rate rose to 44.3%. The factors associated with cesarean section were: previous history of cesarean delivery (PR [prevalence ratio] = 1.48; 95%CI [confidence interval]: 1.51-1.88), fetuses with intrauterine growth restriction (IUGR) (PR = 1.82; 95%CI: 1.32-2.19), Bishop score ≤ 6 (PR = 1.33; 95%CI: 1.01-1.82), and induction time either < 12 hours (PR = 1.44; 95%CI: 1.17-1.66) or > 36 hours (PR = 1.51; 95% CI 1.22-1.92) between the beginning of the induction and the birth.
Conclusion
Labor induction was successful inmost patients. In the cases in which the final outcome was a cesarean section, the most strongly associated factors were: previous history of cesarean delivery, presence of fetuses with IUGR, and either excessively short or excessively long periods of induction.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Original Article
Pethidine in Low Doses versus Dipyrone for Pain Relief in Labor: A Randomized Controlled Trial
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):84-89
02-01-2019
Summary
Original ArticlePethidine in Low Doses versus Dipyrone for Pain Relief in Labor: A Randomized Controlled Trial
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):84-89
02-01-2019Views109See moreAbstract
Objective
To compare low doses of pethidine with dipyrone in labor analgesia.
Methods
In a randomized prospective study conducted by Universidade de Fortaleza, in the state of Ceará, Brazil, between May and December 2016, 200 full-term parturients, with very painful uterine contractions and exhibiting uterine cervix dilatation ≥ 5 cm, were selected to receive a single intravenous dose of either 0.25 mg/kg of pethidine (n = 100) or of 25 mg/kg of dipyrone (n = 100). Pain was assessed using the visual analogue scale. The data were analyzed using the Student t-test, the chi-square test and the likelihood ratio.
Results
There was a significant improvement in pain in 35% of the parturients. Both drugs presented a similar analgesic effect 1 hour after the intervention (p = 0.692). There was no analgesic effect during the evaluation of the second hour after the intervention with pethidine or dipyrone. There were no adverse effects, such as maternal drowsiness, nausea or vomiting, related to the drugs used.
Conclusion
Pethidine in low doses and dipyrone presented equivalent analgesia during labor. Public Registry of Clinical Trials.
Views109This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Summary
Original ArticlePethidine in Low Doses versus Dipyrone for Pain Relief in Labor: A Randomized Controlled Trial
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):84-89
02-01-2019Views109See moreAbstract
Objective
To compare low doses of pethidine with dipyrone in labor analgesia.
Methods
In a randomized prospective study conducted by Universidade de Fortaleza, in the state of Ceará, Brazil, between May and December 2016, 200 full-term parturients, with very painful uterine contractions and exhibiting uterine cervix dilatation ≥ 5 cm, were selected to receive a single intravenous dose of either 0.25 mg/kg of pethidine (n = 100) or of 25 mg/kg of dipyrone (n = 100). Pain was assessed using the visual analogue scale. The data were analyzed using the Student t-test, the chi-square test and the likelihood ratio.
Results
There was a significant improvement in pain in 35% of the parturients. Both drugs presented a similar analgesic effect 1 hour after the intervention (p = 0.692). There was no analgesic effect during the evaluation of the second hour after the intervention with pethidine or dipyrone. There were no adverse effects, such as maternal drowsiness, nausea or vomiting, related to the drugs used.
Conclusion
Pethidine in low doses and dipyrone presented equivalent analgesia during labor. Public Registry of Clinical Trials.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.