Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):235-238
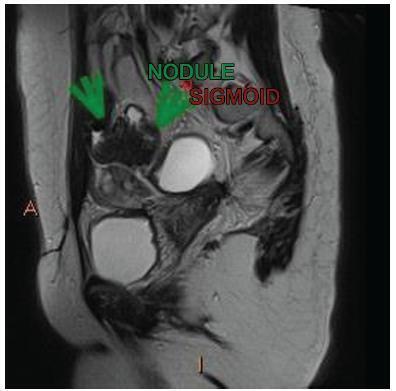
We report the case of a 33 year-old woman who complained of severe dysmenorrhea since menarche. From 2003 to 2009, she underwent 4 laparoscopies for the treatment of pain associated with endometriosis. After all four interventions, the pain recurred despite the use of gonadotropin-releasing hormone (GnRH) analogues and the insertion of a levonorgestrel intrauterine system (LNG-IUS). Finally, a colonoscopy performed in 2010 revealed rectosigmoid stenosis probably due to extrinsic compression. The patient was advised to get pregnant before treating the intestinal lesion. Spontaneous pregnancy occurred soon after LNG-IUS removal in 2011. In the 33rd week of pregnancy, the patient started to feel severe abdominal pain. No fever or sings of pelviperitonitis were present, but as the pain worsened, a cesarean section was performed, with the delivery of a premature healthy male, and an intestinal rupturewas identified. Severe peritoneal infection and sepsis ensued. A colostomy was performed, and the patient recovered after eight days in intensive care. Three months later, the colostomy was closed, and a new LNG-IUS was inserted. The patient then came to be treated by our multidisciplinary endometriosis team. The diagnostic evaluation revealed the presence of intestinal lesions with extrinsic compression of the rectum. She then underwent a laparoscopic excision of the endometriotic lesions, including an ovarian endometrioma, adhesiolysis and segmental colectomy in 2014. She is now fully recovered and planning a new pregnancy. A transvaginal ultrasound (TVUS) performed six months after surgery showed signs of pelvic adhesions, but no endometriotic lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):235-238
We report the case of a 33 year-old woman who complained of severe dysmenorrhea since menarche. From 2003 to 2009, she underwent 4 laparoscopies for the treatment of pain associated with endometriosis. After all four interventions, the pain recurred despite the use of gonadotropin-releasing hormone (GnRH) analogues and the insertion of a levonorgestrel intrauterine system (LNG-IUS). Finally, a colonoscopy performed in 2010 revealed rectosigmoid stenosis probably due to extrinsic compression. The patient was advised to get pregnant before treating the intestinal lesion. Spontaneous pregnancy occurred soon after LNG-IUS removal in 2011. In the 33rd week of pregnancy, the patient started to feel severe abdominal pain. No fever or sings of pelviperitonitis were present, but as the pain worsened, a cesarean section was performed, with the delivery of a premature healthy male, and an intestinal rupturewas identified. Severe peritoneal infection and sepsis ensued. A colostomy was performed, and the patient recovered after eight days in intensive care. Three months later, the colostomy was closed, and a new LNG-IUS was inserted. The patient then came to be treated by our multidisciplinary endometriosis team. The diagnostic evaluation revealed the presence of intestinal lesions with extrinsic compression of the rectum. She then underwent a laparoscopic excision of the endometriotic lesions, including an ovarian endometrioma, adhesiolysis and segmental colectomy in 2014. She is now fully recovered and planning a new pregnancy. A transvaginal ultrasound (TVUS) performed six months after surgery showed signs of pelvic adhesions, but no endometriotic lesions.