Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):178-185
DOI 10.1590/SO100-720320150005184
To conduct a comparative study between two groups of women (HIV positive and negative) analyzing: the prevalence of cervical intraepithelial neoplasia (CIN) and cervical HPV infection; viral risk and relationship with development of CIN; and sociodemographic and behavioral parameters that influence cervical HPV infection and the development of CIN.
A cross-sectional study in which 202 HIV-positive women and 164 HIV-negative women were analyzed to assess the prevalence of CIN and 171 HIV-positive women and 160 HIV-negative women were analyzed to assess the prevalence of cervical HPV infection. The following procedures were performed on the occasion of each medical visit: collection of cervical samples for cytology and polymerase chain reaction (PCR) to detect HPV DNA; colposcopy; standardized questionnaire to collect demographic and behavioral data; and biopsy of all colposcopic changes. Histopathology was the gold standard for the diagnosis of CIN.
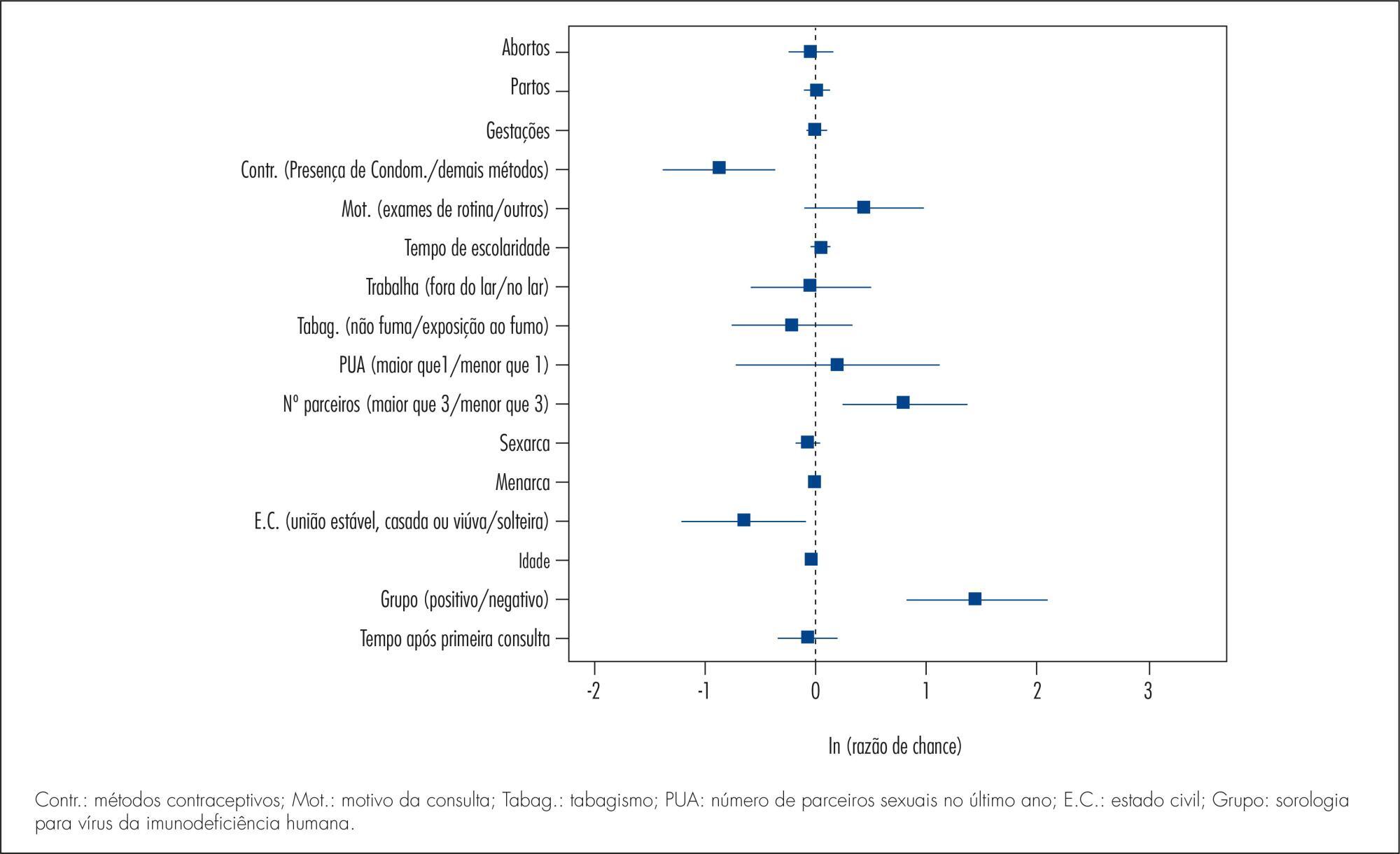
The prevalence of CIN was 2.4 and 15.3% (p<0.001) and the prevalence of cervical HPV infection was 37.1 and 55.5% (p=0.002), respectively, among HIV-negative and -positive women. HIV-positive women had a higher risk of HPV infection (35.7 and 23.6%) (p=0.02). HPV 16 was the most prevalent virus type, occurring in 11.3 and 10.2% of HIV-positive and negative women and was also more prevalent among women presenting CIN in both groups. Factors associated fwith the development of CIN were: HIV infection (HT=4.64; 95%CI 2.23-9.65), age (HT=0.95; 95%CI 0.93-0.98 for each year of life) and marital status(HT=0.49; 95%CI 0.30-0.80). Associated factors for HPV infection were: HIV presence (HT=2.72; 95%CI 1.77-4.17), greater number of sexual partners (HT=1.87; 95%CI 1.23-2.84), age (HT=0.97; 95%CI 0.95-0.99 for each year of life) and marital status (HT=0.65; 95%CI 0.42-1.0 for stable union/widows).
The prevalence of CIN and cervical HPV infection was higher in HIV-positive women, who also presented a higher risk of HPV infections and multiple viral types. Type 16 was predominant in both groups and in women with CIN. Older women and women with stable union/widows were less likely to acquire cervical HPV infection and CIN.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):178-185
DOI 10.1590/SO100-720320150005184
To conduct a comparative study between two groups of women (HIV positive and negative) analyzing: the prevalence of cervical intraepithelial neoplasia (CIN) and cervical HPV infection; viral risk and relationship with development of CIN; and sociodemographic and behavioral parameters that influence cervical HPV infection and the development of CIN.
A cross-sectional study in which 202 HIV-positive women and 164 HIV-negative women were analyzed to assess the prevalence of CIN and 171 HIV-positive women and 160 HIV-negative women were analyzed to assess the prevalence of cervical HPV infection. The following procedures were performed on the occasion of each medical visit: collection of cervical samples for cytology and polymerase chain reaction (PCR) to detect HPV DNA; colposcopy; standardized questionnaire to collect demographic and behavioral data; and biopsy of all colposcopic changes. Histopathology was the gold standard for the diagnosis of CIN.
The prevalence of CIN was 2.4 and 15.3% (p<0.001) and the prevalence of cervical HPV infection was 37.1 and 55.5% (p=0.002), respectively, among HIV-negative and -positive women. HIV-positive women had a higher risk of HPV infection (35.7 and 23.6%) (p=0.02). HPV 16 was the most prevalent virus type, occurring in 11.3 and 10.2% of HIV-positive and negative women and was also more prevalent among women presenting CIN in both groups. Factors associated fwith the development of CIN were: HIV infection (HT=4.64; 95%CI 2.23-9.65), age (HT=0.95; 95%CI 0.93-0.98 for each year of life) and marital status(HT=0.49; 95%CI 0.30-0.80). Associated factors for HPV infection were: HIV presence (HT=2.72; 95%CI 1.77-4.17), greater number of sexual partners (HT=1.87; 95%CI 1.23-2.84), age (HT=0.97; 95%CI 0.95-0.99 for each year of life) and marital status (HT=0.65; 95%CI 0.42-1.0 for stable union/widows).
The prevalence of CIN and cervical HPV infection was higher in HIV-positive women, who also presented a higher risk of HPV infections and multiple viral types. Type 16 was predominant in both groups and in women with CIN. Older women and women with stable union/widows were less likely to acquire cervical HPV infection and CIN.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):179-185
We describe the development and structure of a novel mobile application in a mixed model of prenatal care, in the context of the COVID-19 pandemic. Furthermore, we assess the acceptability of this mobile app in a cohort of patients.
First, we introduced a mixed model of prenatal care; second, we developed a comprehensive, computer-based clinical record to support our system. Lastly, we built a novel mobile app as a tool for prenatal care. We used Flutter Software version 2.2 to build the app for Android and iOS smartphones. A cross-sectional study was carried out to assess the acceptability of the app.
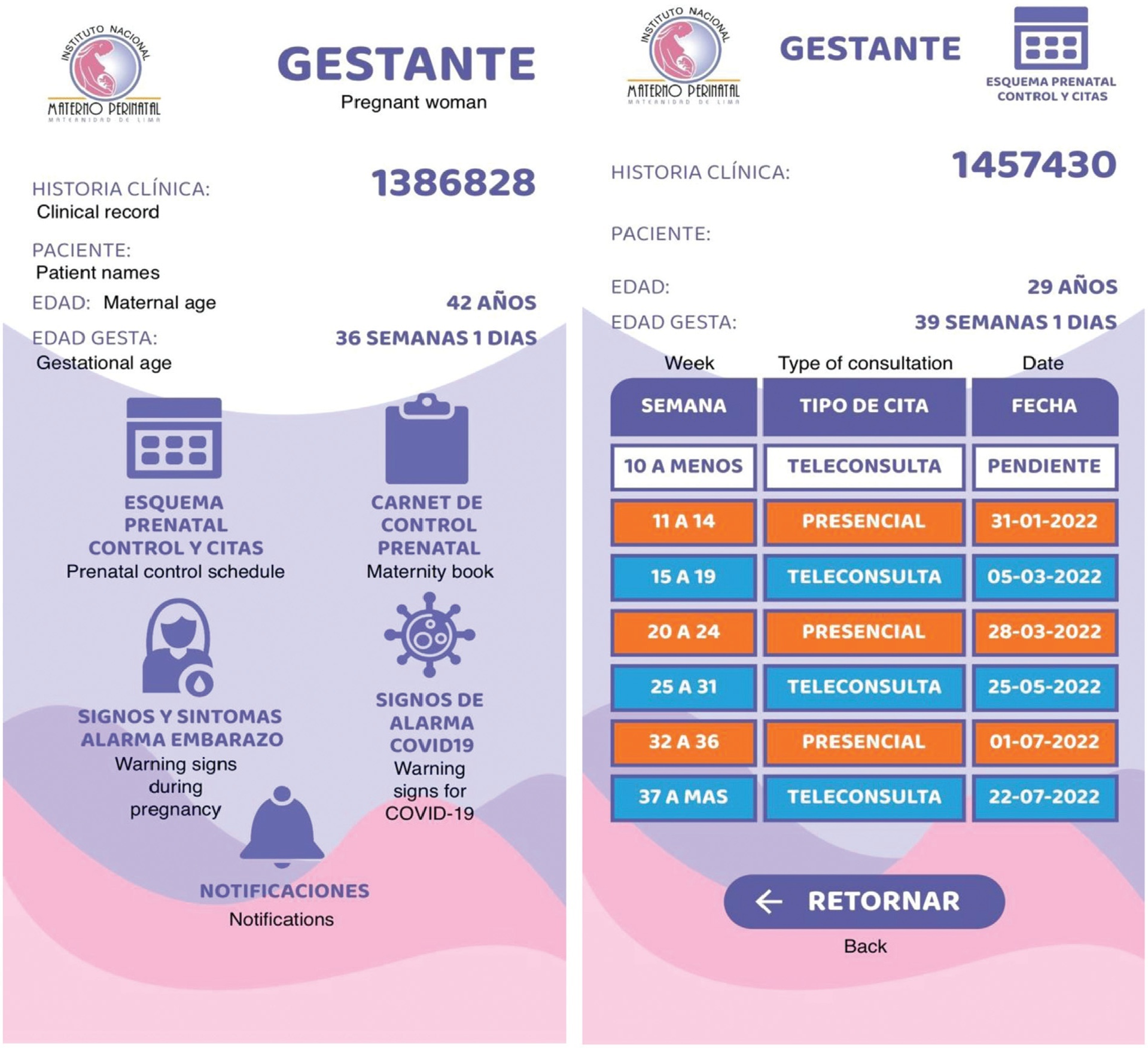
A mobile app was also built with the main attribute of being connected in real-time with the computer-based clinical records. The app screens detail information about activities programmed and developed in the prenatal care according to gestational age. A downloadable maternity book is available and some screens show warning signs and symptoms of pregnancy. The acceptability assessment was mostly rated positively regarding the characteristics of the mobile app, by 50 patients.
This novel mobile app was developed as a tool among pregnant patients to increase the information available about their pregnancies in the provision of a mixed model of prenatal care in the context of the COVID-19 pandemic. It was fully customized to the needs of our users following the local protocols. The introduction of this novel mobile app was highly accepted by the patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):179-185
We describe the development and structure of a novel mobile application in a mixed model of prenatal care, in the context of the COVID-19 pandemic. Furthermore, we assess the acceptability of this mobile app in a cohort of patients.
First, we introduced a mixed model of prenatal care; second, we developed a comprehensive, computer-based clinical record to support our system. Lastly, we built a novel mobile app as a tool for prenatal care. We used Flutter Software version 2.2 to build the app for Android and iOS smartphones. A cross-sectional study was carried out to assess the acceptability of the app.
A mobile app was also built with the main attribute of being connected in real-time with the computer-based clinical records. The app screens detail information about activities programmed and developed in the prenatal care according to gestational age. A downloadable maternity book is available and some screens show warning signs and symptoms of pregnancy. The acceptability assessment was mostly rated positively regarding the characteristics of the mobile app, by 50 patients.
This novel mobile app was developed as a tool among pregnant patients to increase the information available about their pregnancies in the provision of a mixed model of prenatal care in the context of the COVID-19 pandemic. It was fully customized to the needs of our users following the local protocols. The introduction of this novel mobile app was highly accepted by the patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(4):179-179
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(4):179-179
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(3):179-183
DOI 10.1590/S0100-72032006000300007
PURPOSE: to diagnose and treat diabetic pregnant women with antiphospholipid antibodies and to describe the gestational and perinatal results. METHODS: we evaluated 56 gestational and pregestational diabetic women who were attended at one specialized prenatal care unit, between July 2003 and March 2004. All of them had a blood test to quantify antiphospholipid antibodies. If positive, they were treated with heparin and aspirin at low doses and the usual treatment for diabetes. We calculated the prevalence and 95% confidence interval for all and also those for the pregestational ones. The characteristics of the pregnancies and the newborns are described. RESULTS: antiphospholipid antibodies prevalence among the diabetic pregnant women was 7% (95% CI - 0.1 to 13.9). Among pregestational diabetic women it was 12% (95% CI - 0.2 to 23.3). Among the diabetic women with antiphospholipid antibodies the duration of disease was five years or more. Maternal age in positive antiphospholipid antibodies diabetics ranged from 27 to 38 years; one was primiparous, another was secundiparous and two were multiparous. CONCLUSION: antiphospholipid antibodies prevalence in diabetic pregnant women was similar to that in the general population and lower than that of the pregestational diabetic women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(3):179-183
DOI 10.1590/S0100-72032006000300007
PURPOSE: to diagnose and treat diabetic pregnant women with antiphospholipid antibodies and to describe the gestational and perinatal results. METHODS: we evaluated 56 gestational and pregestational diabetic women who were attended at one specialized prenatal care unit, between July 2003 and March 2004. All of them had a blood test to quantify antiphospholipid antibodies. If positive, they were treated with heparin and aspirin at low doses and the usual treatment for diabetes. We calculated the prevalence and 95% confidence interval for all and also those for the pregestational ones. The characteristics of the pregnancies and the newborns are described. RESULTS: antiphospholipid antibodies prevalence among the diabetic pregnant women was 7% (95% CI - 0.1 to 13.9). Among pregestational diabetic women it was 12% (95% CI - 0.2 to 23.3). Among the diabetic women with antiphospholipid antibodies the duration of disease was five years or more. Maternal age in positive antiphospholipid antibodies diabetics ranged from 27 to 38 years; one was primiparous, another was secundiparous and two were multiparous. CONCLUSION: antiphospholipid antibodies prevalence in diabetic pregnant women was similar to that in the general population and lower than that of the pregestational diabetic women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(1):18-26
DOI 10.1590/S0100-72032007000100004
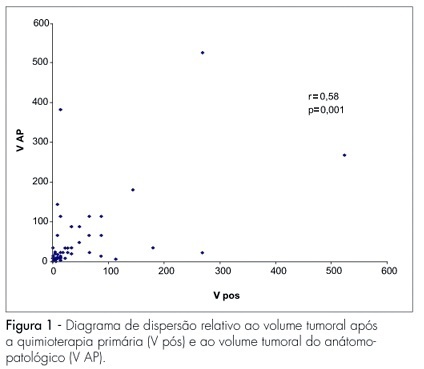
PURPOSE: to evaluate the loco-regional response to primary chemotherapy in patients with breast cancer at stages II and III. METHODS: a retrospective and analytical clinical study carried out in 97 patients with an average age of 52.2 years old, with breast cancer at stages II and III, attended from January 1993 to December 2004, and submitted to 3 to 4 cycles of primary chemotherapy with 5-fluorouracil - 500 mg/m2, epirubicin - 50 mg/m2 and cyclophosphamide - 500 mg/m2 or doxorubicin - 50 mg/m2 e cyclophosphamide - 500 mg/m2, and then to loco-regional surgical conservative or radical surgical treatment. Chi-square and Fisher’s exact tests were used to study the association among the variables (age, menopausal state, pre-chemotherapy tumoral volume, axillary condition, stage, therapeutic scheme and number of cycles), while Pearson’s correlation coefficient was used for the quantitative variables (tumoral volume according to the anatomo-pathological study and the post-chemotherapy clinical tumoral volume. The significance level was 5%. RESULTS: there were 56.8% of cases at stage II and 43.2% at stage III. Approximately 50% of the patients received FEC50 and 50% AC. Objective clinical response with primary chemotherapy was obtained in 64.9% of the cases. Full clinical response occurred in 12.3% of patients, while full pathological response occurred in 10.3% of the cases. CONCLUSIONS: there was a statistically significant correlation between the number of cycles and the response to primary chemotherapy. Patients who received 4 cycles had better response than those who received 3 cycles. There was also a statistically significant concordance between the evaluation through clinical examination of the response to primary chemotherapy and the pathological findings. No statistically significant correlation was observed concerning age, menopausal status, tumoral volume, and pretreatment of axillary damage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(1):18-26
DOI 10.1590/S0100-72032007000100004
PURPOSE: to evaluate the loco-regional response to primary chemotherapy in patients with breast cancer at stages II and III. METHODS: a retrospective and analytical clinical study carried out in 97 patients with an average age of 52.2 years old, with breast cancer at stages II and III, attended from January 1993 to December 2004, and submitted to 3 to 4 cycles of primary chemotherapy with 5-fluorouracil - 500 mg/m2, epirubicin - 50 mg/m2 and cyclophosphamide - 500 mg/m2 or doxorubicin - 50 mg/m2 e cyclophosphamide - 500 mg/m2, and then to loco-regional surgical conservative or radical surgical treatment. Chi-square and Fisher’s exact tests were used to study the association among the variables (age, menopausal state, pre-chemotherapy tumoral volume, axillary condition, stage, therapeutic scheme and number of cycles), while Pearson’s correlation coefficient was used for the quantitative variables (tumoral volume according to the anatomo-pathological study and the post-chemotherapy clinical tumoral volume. The significance level was 5%. RESULTS: there were 56.8% of cases at stage II and 43.2% at stage III. Approximately 50% of the patients received FEC50 and 50% AC. Objective clinical response with primary chemotherapy was obtained in 64.9% of the cases. Full clinical response occurred in 12.3% of patients, while full pathological response occurred in 10.3% of the cases. CONCLUSIONS: there was a statistically significant correlation between the number of cycles and the response to primary chemotherapy. Patients who received 4 cycles had better response than those who received 3 cycles. There was also a statistically significant concordance between the evaluation through clinical examination of the response to primary chemotherapy and the pathological findings. No statistically significant correlation was observed concerning age, menopausal status, tumoral volume, and pretreatment of axillary damage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(1):18-24
DOI 10.1590/S0100-72031999000100004
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(1):18-24
DOI 10.1590/S0100-72031999000100004
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(1):18-23
DOI 10.1590/S0100-72032006000100004
PURPOSE: to characterize postmenopausal endometrial polyps and to determine risk for concomitant premalignant and malignant pathology. METHODS: a retrospective study including 82 postmenopausal women with a histological diagnosis of endometrial polyps who underwent hysteroscopic polypectomy, after a diagnosis of endometrial thickening made by transvaginal ultrasound, was performed. Medical reports provided clinical and gynecological history, data related to the operative hysteroscopy and definitive histological findings. RESULTS: among the 82 patients who underwent hysteroscopic polypectomy, 10.9% were receiving some type of hormonal therapy. Twenty-eight women (34.1%) reported abnormal vaginal bleeding. Single polyp was encountered in 56 women (68.3%), two polyps were found in 19 cases (23.2%) and in 7 cases (3.6%), three or more polyps were found. The definitive histopathologic analysis revealed 63 (76.8%) benign polyps, 17 (20.8%) hyperplastic polyps (10 cases 12.2% - of simple endometrial hyperplasia without cytologic atypia and 7 cases 8.6% - of complex endometrial hyperplasia without cytologic atypia). Two polyps (2.4%) were diagnosed as harboring neoplasia. For the statistical analysis we employed chi2 test improved by Yates. The authors correlated the polyps' histology with the occurrence of abnormal vaginal bleeding (p=0.0056), number of endometrial polyps (p=0.921) and time after menopause (p=0.720). CONCLUSIONS: endometrial polyps are commonly found entities in postmenopausal women, related with low frequency to endometrial hyperplasia or carcinomas and only histological evaluation seems to allow the exclusion of premalignant and malignant pathology.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(1):18-23
DOI 10.1590/S0100-72032006000100004
PURPOSE: to characterize postmenopausal endometrial polyps and to determine risk for concomitant premalignant and malignant pathology. METHODS: a retrospective study including 82 postmenopausal women with a histological diagnosis of endometrial polyps who underwent hysteroscopic polypectomy, after a diagnosis of endometrial thickening made by transvaginal ultrasound, was performed. Medical reports provided clinical and gynecological history, data related to the operative hysteroscopy and definitive histological findings. RESULTS: among the 82 patients who underwent hysteroscopic polypectomy, 10.9% were receiving some type of hormonal therapy. Twenty-eight women (34.1%) reported abnormal vaginal bleeding. Single polyp was encountered in 56 women (68.3%), two polyps were found in 19 cases (23.2%) and in 7 cases (3.6%), three or more polyps were found. The definitive histopathologic analysis revealed 63 (76.8%) benign polyps, 17 (20.8%) hyperplastic polyps (10 cases 12.2% - of simple endometrial hyperplasia without cytologic atypia and 7 cases 8.6% - of complex endometrial hyperplasia without cytologic atypia). Two polyps (2.4%) were diagnosed as harboring neoplasia. For the statistical analysis we employed chi2 test improved by Yates. The authors correlated the polyps' histology with the occurrence of abnormal vaginal bleeding (p=0.0056), number of endometrial polyps (p=0.921) and time after menopause (p=0.720). CONCLUSIONS: endometrial polyps are commonly found entities in postmenopausal women, related with low frequency to endometrial hyperplasia or carcinomas and only histological evaluation seems to allow the exclusion of premalignant and malignant pathology.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):180-187
To assess the effectiveness of metformin in the incidence of gestational diabetes mellitus (GDM) in obese pregnant women attending a public maternity hospital in Joinville, Santa Catarina, Brazil.
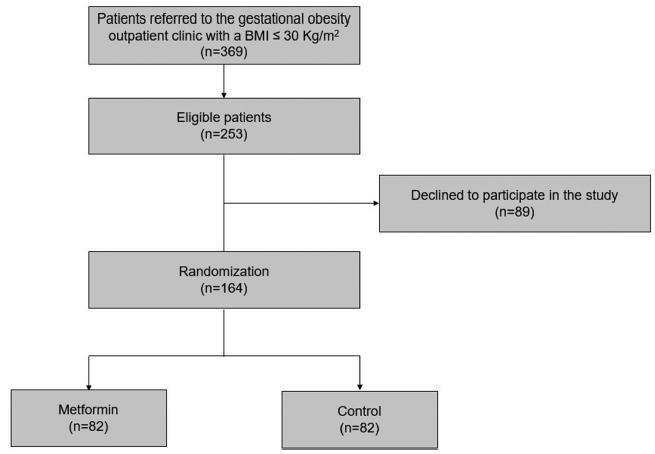
Randomized clinical trial including obese pregnant women with a body mass index (BMI) ≥ 30 kg/m2, divided into two groups (control and metformin). Both groups received guidance regarding diet and physical exercise. The participants were assessed at two moments, the first at enrollment (gestational age ≤ 20) and the second at gestational weeks 24-28. The outcomes assessed were BMI and gestational diabetes mellitus (GDM) diagnosis. The data distribution was assessed with the Friedman test. For all the analytical models, the p-values were considered significant when lower than 0.05. The absolute risk reduction was also estimated.
Overall, 164 pregnant women were assessed and further divided into 82 participants per group. No significant difference was observed in BMI variation between the control and metformin groups (0.9 ± 1.2 versus 1.0 ± 0.9, respectively, p = 0.63). Gestational diabetes mellitus was diagnosed in 15.9% (n = 13) of the patients allocated to the metformin group and 19.5% (n = 16) of those in the control group (p = 0.683). The absolute risk reduction was 3.6 (95% confidence interval 8.0- 15.32) in the group treated with metformin, which was not significant.
Metformin was not effective in reducing BMI and preventing GDM in obese pregnant women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):180-187
To assess the effectiveness of metformin in the incidence of gestational diabetes mellitus (GDM) in obese pregnant women attending a public maternity hospital in Joinville, Santa Catarina, Brazil.
Randomized clinical trial including obese pregnant women with a body mass index (BMI) ≥ 30 kg/m2, divided into two groups (control and metformin). Both groups received guidance regarding diet and physical exercise. The participants were assessed at two moments, the first at enrollment (gestational age ≤ 20) and the second at gestational weeks 24-28. The outcomes assessed were BMI and gestational diabetes mellitus (GDM) diagnosis. The data distribution was assessed with the Friedman test. For all the analytical models, the p-values were considered significant when lower than 0.05. The absolute risk reduction was also estimated.
Overall, 164 pregnant women were assessed and further divided into 82 participants per group. No significant difference was observed in BMI variation between the control and metformin groups (0.9 ± 1.2 versus 1.0 ± 0.9, respectively, p = 0.63). Gestational diabetes mellitus was diagnosed in 15.9% (n = 13) of the patients allocated to the metformin group and 19.5% (n = 16) of those in the control group (p = 0.683). The absolute risk reduction was 3.6 (95% confidence interval 8.0- 15.32) in the group treated with metformin, which was not significant.
Metformin was not effective in reducing BMI and preventing GDM in obese pregnant women.