Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(3):158-164
DOI 10.1590/S0100-72032007000300008
Axillary nodal metastasis is still the most important breast cancer prognostic factor. As in approximately 80% of the patients with tumors measuring less than 2 cm the axillary lymph nodes are negative, it has been proposed sentinel lymph node biopsy, reducing surgical morbidity in the patients with negative result. Recently, this technique has been widely used in Brazil, but there are two questions that need to be answered: what is the probability of a false-negative result (not diagnosing a positive lymph node) and if the understaging by false-negative result exposes the patient to the risk of axillary recurrence or even distant metastases, due to less effective surgical and adjuvant therapy. The literature shows that the false-negative rate varies from 5 to 10%, being the surgeon's experience the major factor that contributes to improved results. Although axillary relapse is rare, it is not yet possible to evaluate the long term effect of not removing positive lymph nodes, due to short follow-up. The recommendation is that sentinel lymph node biopsy should only be performed by surgeons with experience confirmed by a low false-negative rate.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(3):158-164
DOI 10.1590/S0100-72032007000300008
Axillary nodal metastasis is still the most important breast cancer prognostic factor. As in approximately 80% of the patients with tumors measuring less than 2 cm the axillary lymph nodes are negative, it has been proposed sentinel lymph node biopsy, reducing surgical morbidity in the patients with negative result. Recently, this technique has been widely used in Brazil, but there are two questions that need to be answered: what is the probability of a false-negative result (not diagnosing a positive lymph node) and if the understaging by false-negative result exposes the patient to the risk of axillary recurrence or even distant metastases, due to less effective surgical and adjuvant therapy. The literature shows that the false-negative rate varies from 5 to 10%, being the surgeon's experience the major factor that contributes to improved results. Although axillary relapse is rare, it is not yet possible to evaluate the long term effect of not removing positive lymph nodes, due to short follow-up. The recommendation is that sentinel lymph node biopsy should only be performed by surgeons with experience confirmed by a low false-negative rate.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(3):158-164
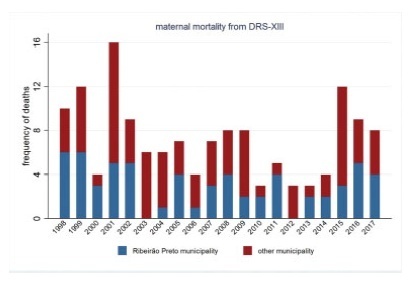
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(3):158-164
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(3):158-164
DOI 10.1590/S0100-72032006000300004
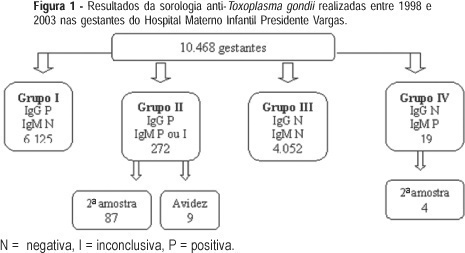
PURPOSE: to describe and analyze the results of conventional serology for toxoplasmosis in pregnant women during prenatal care at the Hospital Materno-Infantil Presidente Vargas in Porto Alegre. METHODS: specific IgG and IgM determinations were performed using fluorometric tests, with IgM capture. A second sample within two to three weeks was requested from all IgM-positive pregnant women and IgG avidity was performed in IgM-positive pregnant women at the beginning of pregnancy. Neonatal IgM was obtained when the delivery occurred at the institution. The analysis was based on the binomial distribution, through simple ratio estimate, to assess soropositivity prevalence and susceptibility to T. gondi infection. RESULTS: the prevalence of infection in 10,468 pregnant women was 61.1% and 38.7% pregnant women were susceptible. Among the 272 IgG and IgM-positive pregnant women, 87 returned for a second test and in 84 of them the antibody levels remained unchanged. Of nine pregnant women with avidity, there was only one low avidity and her newborn was IgM positive. In 44 newborns delivered at the institution, the neonatal IgM was positive in four. CONCLUSIONS: a high prevalence of infection and congenital toxoplasmosis was found in pregnant women, even without data on seroconversion. Most of the IgM-positive serologies were related to past infection. The cost-benefit ratio of prenatal care in isolated samples may be optimized analyzing the risk of mother-to-child transmission in IgM-positive pregnant women. When there is a risk, a neonatal IgM test must be requested and the newborn should be followed during the first year of life.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(3):158-164
DOI 10.1590/S0100-72032006000300004
PURPOSE: to describe and analyze the results of conventional serology for toxoplasmosis in pregnant women during prenatal care at the Hospital Materno-Infantil Presidente Vargas in Porto Alegre. METHODS: specific IgG and IgM determinations were performed using fluorometric tests, with IgM capture. A second sample within two to three weeks was requested from all IgM-positive pregnant women and IgG avidity was performed in IgM-positive pregnant women at the beginning of pregnancy. Neonatal IgM was obtained when the delivery occurred at the institution. The analysis was based on the binomial distribution, through simple ratio estimate, to assess soropositivity prevalence and susceptibility to T. gondi infection. RESULTS: the prevalence of infection in 10,468 pregnant women was 61.1% and 38.7% pregnant women were susceptible. Among the 272 IgG and IgM-positive pregnant women, 87 returned for a second test and in 84 of them the antibody levels remained unchanged. Of nine pregnant women with avidity, there was only one low avidity and her newborn was IgM positive. In 44 newborns delivered at the institution, the neonatal IgM was positive in four. CONCLUSIONS: a high prevalence of infection and congenital toxoplasmosis was found in pregnant women, even without data on seroconversion. Most of the IgM-positive serologies were related to past infection. The cost-benefit ratio of prenatal care in isolated samples may be optimized analyzing the risk of mother-to-child transmission in IgM-positive pregnant women. When there is a risk, a neonatal IgM test must be requested and the newborn should be followed during the first year of life.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(4):159-163
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(4):159-163
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):159-163
DOI 10.1590/SO100-720320150004973
To analyze the relationship between route of delivery and other aspects of pregnancy and the occurrence of intracranial hemorrhage in newborns of very low weight at a teaching hospital in South Brazil.
A case-control study was conducted. Medical records of all patients who were born weighing ≤1,500 g and who were submitted to transfontanellar ultrasonography were analyzed from January 2011 to September 2014. The cases were newborns with diagnosis of intracranial hemorrhage, while newborns with regular exams were used as controls. Differences between groups were analyzed by the Student t test and by χ2 or Fisher exact tests, and association was determined using the odds ratio with a 95% confidence interval and α=5%.
A total of 222 newborns with birth weight ≤1,500 g were recorded; of these, 113 were submitted to transfontanellar ultrasonography and were included in the study. Sixty-nine (61.1%) newborns were diagnosed with intracranial hemorrhage (cases) and 44 (38.9%) showed no abnormal results (controls). Most cases had grade I hemorrhage (96.8%) originating from the germinative matrix (95.7%). The predominant route of delivery was caesarean section (81.2% of the cases and 72.7% of the controls). Five deaths were recorded (3 cases and 2 controls). Gestational age ranged from 24 to 37 weeks. Median birth weight was 1,205 g (range: 675-1,500 g). The median time of hospitalization was 52 days, ranging from 5 to 163 days.
Grade I intracranial hemorrhage from the germinative matrix was the most frequent. No differences were found between cases and controls for the variables studied. The small number of infants submitted to transfontanellar ultrasonography limited the sample size and the results of the study.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):159-163
DOI 10.1590/SO100-720320150004973
To analyze the relationship between route of delivery and other aspects of pregnancy and the occurrence of intracranial hemorrhage in newborns of very low weight at a teaching hospital in South Brazil.
A case-control study was conducted. Medical records of all patients who were born weighing ≤1,500 g and who were submitted to transfontanellar ultrasonography were analyzed from January 2011 to September 2014. The cases were newborns with diagnosis of intracranial hemorrhage, while newborns with regular exams were used as controls. Differences between groups were analyzed by the Student t test and by χ2 or Fisher exact tests, and association was determined using the odds ratio with a 95% confidence interval and α=5%.
A total of 222 newborns with birth weight ≤1,500 g were recorded; of these, 113 were submitted to transfontanellar ultrasonography and were included in the study. Sixty-nine (61.1%) newborns were diagnosed with intracranial hemorrhage (cases) and 44 (38.9%) showed no abnormal results (controls). Most cases had grade I hemorrhage (96.8%) originating from the germinative matrix (95.7%). The predominant route of delivery was caesarean section (81.2% of the cases and 72.7% of the controls). Five deaths were recorded (3 cases and 2 controls). Gestational age ranged from 24 to 37 weeks. Median birth weight was 1,205 g (range: 675-1,500 g). The median time of hospitalization was 52 days, ranging from 5 to 163 days.
Grade I intracranial hemorrhage from the germinative matrix was the most frequent. No differences were found between cases and controls for the variables studied. The small number of infants submitted to transfontanellar ultrasonography limited the sample size and the results of the study.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(3):159-165
DOI 10.1590/S0100-72032001000300005
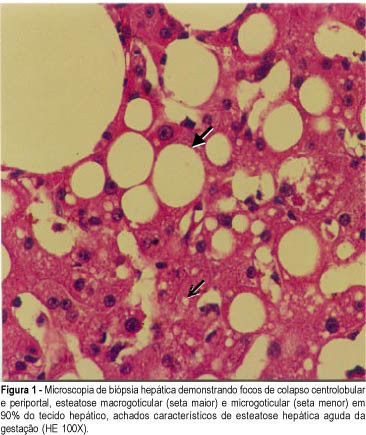
Purpose: to evaluate the diagnostic difficulties, treatment and outcome in cases of acute liver failure of pregnancy. Methods: seven patients with acute liver failure of pregnancy, managed during the past 4 years, were studied with emphasis on presenting symptoms, laboratory findings, clinical course, maternal complications and fetal outcome. Results: the mean age was 25.8 years (two were primigravidas), and the mean gestational age at onset was 30.1 weeks. The final diagnosis was acute fatty liver of pregnancy in four cases and intrahepatic cholestasis of pregnancy in three cases. Anorexia, nausea, abdominal pain, jaundice and encephalopathy were the main clinical findings. Two maternal deaths occurred: one due to hepatic failure, while waiting for transplantation, and another due to hepatic failure associated with coagulopathy and major intra-abdominal bleeding after liver biopsy. One patient with acute fatty liver of pregnancy underwent a successful liver transplantation one year ago (after chronification of her disease). The remaining four cases had complete resolution of the disorders after delivery and supportive measures. Maternal and fetal mortalities were 28.6% and 57.1%, respectively. Conclusion: from this initial experience, we conclude that acute liver failure of pregnancy is a serious disease, with high maternal-fetal mortality, and that early recognition of this illness, referral to tertiary liver centers, and prompt interruption of gestation are, together, very important for the success of the treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(3):159-165
DOI 10.1590/S0100-72032001000300005
Purpose: to evaluate the diagnostic difficulties, treatment and outcome in cases of acute liver failure of pregnancy. Methods: seven patients with acute liver failure of pregnancy, managed during the past 4 years, were studied with emphasis on presenting symptoms, laboratory findings, clinical course, maternal complications and fetal outcome. Results: the mean age was 25.8 years (two were primigravidas), and the mean gestational age at onset was 30.1 weeks. The final diagnosis was acute fatty liver of pregnancy in four cases and intrahepatic cholestasis of pregnancy in three cases. Anorexia, nausea, abdominal pain, jaundice and encephalopathy were the main clinical findings. Two maternal deaths occurred: one due to hepatic failure, while waiting for transplantation, and another due to hepatic failure associated with coagulopathy and major intra-abdominal bleeding after liver biopsy. One patient with acute fatty liver of pregnancy underwent a successful liver transplantation one year ago (after chronification of her disease). The remaining four cases had complete resolution of the disorders after delivery and supportive measures. Maternal and fetal mortalities were 28.6% and 57.1%, respectively. Conclusion: from this initial experience, we conclude that acute liver failure of pregnancy is a serious disease, with high maternal-fetal mortality, and that early recognition of this illness, referral to tertiary liver centers, and prompt interruption of gestation are, together, very important for the success of the treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(3):159-165
DOI 10.1590/S0100-72032000000300007
Purpose: to determine the frequency of recurrence of seizures after anticonvulsant therapy with magnesium sulfate and to evaluate treatment and maternal prognosis. Patients and Methods: a prospective cohort study was conducted, enrolling all cases of eclampsia managed at IMIP between January/1995 and June/1998. Magnesium sulfate and oxygen therapy were administered routinely and interruption of pregnancy was performed after maternal stabilization. The frequency of recurrence of seizures and its association with maternal complications were determined. chi² test for association was used at a 5% level of significance. Results: twelve cases presented recurrence of convulsions after magnesium sulfate (10%) and all received a repeated dose. In four of them convulsions persisted and they received intravenous diazepam. After diazepam, one patient still had seizures, with unsuccessful administration of phenytoin and therefore barbituric coma was induced (thionembutal). This patient had a CT-scan with evidence of intracerebral hemorrhage. Maternal complications were significantly more frequent in the group with recurrence: coma (16.7% versus 0.95), acidosis (50% versus 2.9%), pulmonary edema (16.7% versus 2.9%), cerebral hemorrhage (16.7% versus 0%) and acute renal failure (16.7% versus 1.9%). Three cases of maternal death occurred in patients with recurrence (25%) versus 2 cases in patients without recurrence (1.9%). Conclusions: rate of recurrence after anticonvulsant therapy with magnesium sulfate is low (10%) but it is associated with increased maternal morbidity and mortality. These cases must be managed in an intensive care unit and submitted to routine CT-scan because cerebral hemorrhage can be the cause of recurrence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(3):159-165
DOI 10.1590/S0100-72032000000300007
Purpose: to determine the frequency of recurrence of seizures after anticonvulsant therapy with magnesium sulfate and to evaluate treatment and maternal prognosis. Patients and Methods: a prospective cohort study was conducted, enrolling all cases of eclampsia managed at IMIP between January/1995 and June/1998. Magnesium sulfate and oxygen therapy were administered routinely and interruption of pregnancy was performed after maternal stabilization. The frequency of recurrence of seizures and its association with maternal complications were determined. chi² test for association was used at a 5% level of significance. Results: twelve cases presented recurrence of convulsions after magnesium sulfate (10%) and all received a repeated dose. In four of them convulsions persisted and they received intravenous diazepam. After diazepam, one patient still had seizures, with unsuccessful administration of phenytoin and therefore barbituric coma was induced (thionembutal). This patient had a CT-scan with evidence of intracerebral hemorrhage. Maternal complications were significantly more frequent in the group with recurrence: coma (16.7% versus 0.95), acidosis (50% versus 2.9%), pulmonary edema (16.7% versus 2.9%), cerebral hemorrhage (16.7% versus 0%) and acute renal failure (16.7% versus 1.9%). Three cases of maternal death occurred in patients with recurrence (25%) versus 2 cases in patients without recurrence (1.9%). Conclusions: rate of recurrence after anticonvulsant therapy with magnesium sulfate is low (10%) but it is associated with increased maternal morbidity and mortality. These cases must be managed in an intensive care unit and submitted to routine CT-scan because cerebral hemorrhage can be the cause of recurrence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(3):159-160
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(3):159-160