You searched for:"Antônio Fernandes Moron"
We found (34) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(8):641-647
DOI 10.1590/S0100-72032004000800008
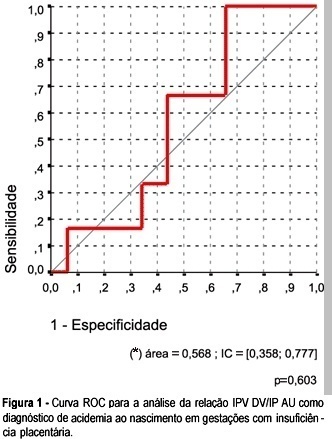
OBJECTIVE: to investigate whether it is possible to predict acidemia at birth in pregnancies with placental insufficiency using venous-arterial indices: pulsatility index for vein (PIV) of the ductus venosus (DV) over PI of the middle cerebral artery (MCA) and PIV of the DV over PI of the umbilical artery, and establish cut-off values for this prediction. PATIENTS AND METHODS: this was a prospective cross-sectional study involving forty-seven patients with placental insufficiency (umbilical artery resistance and pulsatility indices above the 95th percentile for gestational age) who were submitted to Dopplervelocimetry in the last 24 hours before delivery. All pregnancies were singleton, over 26 weeks of age and without structural or chromosome anomalies. Arterial cord blood was obtained for gasometry immediately after birth. Acidemia was defined as umbilical arterial pH < 7.20 in the absence of uterine contractions and pH < 7.15 in the presence of contractions. Metabolic or mixed acidemia at birth were considered pathological. A ROC curve was calculated for the venous-arterial indices: PIV DV/PI umbilical artery (UA) and PIV DV/PI MCA. A cut-off value was established and sensitivity, specificity, accuracy, positive and negative predictive values and positive and negative likelihood ratios were calculated. RESULTS: The DV/UA PI index was not a good predictor of acidemia at birth. The DV/MCA PI index was related to acidemia at birth (area under the curve 0,785, p = 0,004). The cut-off value was: 0,582, sensitivity 66,7%, specificity 77,1 and accuracy 74,5%. CONCLUSION: the PIV DV/PI MCA ratio is adequate for predicting acidemia at birth in pregnancies with placental insufficiency. The cut-off value was: 0,582.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(8):641-647
DOI 10.1590/S0100-72032004000800008
OBJECTIVE: to investigate whether it is possible to predict acidemia at birth in pregnancies with placental insufficiency using venous-arterial indices: pulsatility index for vein (PIV) of the ductus venosus (DV) over PI of the middle cerebral artery (MCA) and PIV of the DV over PI of the umbilical artery, and establish cut-off values for this prediction. PATIENTS AND METHODS: this was a prospective cross-sectional study involving forty-seven patients with placental insufficiency (umbilical artery resistance and pulsatility indices above the 95th percentile for gestational age) who were submitted to Dopplervelocimetry in the last 24 hours before delivery. All pregnancies were singleton, over 26 weeks of age and without structural or chromosome anomalies. Arterial cord blood was obtained for gasometry immediately after birth. Acidemia was defined as umbilical arterial pH < 7.20 in the absence of uterine contractions and pH < 7.15 in the presence of contractions. Metabolic or mixed acidemia at birth were considered pathological. A ROC curve was calculated for the venous-arterial indices: PIV DV/PI umbilical artery (UA) and PIV DV/PI MCA. A cut-off value was established and sensitivity, specificity, accuracy, positive and negative predictive values and positive and negative likelihood ratios were calculated. RESULTS: The DV/UA PI index was not a good predictor of acidemia at birth. The DV/MCA PI index was related to acidemia at birth (area under the curve 0,785, p = 0,004). The cut-off value was: 0,582, sensitivity 66,7%, specificity 77,1 and accuracy 74,5%. CONCLUSION: the PIV DV/PI MCA ratio is adequate for predicting acidemia at birth in pregnancies with placental insufficiency. The cut-off value was: 0,582.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(12):647-652
To determine cervical biometry in pregnant women between 18 and 24 weeks of gestation and the ideal mode of measurement of cervical length in cases of curved and straight cervical morphology.
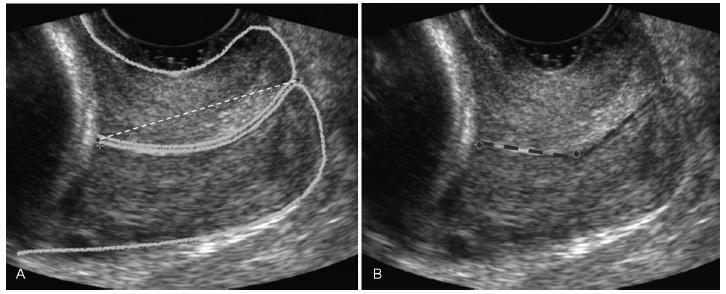
The uterine cervices of 752 low-risk pregnant women were assessed using transvaginal ultrasound in a prospective cross-sectional study. In women with straight uterine cervices, cervical biometry was performed in a continuous manner. In women with curved uterine cervices, the biometry was performed using both the continuous and segmented techniques (in segments joining the cervical os). Polynomial regression models were created to assess the correlation between the cervical length and gestational age. The paired Student t-test was used to comparemeasuring techniques.
The cervical biometry results did not vary significantly with the gestational age and were best represented by linear regression (R2 = 0.0075 with the continuous technique, and R2 = 0.0017 with the segmented technique). Up to the 21st week of gestation, there was a predominance of curved uterine cervix morphology (58.9%), whereas the straight morphology predominated after this gestational age (54.2%). There was a significant difference between the continuous and the segmented measuring methods in all the assessed gestational ages (p < 0.001).
Cervical biometry in pregnant women between 18 and 24 weeks was represented by a linear regression, independently of the measuring mode. The ideal measuring technique was the transvaginal ultrasound performed at a gestational age 21 weeks.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(12):647-652
To determine cervical biometry in pregnant women between 18 and 24 weeks of gestation and the ideal mode of measurement of cervical length in cases of curved and straight cervical morphology.
The uterine cervices of 752 low-risk pregnant women were assessed using transvaginal ultrasound in a prospective cross-sectional study. In women with straight uterine cervices, cervical biometry was performed in a continuous manner. In women with curved uterine cervices, the biometry was performed using both the continuous and segmented techniques (in segments joining the cervical os). Polynomial regression models were created to assess the correlation between the cervical length and gestational age. The paired Student t-test was used to comparemeasuring techniques.
The cervical biometry results did not vary significantly with the gestational age and were best represented by linear regression (R2 = 0.0075 with the continuous technique, and R2 = 0.0017 with the segmented technique). Up to the 21st week of gestation, there was a predominance of curved uterine cervix morphology (58.9%), whereas the straight morphology predominated after this gestational age (54.2%). There was a significant difference between the continuous and the segmented measuring methods in all the assessed gestational ages (p < 0.001).
Cervical biometry in pregnant women between 18 and 24 weeks was represented by a linear regression, independently of the measuring mode. The ideal measuring technique was the transvaginal ultrasound performed at a gestational age 21 weeks.