You searched for:"Marcelo Zugaib"
We found (76) results for your search.Summary
Rev Bras Ginecol Obstet. 2011;33(10):280-285
DOI 10.1590/S0100-72032011001000002
PURPOSE: To analyze the results of assessment of fetal well-being in pregnancies complicated by moderate or severe maternal thrombocytopenia. METHODS: Data from April 2001 to July 2011 of 96 women with a diagnosis of thrombocytopenia in pregnancy were retrospectively analyzed. We analyzed the following tests performed during the antepartum period for fetal assessment: cardiotocography, fetal biophysical profile, amniotic fluid index and umbilical artery Doppler velocimetry. RESULTS: A total of 96 pregnancies with the following diagnoses were analyzed: gestational thrombocytopenia (n=37, 38.5%) hypersplenism (n=32, 33.3%), immune thrombocytopenic purpura (ITP, n=14, 14.6%), secondary immune thrombocytopenia (n=6, 6.3%), bone marrow aplasia (n=3, 3.1%), and others (n=4, 4.1%). Cardiotocography showed normal results in 94% of cases, a fetal biophysical profile with an index of 8 or 10 in 96.9% and an amniotic fluid index >5.0 cm in 89.6%. Doppler umbilical artery velocimetry showed normal results in 96.9% of cases. In the analysis of the major groups of thrombocytopenia, the diagnosis of oligohydramnios was found to be significantly more frequent in the group with ITP (28.6%) compared to the other groups (gestational thrombocytopenia: 5.4% and hypersplenism: 9.4%, p=0.04). CONCLUSIONS: This study indicates that in pregnancies complicated by moderate or severe maternal thrombocytopenia, even though the fetal well-being remains preserved in most cases, fetal surveillance is important in pregnant women with ITP, with emphasis on amniotic fluid volume evaluation due to its association with oligohydramnios.
Summary
Rev Bras Ginecol Obstet. 2011;33(10):280-285
DOI 10.1590/S0100-72032011001000002
PURPOSE: To analyze the results of assessment of fetal well-being in pregnancies complicated by moderate or severe maternal thrombocytopenia. METHODS: Data from April 2001 to July 2011 of 96 women with a diagnosis of thrombocytopenia in pregnancy were retrospectively analyzed. We analyzed the following tests performed during the antepartum period for fetal assessment: cardiotocography, fetal biophysical profile, amniotic fluid index and umbilical artery Doppler velocimetry. RESULTS: A total of 96 pregnancies with the following diagnoses were analyzed: gestational thrombocytopenia (n=37, 38.5%) hypersplenism (n=32, 33.3%), immune thrombocytopenic purpura (ITP, n=14, 14.6%), secondary immune thrombocytopenia (n=6, 6.3%), bone marrow aplasia (n=3, 3.1%), and others (n=4, 4.1%). Cardiotocography showed normal results in 94% of cases, a fetal biophysical profile with an index of 8 or 10 in 96.9% and an amniotic fluid index >5.0 cm in 89.6%. Doppler umbilical artery velocimetry showed normal results in 96.9% of cases. In the analysis of the major groups of thrombocytopenia, the diagnosis of oligohydramnios was found to be significantly more frequent in the group with ITP (28.6%) compared to the other groups (gestational thrombocytopenia: 5.4% and hypersplenism: 9.4%, p=0.04). CONCLUSIONS: This study indicates that in pregnancies complicated by moderate or severe maternal thrombocytopenia, even though the fetal well-being remains preserved in most cases, fetal surveillance is important in pregnant women with ITP, with emphasis on amniotic fluid volume evaluation due to its association with oligohydramnios.
Summary
Rev Bras Ginecol Obstet. 2002;24(1):29-36
DOI 10.1590/S0100-72032002000100005
Purpose: to study computerized cardiotocography performed in high-risk pregnancies, analyze the results, and correlate the criteria to perinatal results. Patients and Methods: two hundred and thirty-three high-risk pregnancies were studied prospectively, performing a total of 485 computerized cardiotocographies. The exclusion criteria included fetal anomalies and signal loss over 20% (proportion of 3.75-millisecond periods in which there were no valid pulse intervals). The perinatal results of 71 pregnancies were correlated to the last cardiotocography, performed at least seven days before birth, excluding patients with absent or reversed end diastolic velocities in the umbilical arteries. Results: thirty-three examinations with signal loss over 20% were excluded. The normal criteria were met in 404 (83.3%), and 62.1% examinations met the criteria within 20 minutes and 79% within 30 minutes. The abnormal computerized cardiotocography was related significantly (p<0.05) to adverse perinatal results, such as: preterm delivery, first minute Apgar score less than 7 (33%), neonatal intensive care admission (55.5%) and intubation of newborn at delivery (44.4%). Conclusions: computerized cardiotocography in high-risk pregnancies met the normal criteria in most of the cases, with the examination performed for 30 minutes. The cases that did not meet the criteria correlated significantly to adverse perinatal results.
Summary
Rev Bras Ginecol Obstet. 2002;24(1):29-36
DOI 10.1590/S0100-72032002000100005
Purpose: to study computerized cardiotocography performed in high-risk pregnancies, analyze the results, and correlate the criteria to perinatal results. Patients and Methods: two hundred and thirty-three high-risk pregnancies were studied prospectively, performing a total of 485 computerized cardiotocographies. The exclusion criteria included fetal anomalies and signal loss over 20% (proportion of 3.75-millisecond periods in which there were no valid pulse intervals). The perinatal results of 71 pregnancies were correlated to the last cardiotocography, performed at least seven days before birth, excluding patients with absent or reversed end diastolic velocities in the umbilical arteries. Results: thirty-three examinations with signal loss over 20% were excluded. The normal criteria were met in 404 (83.3%), and 62.1% examinations met the criteria within 20 minutes and 79% within 30 minutes. The abnormal computerized cardiotocography was related significantly (p<0.05) to adverse perinatal results, such as: preterm delivery, first minute Apgar score less than 7 (33%), neonatal intensive care admission (55.5%) and intubation of newborn at delivery (44.4%). Conclusions: computerized cardiotocography in high-risk pregnancies met the normal criteria in most of the cases, with the examination performed for 30 minutes. The cases that did not meet the criteria correlated significantly to adverse perinatal results.
Summary
Rev Bras Ginecol Obstet. 2002;24(5):301-306
DOI 10.1590/S0100-72032002000500003
Purpose: to compare the outcome of pregnancies with and without threatened abortion presenting alive embryo/fetus between 6 and 13 weeks at sonographic evaluation. Method: this was a retrospective case-control study, carried out from February 1998 to December 1999. Criteria for inclusion were: topic and single pregnancy; embryo/fetus cardiac activity present in the ultrasound scan; gestational age between 6 weeks and 13 weeks and 6 days, absence of fetal anomalies, absence of attempt of abortion by drugs or manipulation, absence of maternal disease, known pregnancy result. A total of 1531 pregnancies were examined, of which 258 with threatened abortion (case group) and 1273 without threatened abortion (control group). The two groups were compared regarding outcome such as: abortion, stillbirth, prematurity and intrauterine growth restriction. Results: the percentage of abortion (11,7%) and prematurity (17,8%) were higher in the group with threatened abortion (p<0.001 and p=0.026, respectively). The frequency of stillbirth and intrauterine growth restriction did not differ significantly between the groups.Conclusion: threatened abortion with alive embryo/fetus in 6- to 13- week gestation presented a higher abortion risk and subsequent prematurity.
Summary
Rev Bras Ginecol Obstet. 2002;24(5):301-306
DOI 10.1590/S0100-72032002000500003
Purpose: to compare the outcome of pregnancies with and without threatened abortion presenting alive embryo/fetus between 6 and 13 weeks at sonographic evaluation. Method: this was a retrospective case-control study, carried out from February 1998 to December 1999. Criteria for inclusion were: topic and single pregnancy; embryo/fetus cardiac activity present in the ultrasound scan; gestational age between 6 weeks and 13 weeks and 6 days, absence of fetal anomalies, absence of attempt of abortion by drugs or manipulation, absence of maternal disease, known pregnancy result. A total of 1531 pregnancies were examined, of which 258 with threatened abortion (case group) and 1273 without threatened abortion (control group). The two groups were compared regarding outcome such as: abortion, stillbirth, prematurity and intrauterine growth restriction. Results: the percentage of abortion (11,7%) and prematurity (17,8%) were higher in the group with threatened abortion (p<0.001 and p=0.026, respectively). The frequency of stillbirth and intrauterine growth restriction did not differ significantly between the groups.Conclusion: threatened abortion with alive embryo/fetus in 6- to 13- week gestation presented a higher abortion risk and subsequent prematurity.
Summary
Rev Bras Ginecol Obstet. 2001;23(1):31-37
DOI 10.1590/S0100-72032001000100005
Purpose: to evaluate the prognosis of fetal omphalocele after prenatal diagnosis. Methods: fifty-one cases with prenatal diagnosis of fetal omphalocele were divided into three groups: group 1, isolated omphalocele; group 2, omphalocele associated with structural abnormalities and normal karyotype; group 3, omphalocele with abnormal karyotype. The data were analyzed for overall survival rate and postsurgery survival, considering associated malformations, gestational age at delivery, birth weight and size of omphalocele. Results: group 1 corresponded to 21% (n = 11), group 2, 55% (n = 28) and group 3,24% (n = 12). All of Group 3 died, and trisomy 18 was the most frequent chromosomal abnormality. The survival rate was 80% for group 1 and 25% for group 2. Sixteen cases underwent surgery (10 isolated and 6 associated), 81% survived (8 isolated and 5 associated). The median birth weight was 3,140 g and 2,000 g for survivals and non-survivals after surgery, respectively (p = 0.148), and the corresponding gestational age at delivery was 37 and 36 weeks (p = 0.836). The ratio of omphalocele/abdominal circumference decreased with gestation, 0.88 between 25-29 weeks and 0.65 between 30-35 weeks (p = 0.043). The size of omphalocele was not significantly different between the 3 groups (p = 0.988), and it was not associated to postsurgery prognosis (p = 0.553). Conclusion: the overall and postsurgery survival rates were 25 and 81%, respectively. Associated malformations were the main prognostic factor in prenatally diagnosed omphaloceles, since they are associated with prematurity and low birth weight.
Summary
Rev Bras Ginecol Obstet. 2001;23(1):31-37
DOI 10.1590/S0100-72032001000100005
Purpose: to evaluate the prognosis of fetal omphalocele after prenatal diagnosis. Methods: fifty-one cases with prenatal diagnosis of fetal omphalocele were divided into three groups: group 1, isolated omphalocele; group 2, omphalocele associated with structural abnormalities and normal karyotype; group 3, omphalocele with abnormal karyotype. The data were analyzed for overall survival rate and postsurgery survival, considering associated malformations, gestational age at delivery, birth weight and size of omphalocele. Results: group 1 corresponded to 21% (n = 11), group 2, 55% (n = 28) and group 3,24% (n = 12). All of Group 3 died, and trisomy 18 was the most frequent chromosomal abnormality. The survival rate was 80% for group 1 and 25% for group 2. Sixteen cases underwent surgery (10 isolated and 6 associated), 81% survived (8 isolated and 5 associated). The median birth weight was 3,140 g and 2,000 g for survivals and non-survivals after surgery, respectively (p = 0.148), and the corresponding gestational age at delivery was 37 and 36 weeks (p = 0.836). The ratio of omphalocele/abdominal circumference decreased with gestation, 0.88 between 25-29 weeks and 0.65 between 30-35 weeks (p = 0.043). The size of omphalocele was not significantly different between the 3 groups (p = 0.988), and it was not associated to postsurgery prognosis (p = 0.553). Conclusion: the overall and postsurgery survival rates were 25 and 81%, respectively. Associated malformations were the main prognostic factor in prenatally diagnosed omphaloceles, since they are associated with prematurity and low birth weight.
Summary
Rev Bras Ginecol Obstet. 2005;27(6):310-315
DOI 10.1590/S0100-72032005000600004
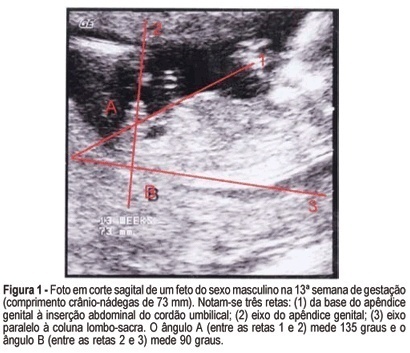
PURPOSE: to evaluate the accuracy of fetal gender prediction at 11 to 13 weeks and 6 days by measuring the anterior and posterior genital tubercle angles. MESTHODS: the anterior and posterior genital tubercle angles were measured in a midsagittal plane in 455 fetuses from 11 to 13 weeks and 6 days. The probability of a correct fetal sex prediction (confirmed after birth) was categorized in accordance with the angle measurements, gestational age and crump-rump length. The optimal accuracy cutoffs were derived from a ROC-plot. The interobserver variability was evaluated by a Bland-Altman plot. RESULTS: the correct fetal sex prediction rate increased with gestational age and crump-rump length. Using a 42-degree anterior angle as a cutoff, a correct fetal sex prediction occurred in 72% of the fetuses from 11 to 11 weeks and 6 days, 86% from 12 to 12 weeks and 6 days and 88% from 13 to 13 weeks and 6 days. Using a 24-degree posterior angle as a cutoff, a correct fetal gender prediction occurred in 70, 87 and 87%, respectively. The interobserver variability evaluation revealed a mean difference between paired measurements of 15.7 and 9 degrees for the posterior and anterior angles, respectively. CONCLUSION: the measurement of the genital tubercle angles showed a high accuracy in correctly predicting the fetal sex from the 12th week of gestation on. However, accuracy was still not high enough for clinical use in pregnancies at risk of serious X-linked diseases.
Summary
Rev Bras Ginecol Obstet. 2005;27(6):310-315
DOI 10.1590/S0100-72032005000600004
PURPOSE: to evaluate the accuracy of fetal gender prediction at 11 to 13 weeks and 6 days by measuring the anterior and posterior genital tubercle angles. MESTHODS: the anterior and posterior genital tubercle angles were measured in a midsagittal plane in 455 fetuses from 11 to 13 weeks and 6 days. The probability of a correct fetal sex prediction (confirmed after birth) was categorized in accordance with the angle measurements, gestational age and crump-rump length. The optimal accuracy cutoffs were derived from a ROC-plot. The interobserver variability was evaluated by a Bland-Altman plot. RESULTS: the correct fetal sex prediction rate increased with gestational age and crump-rump length. Using a 42-degree anterior angle as a cutoff, a correct fetal sex prediction occurred in 72% of the fetuses from 11 to 11 weeks and 6 days, 86% from 12 to 12 weeks and 6 days and 88% from 13 to 13 weeks and 6 days. Using a 24-degree posterior angle as a cutoff, a correct fetal gender prediction occurred in 70, 87 and 87%, respectively. The interobserver variability evaluation revealed a mean difference between paired measurements of 15.7 and 9 degrees for the posterior and anterior angles, respectively. CONCLUSION: the measurement of the genital tubercle angles showed a high accuracy in correctly predicting the fetal sex from the 12th week of gestation on. However, accuracy was still not high enough for clinical use in pregnancies at risk of serious X-linked diseases.
Summary
Rev Bras Ginecol Obstet. 2006;28(6):324-330
DOI 10.1590/S0100-72032006000600002
PURPOSE: to compare the maternal factors, clinical aspects and perinatal results in placental abruption during two periods. METHODS: retrospective analysis of placental abruption cases that occurred from January 1, 1994 through December 31, 1997 (period 94-97), and from April 4, 2001 through March 3, 2005 (period 01-05), in singleton delivery with birthweight higher than 500 g and after 20 weeks of gestation. The following factors were analyzed: maternal age, previous obstetric history, prenatal care, premature rupture of membranes, obstetric and/or clinical intercurrent events, vaginal bleeding, uterine tonus, fetal anomaly, mode of delivery, hemoamnion and maternal complication (hysterectomy, uterine atony, disseminated intravascular coagulation, acute renal failure, and maternal death), and the perinatal results. RESULTS: the rate of placental abruption was 0.78% (60 cases) in the period 94-97 (n=7692 deliveries), and 0.59% (51 cases) in the period 01-05 (n=8644 deliveries), without significant difference. A significant difference was observed between the periods 94-97 and 01-05 regarding mean number of previous gestations (3.5±2.4 and 2.6±1.8, p=0.04), patients without prenatal care (13.3 and 2.0%, p=0.03) and maternal intercurrences (38.3 and 64.7%, p=0.01). No significant difference was observed related to vaginal bleeding, tonus abnormalities and perinatal results, between the periods, but a higher proportion of hemoamnion in 94-97 was found when compared to 01-05 (28.3 and 11.8%, p=0.03). CONCLUSIONS: in spite of obstetrical advances, maternal complications and perinatal results were similar in the analyzed periods. The severity and the unexpected results emphasize the importance of prevention and adequate control of associated factors, when this pathology is approached.
Summary
Rev Bras Ginecol Obstet. 2006;28(6):324-330
DOI 10.1590/S0100-72032006000600002
PURPOSE: to compare the maternal factors, clinical aspects and perinatal results in placental abruption during two periods. METHODS: retrospective analysis of placental abruption cases that occurred from January 1, 1994 through December 31, 1997 (period 94-97), and from April 4, 2001 through March 3, 2005 (period 01-05), in singleton delivery with birthweight higher than 500 g and after 20 weeks of gestation. The following factors were analyzed: maternal age, previous obstetric history, prenatal care, premature rupture of membranes, obstetric and/or clinical intercurrent events, vaginal bleeding, uterine tonus, fetal anomaly, mode of delivery, hemoamnion and maternal complication (hysterectomy, uterine atony, disseminated intravascular coagulation, acute renal failure, and maternal death), and the perinatal results. RESULTS: the rate of placental abruption was 0.78% (60 cases) in the period 94-97 (n=7692 deliveries), and 0.59% (51 cases) in the period 01-05 (n=8644 deliveries), without significant difference. A significant difference was observed between the periods 94-97 and 01-05 regarding mean number of previous gestations (3.5±2.4 and 2.6±1.8, p=0.04), patients without prenatal care (13.3 and 2.0%, p=0.03) and maternal intercurrences (38.3 and 64.7%, p=0.01). No significant difference was observed related to vaginal bleeding, tonus abnormalities and perinatal results, between the periods, but a higher proportion of hemoamnion in 94-97 was found when compared to 01-05 (28.3 and 11.8%, p=0.03). CONCLUSIONS: in spite of obstetrical advances, maternal complications and perinatal results were similar in the analyzed periods. The severity and the unexpected results emphasize the importance of prevention and adequate control of associated factors, when this pathology is approached.
Summary
Rev Bras Ginecol Obstet. 1998;20(6):335-341
DOI 10.1590/S0100-72031998000600006
Objective: to analyze maternal and fetal folate status in cases of neural tube defects (NTD). Methods: a case-control study was designed with 14 cases of fetuses with neural tube defects (study group) and 14 cases of fetuses with other unrelated malformations (control group) gestational age matched, in low-risk pregnant women. Both total and methylated folic acid levels in fetal and maternal compartments using serum and tissular (red blood cells) concentrations and also average corpuscular volume, hematocrit and hemoglobin levels were determined. Fetal and maternal samples were obtained immediately before termination of pregnancy. Results in both groups were compared using a gestational age paired t-test. Results: there were no statistically significant differences in fetal folate levels and fetal hematologic parameters between both groups However, both total (239.9 ng/mL in NTD against 399.1 ng/mL in control group, p=0.01) and methylated (201.9 ng/mL in NTD against 314.0 ng/mL in control group, p=0.02) maternal red blood cells folate levels were significantly lower in the neural tube defect group. Maternal serum folate levels were similar in study and control groups. Conclusion: this study showed that maternal red blood cell folate but not serum folate was significantly reduced in mothers of fetuses with neural tube defects.
Summary
Rev Bras Ginecol Obstet. 1998;20(6):335-341
DOI 10.1590/S0100-72031998000600006
Objective: to analyze maternal and fetal folate status in cases of neural tube defects (NTD). Methods: a case-control study was designed with 14 cases of fetuses with neural tube defects (study group) and 14 cases of fetuses with other unrelated malformations (control group) gestational age matched, in low-risk pregnant women. Both total and methylated folic acid levels in fetal and maternal compartments using serum and tissular (red blood cells) concentrations and also average corpuscular volume, hematocrit and hemoglobin levels were determined. Fetal and maternal samples were obtained immediately before termination of pregnancy. Results in both groups were compared using a gestational age paired t-test. Results: there were no statistically significant differences in fetal folate levels and fetal hematologic parameters between both groups However, both total (239.9 ng/mL in NTD against 399.1 ng/mL in control group, p=0.01) and methylated (201.9 ng/mL in NTD against 314.0 ng/mL in control group, p=0.02) maternal red blood cells folate levels were significantly lower in the neural tube defect group. Maternal serum folate levels were similar in study and control groups. Conclusion: this study showed that maternal red blood cell folate but not serum folate was significantly reduced in mothers of fetuses with neural tube defects.