You searched for:"Geraldo Duarte"
We found (54) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(5):317-321
DOI 10.1590/S0100-72032003000500003
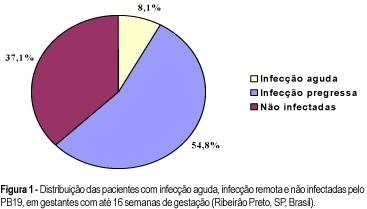
PURPOSE: to evaluate the rate of seropositivity for parvovirus B19 (PB19) among pregnant women and the rate of seroconversion against this infection during pregnancy. METHODS: prospective study carried out in the Hospital of the Medical School of Ribeirão Preto, University of São Paulo. In the first stage of the present study, we evaluated 245 pregnant women with gestational age less than 16 weeks to determine the seroprevalence of PB19 infection by ELISA. According to the serological results we determined if the PB19 infection was an acute infection (IgM positive and IgG negative or positive), or a former infection (IgM negative and IgG positive). In the second stage of this study, 73 previously seronegative pregnant women were tested again when they came to the hospital for delivery (IgM and IgG), to detect the seroconversion rate during pregnancy. RESULTS: the seroprevalence of the PB19 infection until 16 weeks of gestation was 62.9% (95% IC: 56.8-68.9), divided into acute infection (8.1%), or former infection (54.8%). Of the 73 patients, seronegative in the first stage of this investigation, seven (9.6%) showed seroconversion during pregnancy (95% IC: 2.8-16.3), two (2.7%) showed acute serological infection and five (6.9%) presented markers of past infection. The final seroprevalence of PB19 infection during pregnancy was 72.5%. CONCLUSIONS: considering that only the acute PB19 infection is associated with risk for vertical transmission, the high seroprevalence of this infection observed in this study would be protecting these fetuses against this form of infection. Despite the relatively high rate of seroconversion against PB19 infection during the pregnancy period, we did not observe any symptomatic neonate in this group.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(5):317-321
DOI 10.1590/S0100-72032003000500003
PURPOSE: to evaluate the rate of seropositivity for parvovirus B19 (PB19) among pregnant women and the rate of seroconversion against this infection during pregnancy. METHODS: prospective study carried out in the Hospital of the Medical School of Ribeirão Preto, University of São Paulo. In the first stage of the present study, we evaluated 245 pregnant women with gestational age less than 16 weeks to determine the seroprevalence of PB19 infection by ELISA. According to the serological results we determined if the PB19 infection was an acute infection (IgM positive and IgG negative or positive), or a former infection (IgM negative and IgG positive). In the second stage of this study, 73 previously seronegative pregnant women were tested again when they came to the hospital for delivery (IgM and IgG), to detect the seroconversion rate during pregnancy. RESULTS: the seroprevalence of the PB19 infection until 16 weeks of gestation was 62.9% (95% IC: 56.8-68.9), divided into acute infection (8.1%), or former infection (54.8%). Of the 73 patients, seronegative in the first stage of this investigation, seven (9.6%) showed seroconversion during pregnancy (95% IC: 2.8-16.3), two (2.7%) showed acute serological infection and five (6.9%) presented markers of past infection. The final seroprevalence of PB19 infection during pregnancy was 72.5%. CONCLUSIONS: considering that only the acute PB19 infection is associated with risk for vertical transmission, the high seroprevalence of this infection observed in this study would be protecting these fetuses against this form of infection. Despite the relatively high rate of seroconversion against PB19 infection during the pregnancy period, we did not observe any symptomatic neonate in this group.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):369-375
DOI 10.1590/S0100-72032004000500005
OBJECTIVE: to assess the action of antiretroviral drugs on glycid metabolism and on the pancreas of pregnant Wistar rats. METHODS: adult pregnant Wistar rats weighing 200-230g were used. Azidothymidine, lamivudine and nelfinavir were administered to the animals at doses 10 times higher than those administered to pregnant women. The animals were divided into seven groups of 10 animals, including a control group. The animals were sacrificed on the 21st day of pregnancy and glycemia, insulinemia, glucagonemia, free fatty acids (FFA) and hepatic glycogen were measured. Direct counts of the number of immunohistochemically labeled insulin- and glucagon-producing cells were used to determine pancreatic damage. Data were analyzed statistically by the Student's t-test comparing each treated group with the control group. RESULTS: increased serum glucagon (control group: 88.2 pg/ml; treated groups: 99.7-120.7 pg/ml) and reduced insulin (control group: 6.2 muIU/ml; treated groups: 2.1-2.7 muIU/ml) were observed in all groups treated with antiretroviral drugs after 21 days of pregnancy. There was no significant difference between the experimental groups and the control in glycemia, plasma FFA or hepatic glycogen. Also, there was no significant difference in number of insulin- and glucagon-producing cells between the treated groups and the control. CONCLUSION: treatment of noninfected rats with antiretroviral drugs during pregnancy altered maternal glycid metabolism causing insulin decrease and glucagon elevation, with normal glycemia and unchanged number of pancreatic cells.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):369-375
DOI 10.1590/S0100-72032004000500005
OBJECTIVE: to assess the action of antiretroviral drugs on glycid metabolism and on the pancreas of pregnant Wistar rats. METHODS: adult pregnant Wistar rats weighing 200-230g were used. Azidothymidine, lamivudine and nelfinavir were administered to the animals at doses 10 times higher than those administered to pregnant women. The animals were divided into seven groups of 10 animals, including a control group. The animals were sacrificed on the 21st day of pregnancy and glycemia, insulinemia, glucagonemia, free fatty acids (FFA) and hepatic glycogen were measured. Direct counts of the number of immunohistochemically labeled insulin- and glucagon-producing cells were used to determine pancreatic damage. Data were analyzed statistically by the Student's t-test comparing each treated group with the control group. RESULTS: increased serum glucagon (control group: 88.2 pg/ml; treated groups: 99.7-120.7 pg/ml) and reduced insulin (control group: 6.2 muIU/ml; treated groups: 2.1-2.7 muIU/ml) were observed in all groups treated with antiretroviral drugs after 21 days of pregnancy. There was no significant difference between the experimental groups and the control in glycemia, plasma FFA or hepatic glycogen. Also, there was no significant difference in number of insulin- and glucagon-producing cells between the treated groups and the control. CONCLUSION: treatment of noninfected rats with antiretroviral drugs during pregnancy altered maternal glycid metabolism causing insulin decrease and glucagon elevation, with normal glycemia and unchanged number of pancreatic cells.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):37-43
DOI 10.1590/S0100-72032005000100008
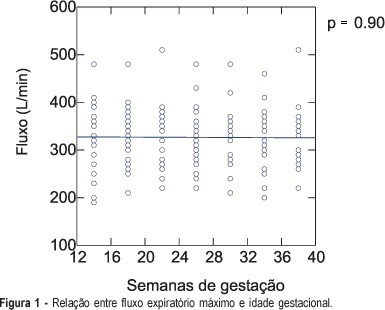
PURPOSE: to investigate the normal peak expiratory flow values in healthy pregnant women employing a portable expiratory apparatus (Mini-Wright Peak Flow Meter), and to relate the obtained measurements to each patient's height, body mass index (BMI) and age, along gestation. METHODS: a longitudinal prospective study including 26 pregnant women followed up from the first trimester to the 36th week of gestation and examined every four weeks. On the occasion of seven visits, the pregnant women performed forced exhaling into a portable expiratory apparatus three times, with the highest value being considered the peak expiratory flow. All measurements were made under the same investigator's supervision in order to reduce the margin of error. Pearson coefficient was used to calculate the correlation between flow and BMI, between flow and patient's height, and between flow and patient's age. RESULTS: the variation in flow values during pregnancy can be determined by flow = 328.32 -0.07 x week, with a Pearson coefficient equal to zero. To determine whether there was a difference in the correlation coefficients between BMI and flow, we compared the lowest coefficient (0.47 for week 30, flow = 123.49 + 7.64 x BMI) with the highest coefficient (0.59 for week 34, flow = 87.77 + 9.05 x BMI) of each studied time interval and obtained a value of 0.22, indicating a good correlation between the flow and BMI variables. There was a positive correlation between height and flow (Pearson = 0.61), with flow = -477.47 + 497.38 x height. The correlation coefficient between flow and age was 0.24, with the equation obtained in this case being non-linear. CONCLUSIONS: peak expiratory flow values did not change along gestation. Higher flows were observed in taller women. Pregnant women with a higher BMI before gestation presented higher flows. There was no correlation between flow and maternal age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):37-43
DOI 10.1590/S0100-72032005000100008
PURPOSE: to investigate the normal peak expiratory flow values in healthy pregnant women employing a portable expiratory apparatus (Mini-Wright Peak Flow Meter), and to relate the obtained measurements to each patient's height, body mass index (BMI) and age, along gestation. METHODS: a longitudinal prospective study including 26 pregnant women followed up from the first trimester to the 36th week of gestation and examined every four weeks. On the occasion of seven visits, the pregnant women performed forced exhaling into a portable expiratory apparatus three times, with the highest value being considered the peak expiratory flow. All measurements were made under the same investigator's supervision in order to reduce the margin of error. Pearson coefficient was used to calculate the correlation between flow and BMI, between flow and patient's height, and between flow and patient's age. RESULTS: the variation in flow values during pregnancy can be determined by flow = 328.32 -0.07 x week, with a Pearson coefficient equal to zero. To determine whether there was a difference in the correlation coefficients between BMI and flow, we compared the lowest coefficient (0.47 for week 30, flow = 123.49 + 7.64 x BMI) with the highest coefficient (0.59 for week 34, flow = 87.77 + 9.05 x BMI) of each studied time interval and obtained a value of 0.22, indicating a good correlation between the flow and BMI variables. There was a positive correlation between height and flow (Pearson = 0.61), with flow = -477.47 + 497.38 x height. The correlation coefficient between flow and age was 0.24, with the equation obtained in this case being non-linear. CONCLUSIONS: peak expiratory flow values did not change along gestation. Higher flows were observed in taller women. Pregnant women with a higher BMI before gestation presented higher flows. There was no correlation between flow and maternal age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):387-392
DOI 10.1590/S0100-72032005000700004
PURPOSE: to assess peak systolic velocity (PSV) and the resistance index (RI) in the middle cerebral artery (MCA), suprarenal aorta (SRA) and infrarenal aorta (IRA) of the fetus and in the umbilical artery (UA) between the 22nd and 38th week of gestation. METHODS: a prospective study which evaluated the parameters of 33 normal fetuses in the 22nd, 26th, 30th, and 38th week of gestation. Pregnant women with a singleton fetus with no diseases or complications and who agreed to participate were included in the study. Exclusion criteria were fetal malformations, discontinuation of prenatal care visits and mothers who smoked, used alcohol or illicit drugs. Ultrasound examinations were performed by a single observer. For the acquisition of the Doppler velocimetry tracing in the MCA, SRA, IRA and UA, the sample volume was 1 to 2 mm, placed in the center of the arteries. The insonation angle was 5º to 19º in the MCA, below 45º in the SRA and IRA, and less than 60º in the UA. We used a wall filter of 50-100 Hz. The parameters were calculated automatically with the frozen image, three measurements being made. The final result was obtained by the arithmetic mean of the three values. Data were analyzed by analysis of variance (ANOVA), post hoc Bonferroni test, Pearson's correlation, and regression analysis. The level of significance was set at p<0.05 in all analyses. RESULTS: PSV increased from 26.3 to 57.7 cm/s in the MCA between the 22nd and the 38th week of gestation (p<0.05). In the SRA and in the IRA, PSV increased between the 22nd and 34th week of gestation, from 74.6 and 59.0 cm/s to 106.0 and 86.6 cm/s, respectively (p<0.05). In the UA, PSV increased between the 22nd and the 34th week of gestation, but decreased from 55.5 to 46.2 cm/s between the 34th and the 38th week of gestation. In the MCA, the RI was lower in the 22nd (0.81) and 38th week of gestation (0.75) and higher (0.85) in the 26th week (p<0.05). In the SRA, the RI values were stable in all weeks and in the IRA they were stable in most weeks (p>0.05). In the UA, RI decreased from 0.69 to 0.56 between the 22nd and 38th week of gestation (p<0.05). CONCLUSION: in normal fetuses, in the second half of gestation PSV increased in the MCA, SRA and IRA, decreasing in the UA between the 34th and 38th week of gestation. RI was lower in the 22nd and 38th weeks of gestation in the MCA, decreased between the 22nd and the 38th week in the UA, and was constant in most of the gestational weeks in the SRA and IRA.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):387-392
DOI 10.1590/S0100-72032005000700004
PURPOSE: to assess peak systolic velocity (PSV) and the resistance index (RI) in the middle cerebral artery (MCA), suprarenal aorta (SRA) and infrarenal aorta (IRA) of the fetus and in the umbilical artery (UA) between the 22nd and 38th week of gestation. METHODS: a prospective study which evaluated the parameters of 33 normal fetuses in the 22nd, 26th, 30th, and 38th week of gestation. Pregnant women with a singleton fetus with no diseases or complications and who agreed to participate were included in the study. Exclusion criteria were fetal malformations, discontinuation of prenatal care visits and mothers who smoked, used alcohol or illicit drugs. Ultrasound examinations were performed by a single observer. For the acquisition of the Doppler velocimetry tracing in the MCA, SRA, IRA and UA, the sample volume was 1 to 2 mm, placed in the center of the arteries. The insonation angle was 5º to 19º in the MCA, below 45º in the SRA and IRA, and less than 60º in the UA. We used a wall filter of 50-100 Hz. The parameters were calculated automatically with the frozen image, three measurements being made. The final result was obtained by the arithmetic mean of the three values. Data were analyzed by analysis of variance (ANOVA), post hoc Bonferroni test, Pearson's correlation, and regression analysis. The level of significance was set at p<0.05 in all analyses. RESULTS: PSV increased from 26.3 to 57.7 cm/s in the MCA between the 22nd and the 38th week of gestation (p<0.05). In the SRA and in the IRA, PSV increased between the 22nd and 34th week of gestation, from 74.6 and 59.0 cm/s to 106.0 and 86.6 cm/s, respectively (p<0.05). In the UA, PSV increased between the 22nd and the 34th week of gestation, but decreased from 55.5 to 46.2 cm/s between the 34th and the 38th week of gestation. In the MCA, the RI was lower in the 22nd (0.81) and 38th week of gestation (0.75) and higher (0.85) in the 26th week (p<0.05). In the SRA, the RI values were stable in all weeks and in the IRA they were stable in most weeks (p>0.05). In the UA, RI decreased from 0.69 to 0.56 between the 22nd and 38th week of gestation (p<0.05). CONCLUSION: in normal fetuses, in the second half of gestation PSV increased in the MCA, SRA and IRA, decreasing in the UA between the 34th and 38th week of gestation. RI was lower in the 22nd and 38th weeks of gestation in the MCA, decreased between the 22nd and the 38th week in the UA, and was constant in most of the gestational weeks in the SRA and IRA.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(9):387-392
DOI 10.1590/SO100-720320140005053
To evaluate the cases of uterine rupture and dehiscence of the uterine scar at a low-risk maternity and to point out possibilities for an improved approach to these complications.
A descriptive study was conducted at a 30-bed low-risk maternity hospital that provides care to users of the public health system. The investigation was carried out by searching for cases in the delivery room registry book and later reading the medical records in order to obtain the data. The information was inserted on a form previously elaborated for this study. Cases of uterine rupure and dehiscence of the uterine scar diagnosed from 1998 to 2012 were included, with the determination of incidence, aspects related to risk factors and diagnosis, association with the use of misoprostol and oxytocin, and the outcomes observed.
A total of 39,206 deliveries were performed in this maternity during the study period, with 12 cases of uterine rupture and 16 cases of dehiscence of uterine scar being observed. The most relevant results were a high perinatal mortality associated with uterine rupture and the unsuccessful diagnosis of this complications. It was not possible to demonstrate an association with the use of misoprostol or oxytocin.
The adverse outcomes of uterine rupture could be minimized if efforts were directed at improving the diagnostic performance of the assisting teams.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(9):387-392
DOI 10.1590/SO100-720320140005053
To evaluate the cases of uterine rupture and dehiscence of the uterine scar at a low-risk maternity and to point out possibilities for an improved approach to these complications.
A descriptive study was conducted at a 30-bed low-risk maternity hospital that provides care to users of the public health system. The investigation was carried out by searching for cases in the delivery room registry book and later reading the medical records in order to obtain the data. The information was inserted on a form previously elaborated for this study. Cases of uterine rupure and dehiscence of the uterine scar diagnosed from 1998 to 2012 were included, with the determination of incidence, aspects related to risk factors and diagnosis, association with the use of misoprostol and oxytocin, and the outcomes observed.
A total of 39,206 deliveries were performed in this maternity during the study period, with 12 cases of uterine rupture and 16 cases of dehiscence of uterine scar being observed. The most relevant results were a high perinatal mortality associated with uterine rupture and the unsuccessful diagnosis of this complications. It was not possible to demonstrate an association with the use of misoprostol or oxytocin.
The adverse outcomes of uterine rupture could be minimized if efforts were directed at improving the diagnostic performance of the assisting teams.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):442-449
DOI 10.1590/S0100-72032005000800002
PURPOSE: to establish the frequency of acute toxoplasmosis in pregnant women, vertical transmission rate and the perinatal results of the infected fetuses and also to evaluate the relationship between the most used maternal-fetal diagnostic tests for toxoplasmosis during pregnancy and the relationship between age and acute toxoplasmosis infection during pregnancy. METHODS: longitudinal prospective study of 32,512 pregnant women attended by The Pregnancy Protection Program of the State of Mato Grosso do Sul - Brazil, from November 2002 to October 2003. ELISA (IgG and IgM) and IgG avidity test were performed for maternal diagnosis and amniotic fluid PCR for fetal investigation of the infection. The relationship between data was analyzed statistically by the chi2 or two-sided Fisher's exact test in contingency tables. RESULTS: a 0.42% frequency of acute Toxoplasma gondii infection among pregnant population was found, where 92% were previously exposed and 8% were susceptible. Among IgM-positive pregnant women, the age ranged from 14 to 39 years, with a mean of 23±5.9 years. There was no statistically significant relationship between age and maternal acute T. gondii infection (p=0.73). The vertical transmission rate was 3.9%. A statistically significant relationship was shown (p=0.001) between a lower avidity IgG test (<30%) and the presence of fetal infection and a higher IgG avidity test (>60%) and the absence of fetal infection. There was a statistically significant association (p=0.001) between fetal infection (amniotic fluid PCR) and neonatal infection. CONCLUSIONS: maternal acute toxoplasmosis frequency was lower than the Brazilian national parameters, whereas vertical transmission rate did not differ from the rates found in other studies. The IgG avidity test, when associated with gestational age and the examination date, was useful to evaluate the therapeutical options and to consider the risk of vertical transmission when performed before 12 weeks. Positive PCR in amniotic fluid showed a positive relationship with the worst neonatal prognosis, being a specific method in diagnosing intrauterine fetal infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):442-449
DOI 10.1590/S0100-72032005000800002
PURPOSE: to establish the frequency of acute toxoplasmosis in pregnant women, vertical transmission rate and the perinatal results of the infected fetuses and also to evaluate the relationship between the most used maternal-fetal diagnostic tests for toxoplasmosis during pregnancy and the relationship between age and acute toxoplasmosis infection during pregnancy. METHODS: longitudinal prospective study of 32,512 pregnant women attended by The Pregnancy Protection Program of the State of Mato Grosso do Sul - Brazil, from November 2002 to October 2003. ELISA (IgG and IgM) and IgG avidity test were performed for maternal diagnosis and amniotic fluid PCR for fetal investigation of the infection. The relationship between data was analyzed statistically by the chi2 or two-sided Fisher's exact test in contingency tables. RESULTS: a 0.42% frequency of acute Toxoplasma gondii infection among pregnant population was found, where 92% were previously exposed and 8% were susceptible. Among IgM-positive pregnant women, the age ranged from 14 to 39 years, with a mean of 23±5.9 years. There was no statistically significant relationship between age and maternal acute T. gondii infection (p=0.73). The vertical transmission rate was 3.9%. A statistically significant relationship was shown (p=0.001) between a lower avidity IgG test (<30%) and the presence of fetal infection and a higher IgG avidity test (>60%) and the absence of fetal infection. There was a statistically significant association (p=0.001) between fetal infection (amniotic fluid PCR) and neonatal infection. CONCLUSIONS: maternal acute toxoplasmosis frequency was lower than the Brazilian national parameters, whereas vertical transmission rate did not differ from the rates found in other studies. The IgG avidity test, when associated with gestational age and the examination date, was useful to evaluate the therapeutical options and to consider the risk of vertical transmission when performed before 12 weeks. Positive PCR in amniotic fluid showed a positive relationship with the worst neonatal prognosis, being a specific method in diagnosing intrauterine fetal infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):456-460
DOI 10.1590/S0100-72032005000800004
PURPOSE: to analyze the effectiveness and safety of exclusive hospital parenteral antibiotic therapy to treat puerperal endometritis in a population of low socioeconomic level. METHODS: a prospective clinical trial evaluated 21 puerperae with a diagnosis of postpartum endometritis, whose deliveries occurred at a university hospital by cesarean section (52.4%) or normal delivery (47.6%). The sample was characterized by low socioeconomic and educational levels. The patients were submitted to a regimen of exclusive parenteral antibiotic, only during the hospitalization period (ATP-EX group). These results were compared with results obtained in a historical cohort in the same hospital (20 cases) submitted to a regimen of hospital parenteral antibiotic therapy complemented with ambulatory oral treatment (ATP+VO group). The patients were evaluated clinically on the occasion of periodic return visits in order to identify cases of recurrence and infectious complications. RESULTS: one patient from the ATP+VO group needed to be readmitted to the hospital on the 6th day after her discharge from the hospital with a diagnosis of endometritis recrudescence. No complications were observed among patients from ATP-EX group. CONCLUSION: for the treatment of puerperal endometritis, there was no additional advantage in using supplementary oral antibiotic therapy after patient discharge. The results using exclusive parenteral antibiotic treatment during hospitalization time indicate that it is effective and can be safely used in a population of low socioeconomic level.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):456-460
DOI 10.1590/S0100-72032005000800004
PURPOSE: to analyze the effectiveness and safety of exclusive hospital parenteral antibiotic therapy to treat puerperal endometritis in a population of low socioeconomic level. METHODS: a prospective clinical trial evaluated 21 puerperae with a diagnosis of postpartum endometritis, whose deliveries occurred at a university hospital by cesarean section (52.4%) or normal delivery (47.6%). The sample was characterized by low socioeconomic and educational levels. The patients were submitted to a regimen of exclusive parenteral antibiotic, only during the hospitalization period (ATP-EX group). These results were compared with results obtained in a historical cohort in the same hospital (20 cases) submitted to a regimen of hospital parenteral antibiotic therapy complemented with ambulatory oral treatment (ATP+VO group). The patients were evaluated clinically on the occasion of periodic return visits in order to identify cases of recurrence and infectious complications. RESULTS: one patient from the ATP+VO group needed to be readmitted to the hospital on the 6th day after her discharge from the hospital with a diagnosis of endometritis recrudescence. No complications were observed among patients from ATP-EX group. CONCLUSION: for the treatment of puerperal endometritis, there was no additional advantage in using supplementary oral antibiotic therapy after patient discharge. The results using exclusive parenteral antibiotic treatment during hospitalization time indicate that it is effective and can be safely used in a population of low socioeconomic level.