Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(3):121-123
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(3):121-123
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(2):122-125
DOI 10.1590/S0100-72032006000200008
PURPOSE: to evaluate the prevalence of hemoglobin S (HbS) in newborns, through clinical investigation and laboratory data. METHODS: a protocol established the drawing of 10 mL blood from the umbilical cord after its ligature and section, immediately after birth. The samples were kept in a tube with 5% EDTA and then submitted to high-performance liquid chromatography. The study included a clinical record taken from an interview with the mother, her physical and biochemical condition, as well as that of her newborn. Main criteria were newborn's weight, sex, first minute Apgar, and the mother's color. Statistical analysis was based on the Epi-Info 6.0 program and performed by Student's t test, with the level of significance set at p<0.05. RESULTS: from August 2001 to September 2002, 389 umbilical cord blood samples showed HbS in 16 newborn babies (4.1%). Fifteen of these presented sickle-cell traits (HbS) and the other had a diagnostic hypothesis of sickle-cell anemia (HbSS). Hemoglobinopathy prevailed among male babies. No significant difference was observed between newborns with or without HbS regarding averages of weight and Apgar scores; the same occurred regarding the mother's skin color (Caucasians, mulattos and blacks). CONCLUSION: searching for hemoglobin diseases in newborns should be considered because of the possibility of 25% sickle-cell anemia in the offspring of couples with sickle-cell traits. Screening for abnormal hemoglobin is important in the population at risk. Thus, the creation of programs with these aims is recommended to be included in hospital routines.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(2):122-125
DOI 10.1590/S0100-72032006000200008
PURPOSE: to evaluate the prevalence of hemoglobin S (HbS) in newborns, through clinical investigation and laboratory data. METHODS: a protocol established the drawing of 10 mL blood from the umbilical cord after its ligature and section, immediately after birth. The samples were kept in a tube with 5% EDTA and then submitted to high-performance liquid chromatography. The study included a clinical record taken from an interview with the mother, her physical and biochemical condition, as well as that of her newborn. Main criteria were newborn's weight, sex, first minute Apgar, and the mother's color. Statistical analysis was based on the Epi-Info 6.0 program and performed by Student's t test, with the level of significance set at p<0.05. RESULTS: from August 2001 to September 2002, 389 umbilical cord blood samples showed HbS in 16 newborn babies (4.1%). Fifteen of these presented sickle-cell traits (HbS) and the other had a diagnostic hypothesis of sickle-cell anemia (HbSS). Hemoglobinopathy prevailed among male babies. No significant difference was observed between newborns with or without HbS regarding averages of weight and Apgar scores; the same occurred regarding the mother's skin color (Caucasians, mulattos and blacks). CONCLUSION: searching for hemoglobin diseases in newborns should be considered because of the possibility of 25% sickle-cell anemia in the offspring of couples with sickle-cell traits. Screening for abnormal hemoglobin is important in the population at risk. Thus, the creation of programs with these aims is recommended to be included in hospital routines.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):122-127
DOI 10.1590/S0100-72032012000300006
PURPOSE: To compare the diagnostic accuracy of sonohysterography (HSN) and conventional transvaginal ultrasound (USG) in assessing the uterine cavity of infertile women candidate to assisted reproduction techniques (ART). METHODS: Comparative cross-sectional study with 120 infertile women candidate to ART, assisted at Centro de Reprodução Assistida (CRA) of Hospital Regional da Asa Sul (HRAS), Brasília - DF, from August 2009 to November 2010. Sonohysterography was performed with saline solution infusion in a close system. The sonohysterography finding was compared to previous USG results. The uterine cavity was considered abnormal when the endometrium was found to be thicker than expected during the menstrual cycle and when an endometrial polyp, a submucous myoma and an abnormal shape of the uterine cavity were observed. The statistical analysis was done using absolute frequencies, percentage values and the χ², with the level of significance set at 5%. RESULTS: HSN revealed that 92 (76.7%) infertile women candidate to ART had a normal uterine cavity, while 28 (23.3%) had the following abnormalities: 15 polyps (12.5%), 9 cases of abnormal shape of the uterine cavity (7.5%), 6 submucous myomas (5%), 4 cases of inadequate endometrial thickness for the menstrual cycle phase (3.3%), and 2 cases of uterine septum (1.7%); 5 women presented more than one abnormality (4.2%). While USG showed alteration in the cavity only in 5 (4.2%) women, the sonohysterography confirmed 4 out of the 5 abnormalities shown by USG and detected an abnormal uterine cavity in 24 other women, who had not been detected by USG. This means that sonohysterography was able to detect more abnormalities in the uterine cavity than USG, with a statistically significant difference (p=0.002). CONCLUSION: The sonohysterography was more accurate than USG in the assessment of the uterine cavity of this cohort of infertile women candidate to ART. The sonohysterography can be easily incorporated into the investigation of these women and contribute to reducing embryo implantation failures.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):122-127
DOI 10.1590/S0100-72032012000300006
PURPOSE: To compare the diagnostic accuracy of sonohysterography (HSN) and conventional transvaginal ultrasound (USG) in assessing the uterine cavity of infertile women candidate to assisted reproduction techniques (ART). METHODS: Comparative cross-sectional study with 120 infertile women candidate to ART, assisted at Centro de Reprodução Assistida (CRA) of Hospital Regional da Asa Sul (HRAS), Brasília - DF, from August 2009 to November 2010. Sonohysterography was performed with saline solution infusion in a close system. The sonohysterography finding was compared to previous USG results. The uterine cavity was considered abnormal when the endometrium was found to be thicker than expected during the menstrual cycle and when an endometrial polyp, a submucous myoma and an abnormal shape of the uterine cavity were observed. The statistical analysis was done using absolute frequencies, percentage values and the χ², with the level of significance set at 5%. RESULTS: HSN revealed that 92 (76.7%) infertile women candidate to ART had a normal uterine cavity, while 28 (23.3%) had the following abnormalities: 15 polyps (12.5%), 9 cases of abnormal shape of the uterine cavity (7.5%), 6 submucous myomas (5%), 4 cases of inadequate endometrial thickness for the menstrual cycle phase (3.3%), and 2 cases of uterine septum (1.7%); 5 women presented more than one abnormality (4.2%). While USG showed alteration in the cavity only in 5 (4.2%) women, the sonohysterography confirmed 4 out of the 5 abnormalities shown by USG and detected an abnormal uterine cavity in 24 other women, who had not been detected by USG. This means that sonohysterography was able to detect more abnormalities in the uterine cavity than USG, with a statistically significant difference (p=0.002). CONCLUSION: The sonohysterography was more accurate than USG in the assessment of the uterine cavity of this cohort of infertile women candidate to ART. The sonohysterography can be easily incorporated into the investigation of these women and contribute to reducing embryo implantation failures.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(3):123-129
DOI 10.1590/S0100-72032013000300006
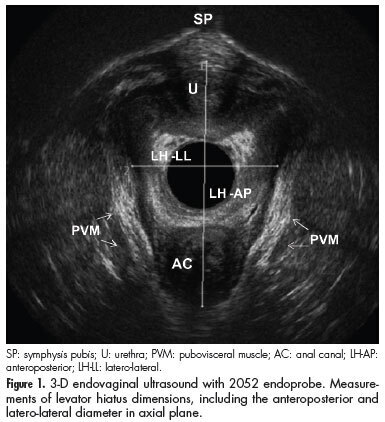
PURPOSE: To determine anatomical and functional pelvic floor measurements performed with three-dimensional (3-D) endovaginal ultrasonography in asymptomatic nulliparous women without dysfunctions detected in previous dynamic 3-D anorectal ultrasonography (echo defecography) and to demonstrate the interobserver reliability of these measurements. METHODS: Asymptomatic nulliparous volunteers were submitted to echo defecography to identify dynamic dysfunctions, including anatomical (rectocele, intussusceptions, entero/sigmoidocele and perineal descent) and functional changes (non-relaxation or paradoxical contraction of the puborectalis muscle) in the posterior compartment and assessed with regard to the biometric index of levator hiatus, pubovisceral muscle thickness, urethral length, anorectal angle, anorectal junction position and bladder neck position with the 3-D endovaginal ultrasonography. All measurements were compared at rest and during the Valsalva maneuver, and perineal and bladder neck descent was determined. The level of interobserver agreement was evaluated for all measurements. RESULTS: A total of 34 volunteers were assessed by echo defecography and by 3-D endovaginal ultrasonography. Out of these, 20 subjects met the inclusion criteria. The 14 excluded subjects were found to have posterior dynamic dysfunctions. During the Valsalva maneuver, the hiatal area was significantly larger, the urethra was significantly shorter and the anorectal angle was greater. Measurements at rest and during the Valsalva maneuver differed significantly with regard to anorectal junction and bladder neck position. The mean values for normal perineal descent and bladder neck descent were 0.6 cm and 0.5 cm above the symphysis pubis, respectively. The intraclass correlation coefficient ranged from 0.62-0.93. CONCLUSIONS: Functional biometric indexes, normal perineal descent and bladder neck descent values were determined for young asymptomatic nulliparous women with the 3-D endovaginal ultrasonography. The method was found to be reliable to measure pelvic floor structures at rest and during Valsalva, and might therefore be suitable for identifying dysfunctions in symptomatic patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(3):123-129
DOI 10.1590/S0100-72032013000300006
PURPOSE: To determine anatomical and functional pelvic floor measurements performed with three-dimensional (3-D) endovaginal ultrasonography in asymptomatic nulliparous women without dysfunctions detected in previous dynamic 3-D anorectal ultrasonography (echo defecography) and to demonstrate the interobserver reliability of these measurements. METHODS: Asymptomatic nulliparous volunteers were submitted to echo defecography to identify dynamic dysfunctions, including anatomical (rectocele, intussusceptions, entero/sigmoidocele and perineal descent) and functional changes (non-relaxation or paradoxical contraction of the puborectalis muscle) in the posterior compartment and assessed with regard to the biometric index of levator hiatus, pubovisceral muscle thickness, urethral length, anorectal angle, anorectal junction position and bladder neck position with the 3-D endovaginal ultrasonography. All measurements were compared at rest and during the Valsalva maneuver, and perineal and bladder neck descent was determined. The level of interobserver agreement was evaluated for all measurements. RESULTS: A total of 34 volunteers were assessed by echo defecography and by 3-D endovaginal ultrasonography. Out of these, 20 subjects met the inclusion criteria. The 14 excluded subjects were found to have posterior dynamic dysfunctions. During the Valsalva maneuver, the hiatal area was significantly larger, the urethra was significantly shorter and the anorectal angle was greater. Measurements at rest and during the Valsalva maneuver differed significantly with regard to anorectal junction and bladder neck position. The mean values for normal perineal descent and bladder neck descent were 0.6 cm and 0.5 cm above the symphysis pubis, respectively. The intraclass correlation coefficient ranged from 0.62-0.93. CONCLUSIONS: Functional biometric indexes, normal perineal descent and bladder neck descent values were determined for young asymptomatic nulliparous women with the 3-D endovaginal ultrasonography. The method was found to be reliable to measure pelvic floor structures at rest and during Valsalva, and might therefore be suitable for identifying dysfunctions in symptomatic patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):123-131
DOI 10.1590/S0100-72032011000700002
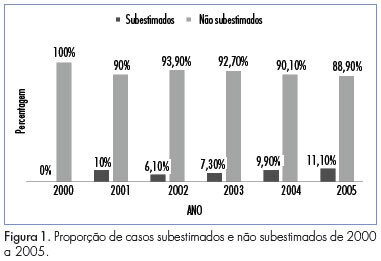
PURPOSE: To determine the rate of underestimation of an image-guided core biopsy of nonpalpable breast lesions, with validation by histologic examination after surgical excision. METHODS: We retrospectively reviewed 352 biopsies from patients who were submitted to surgery from February 2000 to December 2005, and whose histopathologic findings were recorded in the database system. Results were compared to surgical findings and underestimation rate was determined by dividing the number of lesions that proved to be carcinomas at surgical excision by the total number of lesions evaluated with excisional biopsy. Clinical, imaging, core biopsy and pathologic features were analyzed to identify factors that affect the rate of underestimation. The degree of agreement between the results was obtained by the percentage of agreement and Cohen's kappa coefficient. The association of variables with the underestimation of the diagnosis was determined by the chi-square, Fisher exact, ANOVA and Mann-Whitney U tests. The risk of underestimation was measured by the relative risk (RR) together with the respective 95% confidence intervals (95%CI). RESULTS: Inconclusive core biopsy findings occurred in 15.6% of cases. The histopathological result was benign in 26.4%, a high-risk lesion in 12.8% and malignant in 45.2%. There was agreement between core biopsy and surgery in 82.1% of cases (kappa=0.75). The false-negative rate was 5.4% and the lesion was completely removed in 3.4% of cases. The underestimation rate was 9.1% and was associated with BI-RADS® category 5 (p=0,01), microcalcifications (p CONCLUSIONS: The core breast biopsy under image guidance is a reliable procedure but the recommendation of surgical excision of high-risk lesions detected in the core biopsy remains since it was not possible to assess clinical, imaging, core biopsy and pathologic features that could predict underestimation and avoid excision. Representative samples are much more important than number of fragments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):123-131
DOI 10.1590/S0100-72032011000700002
PURPOSE: To determine the rate of underestimation of an image-guided core biopsy of nonpalpable breast lesions, with validation by histologic examination after surgical excision. METHODS: We retrospectively reviewed 352 biopsies from patients who were submitted to surgery from February 2000 to December 2005, and whose histopathologic findings were recorded in the database system. Results were compared to surgical findings and underestimation rate was determined by dividing the number of lesions that proved to be carcinomas at surgical excision by the total number of lesions evaluated with excisional biopsy. Clinical, imaging, core biopsy and pathologic features were analyzed to identify factors that affect the rate of underestimation. The degree of agreement between the results was obtained by the percentage of agreement and Cohen's kappa coefficient. The association of variables with the underestimation of the diagnosis was determined by the chi-square, Fisher exact, ANOVA and Mann-Whitney U tests. The risk of underestimation was measured by the relative risk (RR) together with the respective 95% confidence intervals (95%CI). RESULTS: Inconclusive core biopsy findings occurred in 15.6% of cases. The histopathological result was benign in 26.4%, a high-risk lesion in 12.8% and malignant in 45.2%. There was agreement between core biopsy and surgery in 82.1% of cases (kappa=0.75). The false-negative rate was 5.4% and the lesion was completely removed in 3.4% of cases. The underestimation rate was 9.1% and was associated with BI-RADS® category 5 (p=0,01), microcalcifications (p CONCLUSIONS: The core breast biopsy under image guidance is a reliable procedure but the recommendation of surgical excision of high-risk lesions detected in the core biopsy remains since it was not possible to assess clinical, imaging, core biopsy and pathologic features that could predict underestimation and avoid excision. Representative samples are much more important than number of fragments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):123-123
DOI 10.1590/S0100-72032001000200011
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):123-123
DOI 10.1590/S0100-72032001000200011
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):123-123
DOI 10.1590/S0100-72032001000200012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):123-123
DOI 10.1590/S0100-72032001000200012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(3):123-127
Expectant follow-up for biopsy-proven cervical intraepithelial neoplasia (CIN) 1 is the current recommendation for the management of this lesion. Nevertheless, the performance of the biopsy guided by colposcopy might not be optimal. Therefore, this study aimed to calculate the rate of underdiagnoses of more severe lesions in women with CIN 1 diagnosis and to evaluate whether age, lesion extent and biopsy site are factors associated with diagnostic failure.
Eighty women with a diagnosis of CIN 1 obtained by colposcopy-guided biopsy were selected for this study. These women were herein submitted to large loop excision of the transformation zone (LLETZ). The prevalence of lesions more severe than CIN 1 was calculated, and the histological diagnoses of the LLETZ specimens were grouped into two categories: "CIN 1 or less" and "CIN 2 or worse."
The prevalence of lesions diagnosed as CIN 2 or worse in the LLETZ specimens was of 19% (15/80). Three women revealed CIN 3, and 1 woman revealed a sclerosing adenocarcinoma stage I-a, a rare type of malignant neoplasia of low proliferation, which was not detected by either colposcopy or previous biopsy. The underdiagnosis of CIN 2 was not associated with the women's age, lesion extension and biopsy site.
The standard methods used for the diagnosis of CIN 1 may underestimate the severity of the true lesion and, therefore, women undergoing expectant management must have an adequate follow-up.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(3):123-127
Expectant follow-up for biopsy-proven cervical intraepithelial neoplasia (CIN) 1 is the current recommendation for the management of this lesion. Nevertheless, the performance of the biopsy guided by colposcopy might not be optimal. Therefore, this study aimed to calculate the rate of underdiagnoses of more severe lesions in women with CIN 1 diagnosis and to evaluate whether age, lesion extent and biopsy site are factors associated with diagnostic failure.
Eighty women with a diagnosis of CIN 1 obtained by colposcopy-guided biopsy were selected for this study. These women were herein submitted to large loop excision of the transformation zone (LLETZ). The prevalence of lesions more severe than CIN 1 was calculated, and the histological diagnoses of the LLETZ specimens were grouped into two categories: "CIN 1 or less" and "CIN 2 or worse."
The prevalence of lesions diagnosed as CIN 2 or worse in the LLETZ specimens was of 19% (15/80). Three women revealed CIN 3, and 1 woman revealed a sclerosing adenocarcinoma stage I-a, a rare type of malignant neoplasia of low proliferation, which was not detected by either colposcopy or previous biopsy. The underdiagnosis of CIN 2 was not associated with the women's age, lesion extension and biopsy site.
The standard methods used for the diagnosis of CIN 1 may underestimate the severity of the true lesion and, therefore, women undergoing expectant management must have an adequate follow-up.