Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(7):586-586
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(7):586-586
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(7):586-586
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(7):586-586
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(9):586-587
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(9):586-587
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):586-592
To determine if there is a correlation between body mass index (BMI) and climacteric symptoms in postmenopausal women.
The study sample was composed of 109 postmenopausal women with a mean age of 57 ± 8 years, mean body mass index (BMI) of 30 ± 6 kg/m2, and 8 ± 8 years after menopause. For the assessment of the climacteric symptoms, the Blatt-Kupperman Index (BKI), the Menopause Rating Scale (MRS), and the Cervantes Scale (CS) were used. Data analysis was performed through the Chi-squared test, analysis of variance (ANOVA) with the Bonferroni post hoc test, and multiple linear regression. The level of significance adopted was of p < 0.05. The statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, United States) software, version 26.0.
The multiple linear regression showed a positive association (p<0.01) between BMI values and menopause symptoms when adjusted for age and time after menopause in the 3 questionnaires used (BKI: B = 0.432; CS: B = 304; and MRS: B = 302). Regarding symptom scores, the obese women had higher mean scores (p<0.05) when compared to eutrophic women (BKI = 28 ± 10 and 20 ± 10; and MRS = 20 ± 10 and 13±7, respectively). In the Chi-squared analysis, 28% of obese women had severe symptoms and 46% had moderate symptoms, while only 1% and 46% of eutrophic women had these same symptoms.
There is an association between BMI and climacteric symptoms, and overweight or obese women have more intense and moderate symptoms than eutrophic women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):586-592
To determine if there is a correlation between body mass index (BMI) and climacteric symptoms in postmenopausal women.
The study sample was composed of 109 postmenopausal women with a mean age of 57 ± 8 years, mean body mass index (BMI) of 30 ± 6 kg/m2, and 8 ± 8 years after menopause. For the assessment of the climacteric symptoms, the Blatt-Kupperman Index (BKI), the Menopause Rating Scale (MRS), and the Cervantes Scale (CS) were used. Data analysis was performed through the Chi-squared test, analysis of variance (ANOVA) with the Bonferroni post hoc test, and multiple linear regression. The level of significance adopted was of p < 0.05. The statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, United States) software, version 26.0.
The multiple linear regression showed a positive association (p<0.01) between BMI values and menopause symptoms when adjusted for age and time after menopause in the 3 questionnaires used (BKI: B = 0.432; CS: B = 304; and MRS: B = 302). Regarding symptom scores, the obese women had higher mean scores (p<0.05) when compared to eutrophic women (BKI = 28 ± 10 and 20 ± 10; and MRS = 20 ± 10 and 13±7, respectively). In the Chi-squared analysis, 28% of obese women had severe symptoms and 46% had moderate symptoms, while only 1% and 46% of eutrophic women had these same symptoms.
There is an association between BMI and climacteric symptoms, and overweight or obese women have more intense and moderate symptoms than eutrophic women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(12):586-591
DOI 10.1590/S0100-72032009001200002
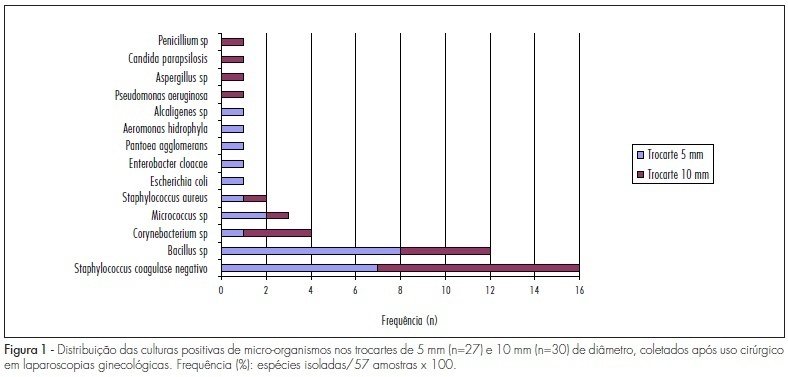
PURPOSE: to identify the microbial charge present in reusable trocars used in gynecological laparoscopies. METHODS: a descriptive exploratory study. An amount of 57 trocars, 30 with 10 mm of diameter and 27 with 5 mm, have been collected from the surgical unit, immediately after the surgery and placed in a sterilized recipient, in which 250 mL of sterile distilled water was added. Then, the trocars were agitated for the drainage of particles and to obtain a wash-out fluid to be analyzed. After being filtered through 0.22 µm cellulose membrane, the residue was placed on blood agar plates with a sterilized forceps. Following incubation, microbiological analysis has been done to count the number of colonies and further identify the microorganisms, using standard laboratorial techniques. RESULTS: microbial charge was recovered from 47.4% of the trocars analyzed. Among those, 45.6% presented 1 to 100 growing colonies. Fourteen types of microorganisms have been identified, among which the more frequently isolated were coagulase-negative Staphylococcus (28%) and Bacillus sp (21%), Aeromonas hydrophila, Alcaligenes sp, Candida parapsilosis, and enterobacteries were also identified. CONCLUSIONS: the study has demonstrated that the microbial challenge faced by the technician responsible for the cleaning and sterilization of trocars is low, as compared to the challenge imposed by biological markers. Nevertheless, it may be not inferred that the risks for infectious complications for patients are minimal.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(12):586-591
DOI 10.1590/S0100-72032009001200002
PURPOSE: to identify the microbial charge present in reusable trocars used in gynecological laparoscopies. METHODS: a descriptive exploratory study. An amount of 57 trocars, 30 with 10 mm of diameter and 27 with 5 mm, have been collected from the surgical unit, immediately after the surgery and placed in a sterilized recipient, in which 250 mL of sterile distilled water was added. Then, the trocars were agitated for the drainage of particles and to obtain a wash-out fluid to be analyzed. After being filtered through 0.22 µm cellulose membrane, the residue was placed on blood agar plates with a sterilized forceps. Following incubation, microbiological analysis has been done to count the number of colonies and further identify the microorganisms, using standard laboratorial techniques. RESULTS: microbial charge was recovered from 47.4% of the trocars analyzed. Among those, 45.6% presented 1 to 100 growing colonies. Fourteen types of microorganisms have been identified, among which the more frequently isolated were coagulase-negative Staphylococcus (28%) and Bacillus sp (21%), Aeromonas hydrophila, Alcaligenes sp, Candida parapsilosis, and enterobacteries were also identified. CONCLUSIONS: the study has demonstrated that the microbial challenge faced by the technician responsible for the cleaning and sterilization of trocars is low, as compared to the challenge imposed by biological markers. Nevertheless, it may be not inferred that the risks for infectious complications for patients are minimal.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(10):587-591
DOI 10.1590/S0100-72031999001000004
Objetivo: determinar se o não-fechamento dos folhetos peritoneais (visceral e parietal) na cesárea apresenta benefícios no intra e pós-operatório. Pacientes e Métodos: seiscentas e noventa e oito mulheres programadas para cesárea foram alocadas aleatoriamente em dois grupos: com sutura dos peritônios visceral e parietal (n = 349) e sem sutura dos peritônios (n = 349), na Maternidade da Encruzilhada (CISAM) em Recife, entre novembro de 1997 e dezembro de 1998. A análise estatística comparou as variáveis do intra-operatório e do pós-operatório entre os dois grupos. Não houve diferenças significativas entre os dois grupos em relação a idade, paridade, idade gestacional, antibiótico profilático, cefaléia pós-raquianestesia, cistite, amniorrexe prematura e indicações da cesárea. Resultados: o tempo cirúrgico, o número de fios categute simples e o uso de analgésico foram significativamente menores no grupo sem sutura do que no grupo com sutura. As incidências de febre, infecção de ferida operatória, endometrite foram similares nos dois grupos. Não houve diferenças quanto ao uso de antifisético, antiemético e óleo mineral. As médias de dias de permanência hospitalar foram similares nos dois grupos. Conclusões: o não-fechamento dos folhetos peritoneais não apresenta efeitos adversos no pós-operatório e, ao contrário, diminui o uso de analgésicos e no intra-operatório diminui o tempo e o número de fios categute simples.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(10):587-591
DOI 10.1590/S0100-72031999001000004
Objetivo: determinar se o não-fechamento dos folhetos peritoneais (visceral e parietal) na cesárea apresenta benefícios no intra e pós-operatório. Pacientes e Métodos: seiscentas e noventa e oito mulheres programadas para cesárea foram alocadas aleatoriamente em dois grupos: com sutura dos peritônios visceral e parietal (n = 349) e sem sutura dos peritônios (n = 349), na Maternidade da Encruzilhada (CISAM) em Recife, entre novembro de 1997 e dezembro de 1998. A análise estatística comparou as variáveis do intra-operatório e do pós-operatório entre os dois grupos. Não houve diferenças significativas entre os dois grupos em relação a idade, paridade, idade gestacional, antibiótico profilático, cefaléia pós-raquianestesia, cistite, amniorrexe prematura e indicações da cesárea. Resultados: o tempo cirúrgico, o número de fios categute simples e o uso de analgésico foram significativamente menores no grupo sem sutura do que no grupo com sutura. As incidências de febre, infecção de ferida operatória, endometrite foram similares nos dois grupos. Não houve diferenças quanto ao uso de antifisético, antiemético e óleo mineral. As médias de dias de permanência hospitalar foram similares nos dois grupos. Conclusões: o não-fechamento dos folhetos peritoneais não apresenta efeitos adversos no pós-operatório e, ao contrário, diminui o uso de analgésicos e no intra-operatório diminui o tempo e o número de fios categute simples.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(10):587-592
To evaluate the effects of pregnancy in systemic lupus erythematosus (SLE) patients.
The present article is a retrospective cohort study. Datawere collected from medical records of pregnant women with SLE from January 2002 to December 2012 at Universidade Estadual de Campinas, in the city of Campinas, state of São Paulo, Brazil. Systemic lupus erythematosus and disease activity were defined according to the American College of Rheumatology and the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) criteria respectively. The means, standard deviations (SDs), percentages and correlations were performed using the SAS software, version 9.4 (SAS Institute Inc., Cary, NC, US).
We obtained data from 69 pregnancies in 58 women. During pregnancy, a new flare was observed in 39.2% (n = 27). The manifestations were most common in patients with prior kidney disease, and mainly occurred during the third quarter and the puerperium. Renal activity occurred in 24.6% (n = 17), and serious activity, in 16% (n = 11). Of all deliveries, 75% (n = 48) were by cesarean section. Twomaternal deaths occurred (3%). Preterm birth was themain complication in the newborns. The abortion rate was 8.7%. Severe SLEDAI during pregnancy was associated with prematurity (100%) and perinatal death (54%).
Thematernal-fetal outcome is worse in SLE when thewomen experience a flare during pregnancy. The best maternal-fetal outcomes occur when the disease is in remission for at least 6 months before the pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(10):587-592
To evaluate the effects of pregnancy in systemic lupus erythematosus (SLE) patients.
The present article is a retrospective cohort study. Datawere collected from medical records of pregnant women with SLE from January 2002 to December 2012 at Universidade Estadual de Campinas, in the city of Campinas, state of São Paulo, Brazil. Systemic lupus erythematosus and disease activity were defined according to the American College of Rheumatology and the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) criteria respectively. The means, standard deviations (SDs), percentages and correlations were performed using the SAS software, version 9.4 (SAS Institute Inc., Cary, NC, US).
We obtained data from 69 pregnancies in 58 women. During pregnancy, a new flare was observed in 39.2% (n = 27). The manifestations were most common in patients with prior kidney disease, and mainly occurred during the third quarter and the puerperium. Renal activity occurred in 24.6% (n = 17), and serious activity, in 16% (n = 11). Of all deliveries, 75% (n = 48) were by cesarean section. Twomaternal deaths occurred (3%). Preterm birth was themain complication in the newborns. The abortion rate was 8.7%. Severe SLEDAI during pregnancy was associated with prematurity (100%) and perinatal death (54%).
Thematernal-fetal outcome is worse in SLE when thewomen experience a flare during pregnancy. The best maternal-fetal outcomes occur when the disease is in remission for at least 6 months before the pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):587-595
To identify the prevalence of maternal morbidity and its socioeconomic, demographic and health care associated factors in a city in Northeastern Brazil.
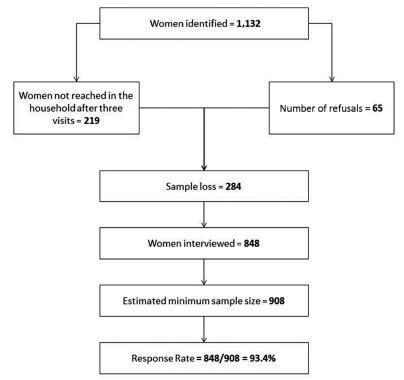
A cross-sectional and population-based study was conducted, with a design based on multi-stage complex sampling. A validated questionnaire was applied to 848 women aged between 15 and 49 years identified in 8,227 households from 60 census tracts of Natal, the capital of the state of Rio Grande do Norte (RN), Brazil. The main outcome measure was maternal morbidity. The Poisson regression analysis, with 5% significance, was used for the analysis of the associated factors.
The prevalence of maternal morbidity was of 21.2%. A bivariate analysis showed the following variables associated with an increased number of obstetric complications: non-white race (prevalence ratio [PR] =1.23; 95% confidence interval [95%CI]: 1.04-1.46); lower socioeconomic status (PR = 1.33; 95%CI: 1.12-1.58); prenatal care performed in public services (PR = 1.42; 95%CI: 1.16-1.72): women that were not advised during prenatal care about where they should deliver (PR = 1.24; 95%CI: 1.05-1.46); delivery in public services (PR = 1.63; 95%CI: 1.30-2.03); need to search for more than one hospital for delivery (PR = 1.22; 95%CI: 1.03-1.45); and no companion at all times of delivery care (PR = 1.25, 95%CI: 1.05-1.48). The place where the delivery occurred (public or private) and the socioeconomic status remained significant in the final model.
Women in a worse socioeconomic situation and whose delivery was performed in public services had a higher prevalence of maternal morbidity. Such an association reinforces the need to strengthen public policies to tackle health inequalities through actions focusing on these determinants.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):587-595
To identify the prevalence of maternal morbidity and its socioeconomic, demographic and health care associated factors in a city in Northeastern Brazil.
A cross-sectional and population-based study was conducted, with a design based on multi-stage complex sampling. A validated questionnaire was applied to 848 women aged between 15 and 49 years identified in 8,227 households from 60 census tracts of Natal, the capital of the state of Rio Grande do Norte (RN), Brazil. The main outcome measure was maternal morbidity. The Poisson regression analysis, with 5% significance, was used for the analysis of the associated factors.
The prevalence of maternal morbidity was of 21.2%. A bivariate analysis showed the following variables associated with an increased number of obstetric complications: non-white race (prevalence ratio [PR] =1.23; 95% confidence interval [95%CI]: 1.04-1.46); lower socioeconomic status (PR = 1.33; 95%CI: 1.12-1.58); prenatal care performed in public services (PR = 1.42; 95%CI: 1.16-1.72): women that were not advised during prenatal care about where they should deliver (PR = 1.24; 95%CI: 1.05-1.46); delivery in public services (PR = 1.63; 95%CI: 1.30-2.03); need to search for more than one hospital for delivery (PR = 1.22; 95%CI: 1.03-1.45); and no companion at all times of delivery care (PR = 1.25, 95%CI: 1.05-1.48). The place where the delivery occurred (public or private) and the socioeconomic status remained significant in the final model.
Women in a worse socioeconomic situation and whose delivery was performed in public services had a higher prevalence of maternal morbidity. Such an association reinforces the need to strengthen public policies to tackle health inequalities through actions focusing on these determinants.