Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(10):565-569
DOI 10.1590/S0100-72031998001000004
Purpose: to estimate the duration of cervical neoplasia from human pappilomavirus (HPV) infection to advanced invasive carcinoma, using as paremeter the mean age of the women at diagnosis. Methods: this cross-sectional study included 1,177 women with HPV infection, 1,561 with cervical intraepithelial neoplasia (CIN) and 773 with invasive carcinoma. Results: the mean ages of CIN 1 and CIN 2 on diagnosis were not statistically different. The mean duration of CIN 2 was 2.2 years. The mean duration of CIN 3 was 10.3 years, with 4.1 years as severe dysplasia and 6.2 years as carcinoma in situ (CIS). The mean duration of high grade squamous intraepithelial lesions was 12.5 years. The duration means of invasive carcinoma stages Ia, Ib and II were 3.0, 2.7 and 3.7 years, respectively. Conclusions: according to the results, CIN 1 and CIN 2 may arise directly from HPV infection and most of these lesions are transient. CIS presented the longest duration and the mean asymptomatic period of cervical neoplasia is 18.2 years. These results were discussed considering the present knowledge of the natural history of cervical carcinoma and other studies on duration of this neoplasia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(10):565-569
DOI 10.1590/S0100-72031998001000004
Purpose: to estimate the duration of cervical neoplasia from human pappilomavirus (HPV) infection to advanced invasive carcinoma, using as paremeter the mean age of the women at diagnosis. Methods: this cross-sectional study included 1,177 women with HPV infection, 1,561 with cervical intraepithelial neoplasia (CIN) and 773 with invasive carcinoma. Results: the mean ages of CIN 1 and CIN 2 on diagnosis were not statistically different. The mean duration of CIN 2 was 2.2 years. The mean duration of CIN 3 was 10.3 years, with 4.1 years as severe dysplasia and 6.2 years as carcinoma in situ (CIS). The mean duration of high grade squamous intraepithelial lesions was 12.5 years. The duration means of invasive carcinoma stages Ia, Ib and II were 3.0, 2.7 and 3.7 years, respectively. Conclusions: according to the results, CIN 1 and CIN 2 may arise directly from HPV infection and most of these lesions are transient. CIS presented the longest duration and the mean asymptomatic period of cervical neoplasia is 18.2 years. These results were discussed considering the present knowledge of the natural history of cervical carcinoma and other studies on duration of this neoplasia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):565-565
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):565-565
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):565-565
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):565-565
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(12):565-570
DOI 10.1590/SO100-720320150005488
To determine the influence of breastfeeding on the results of a postpartum oral glucose tolerance test in women recently diagnosed with gestational diabetes mellitus.
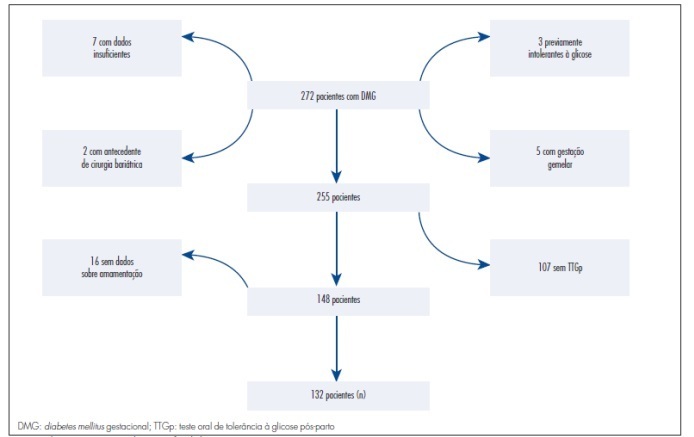
The data were obtained from the electronic medical records of the Endocrinopathy Sector during pregnancy, HCMED laboratory system ofHospital das Clínicas of São Paulo , and by telephone. According to the inclusion criteria adopted, 132 patients were eligible for the study. For statistical analysis, the patients were divided into two groups according to whether or not they breastfed. The results were analyzed by the Student t-test and by the Mann-Whitney, Chi-square and Fisher's exact tests, depending on the variable analyzed, with the level of significance set at p<0.05.
Of the 132 patients included in the study, 114 breastfed and 18 did not. Most of the patients in both groups were overweight or obese. The breastfeeding group had a lower pre-pregnancy Body Mass Index than the non-breastfeeding group (p=0.006). Insulin was introduced earlier in the group that did not breastfeed (23.21±4.33 versus 28.84±6.17; p=0.04). The group that did not breastfeed had a higher mean postpartum fasting glucose value in the oral glucose tolerance test than the group that breastfed (91.3±8.7 versus 86.5±9.3; p=0.01). Breastfeeding acted as a protective factor against the development of glucose intolerance in the postpartum oral glucose tolerance test (OR=0.27; 95%CI 0.09-0.8). By logistic regression, breastfeeding was shown to be an independent protective factor.
There was a statistically significant relationship between breastfeeding and a decreased risk of developing glucose intolerance. Breastfeeding should be encouraged because it is an effective, low cost intervention easily accessible to all patients during the postpartum period.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(12):565-570
DOI 10.1590/SO100-720320150005488
To determine the influence of breastfeeding on the results of a postpartum oral glucose tolerance test in women recently diagnosed with gestational diabetes mellitus.
The data were obtained from the electronic medical records of the Endocrinopathy Sector during pregnancy, HCMED laboratory system ofHospital das Clínicas of São Paulo , and by telephone. According to the inclusion criteria adopted, 132 patients were eligible for the study. For statistical analysis, the patients were divided into two groups according to whether or not they breastfed. The results were analyzed by the Student t-test and by the Mann-Whitney, Chi-square and Fisher's exact tests, depending on the variable analyzed, with the level of significance set at p<0.05.
Of the 132 patients included in the study, 114 breastfed and 18 did not. Most of the patients in both groups were overweight or obese. The breastfeeding group had a lower pre-pregnancy Body Mass Index than the non-breastfeeding group (p=0.006). Insulin was introduced earlier in the group that did not breastfeed (23.21±4.33 versus 28.84±6.17; p=0.04). The group that did not breastfeed had a higher mean postpartum fasting glucose value in the oral glucose tolerance test than the group that breastfed (91.3±8.7 versus 86.5±9.3; p=0.01). Breastfeeding acted as a protective factor against the development of glucose intolerance in the postpartum oral glucose tolerance test (OR=0.27; 95%CI 0.09-0.8). By logistic regression, breastfeeding was shown to be an independent protective factor.
There was a statistically significant relationship between breastfeeding and a decreased risk of developing glucose intolerance. Breastfeeding should be encouraged because it is an effective, low cost intervention easily accessible to all patients during the postpartum period.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):566-566
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):566-566
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):566-566
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(9):566-566
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(11):566-572
DOI 10.1590/S0100-72032008001100007
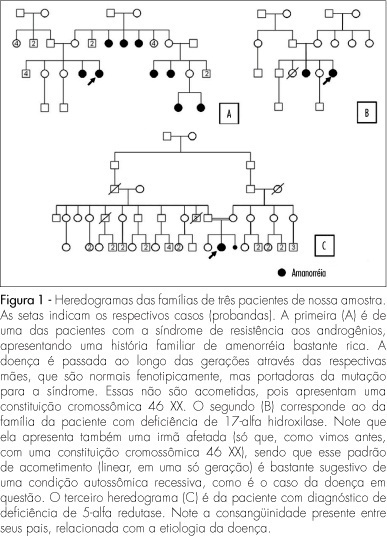
PURPOSE: to verify the prevalence and clinical characteristics of patients with primary amenorrhea and XY caryotype, evaluated in our Service, aiming at identifying findings which could help their recognition. METHODS: from January 1975 to November 2007, 104 patients with amenorrhea were evaluated. All the cases were analyzed by the caryotype by GTG bands. Among them, 21 (20.2%) presented a XY 46 constitution. Nevertheless, two of them were excluded from the study, because of incomplete data in their patient's chart. Most of the 19 patients who formed the sample had been referred to us by the gynecology clinics (63.2%). Their ages varied from 16 to 41 years old (an average of 22.1). Data were collected about their family and previous history, physical examination and results of complementary exams and the information was taken into consideration to determine the diagnosis. RESULTS: the predominant diagnosis was resistance to androgens syndrome (n=12; 63.2%); five patients (25.3%) presented XY pure gonadal dysgenesis (XY PGD), one (5.3%) 17 alpha-hydroxylase deficiency, and one (5.3%), 5 alpha-reductase deficiency. Clinical findings frequently found in these patients included abnormal development of secondary sexual characters (n=19), uterine agenesia with a blind vagina (n=14), family history of amenorrhea (n=8), and palpable gonads in the inguinal canal (n=5). Two of them presented a history of inguinal hernia. Systemic arterial hypertension was only diagnosed in the patient with 17 alpha-hydroxylase deficiency, and gonadal malignization, in the one with XY PGD. CONCLUSIONS: the rate of patients with XY caryotype (20%) was higher than the one described in the literature (3 to 11%). It is believed that this fact is related to the way patients are usually referred to our service. Some findings from the clinical history and from the physical examination should be evaluated as a routine in individuals with primary amenorrhea. This way, there would be a more precocious detection of XY 46 patients, and a better clinical management of them, as a consequence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(11):566-572
DOI 10.1590/S0100-72032008001100007
PURPOSE: to verify the prevalence and clinical characteristics of patients with primary amenorrhea and XY caryotype, evaluated in our Service, aiming at identifying findings which could help their recognition. METHODS: from January 1975 to November 2007, 104 patients with amenorrhea were evaluated. All the cases were analyzed by the caryotype by GTG bands. Among them, 21 (20.2%) presented a XY 46 constitution. Nevertheless, two of them were excluded from the study, because of incomplete data in their patient's chart. Most of the 19 patients who formed the sample had been referred to us by the gynecology clinics (63.2%). Their ages varied from 16 to 41 years old (an average of 22.1). Data were collected about their family and previous history, physical examination and results of complementary exams and the information was taken into consideration to determine the diagnosis. RESULTS: the predominant diagnosis was resistance to androgens syndrome (n=12; 63.2%); five patients (25.3%) presented XY pure gonadal dysgenesis (XY PGD), one (5.3%) 17 alpha-hydroxylase deficiency, and one (5.3%), 5 alpha-reductase deficiency. Clinical findings frequently found in these patients included abnormal development of secondary sexual characters (n=19), uterine agenesia with a blind vagina (n=14), family history of amenorrhea (n=8), and palpable gonads in the inguinal canal (n=5). Two of them presented a history of inguinal hernia. Systemic arterial hypertension was only diagnosed in the patient with 17 alpha-hydroxylase deficiency, and gonadal malignization, in the one with XY PGD. CONCLUSIONS: the rate of patients with XY caryotype (20%) was higher than the one described in the literature (3 to 11%). It is believed that this fact is related to the way patients are usually referred to our service. Some findings from the clinical history and from the physical examination should be evaluated as a routine in individuals with primary amenorrhea. This way, there would be a more precocious detection of XY 46 patients, and a better clinical management of them, as a consequence.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(11):566-573
DOI 10.1590/S0100-72032009001100007
PURPOSE: to identify the profile, tendency and causes of maternal death by pre-eclampsia/eclampsia in Paraná. METHODS: descriptive, transversal cohort study on maternal death by pre-eclampsia/eclampsia from 1997 to 2005. Data were obtained from case studies prepared by Maternal Death Committees that employ the Reproductive Age Mortality Survey Method to examine all the cases of death among women in fertile age. The general and specific maternal death rate (MDR) by pre-eclampsia/eclampsia were considered. To evaluate the tendency, triennial periods have been compared, two by two, taking into consideration the MDR of each period (p<0.05). In the triennial period from 2003 to 2005, 56 deaths by pre-eclampsia/eclampsia were analyzed. The variables focused were: age, income, schooling, gestation number and complications, pre-natal conditions, signs and symptoms related to the condition, delivery route, the time gestation was interrupted, the newborn conditions, access and treatment, ability to avoid and prevention measures. RESULTS: the general triennial MDR has presented significant decline, with 64.3/100,000 born-alive babies. There has been stability along the period for MDR by hypertensive disorder, with MDR of 11.8/100,000 born-alive. Primiparous women, women over 40 and with low socio-economical status have presented higher risks. In relation to the treatment, there has been underuse or inadequate use of conventional medicines for severe pre-eclampsia and eclampsia. The committees' analysis indicated that all the maternal death due to these conditions could have been avoided. CONCLUSIONS: actions aiming at minimizing the set of causes that lead to death by pre-eclampsia in Paraná should be enforced, including the training and monitoring of health professionals in order to apply the treatment protocols, besides the formalization of a reference net of clinics and hospitals, qualified for the care of high risk pregnancy and its intercurrences, to which pre-natal pregnant women are enrolled.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(11):566-573
DOI 10.1590/S0100-72032009001100007
PURPOSE: to identify the profile, tendency and causes of maternal death by pre-eclampsia/eclampsia in Paraná. METHODS: descriptive, transversal cohort study on maternal death by pre-eclampsia/eclampsia from 1997 to 2005. Data were obtained from case studies prepared by Maternal Death Committees that employ the Reproductive Age Mortality Survey Method to examine all the cases of death among women in fertile age. The general and specific maternal death rate (MDR) by pre-eclampsia/eclampsia were considered. To evaluate the tendency, triennial periods have been compared, two by two, taking into consideration the MDR of each period (p<0.05). In the triennial period from 2003 to 2005, 56 deaths by pre-eclampsia/eclampsia were analyzed. The variables focused were: age, income, schooling, gestation number and complications, pre-natal conditions, signs and symptoms related to the condition, delivery route, the time gestation was interrupted, the newborn conditions, access and treatment, ability to avoid and prevention measures. RESULTS: the general triennial MDR has presented significant decline, with 64.3/100,000 born-alive babies. There has been stability along the period for MDR by hypertensive disorder, with MDR of 11.8/100,000 born-alive. Primiparous women, women over 40 and with low socio-economical status have presented higher risks. In relation to the treatment, there has been underuse or inadequate use of conventional medicines for severe pre-eclampsia and eclampsia. The committees' analysis indicated that all the maternal death due to these conditions could have been avoided. CONCLUSIONS: actions aiming at minimizing the set of causes that lead to death by pre-eclampsia in Paraná should be enforced, including the training and monitoring of health professionals in order to apply the treatment protocols, besides the formalization of a reference net of clinics and hospitals, qualified for the care of high risk pregnancy and its intercurrences, to which pre-natal pregnant women are enrolled.