You searched for:"Geraldo Duarte"
We found (52) results for your search.Summary
Rev Bras Ginecol Obstet. 2004;26(3):241-245
DOI 10.1590/S0100-72032004000300011
The reduction of mother-to-child transmission (MTCT) of the HIV-1 using zidovudine (ZDV) represents a cornerstone in the prenatal and obstetrical care to these patients. The invasive fetal and obstetric procedures are proscribed in HIV-1 infected pregnant patients, to avoid the increased risk of MTCT of this virus. The authors present a case of an HIV-1 infected woman with recurrent polyhydramnios. Four ultrasound-guided amniotic punctures were performed in the 23rd, 26th, 27th and 29th weeks of gestation, each one draining the respective volumes of 1,800, 1,450, 1,700 and 1,960 ml of clear amniotic fluid. The patient started preterm labor with 30 weeks and 5 days resulting in vaginal delivery of a male neonate weighing 1,690g and measuring 43cm. The baby presented a post natal diagnosis of a sodium-losing nephropathy and was submitted to three negative polymerase chain reaction tests for HIV-1. The authors point out that the option to manage cases of HIV-1 infected pregnancies that could need invasive obstetric procedures should be to give the patient 2 mg//kg of ZDV endovenously before the procedure, in order to avoid MTCT of HIV-1, as it has demonstrated good results in this case.
Summary
Rev Bras Ginecol Obstet. 2004;26(3):241-245
DOI 10.1590/S0100-72032004000300011
The reduction of mother-to-child transmission (MTCT) of the HIV-1 using zidovudine (ZDV) represents a cornerstone in the prenatal and obstetrical care to these patients. The invasive fetal and obstetric procedures are proscribed in HIV-1 infected pregnant patients, to avoid the increased risk of MTCT of this virus. The authors present a case of an HIV-1 infected woman with recurrent polyhydramnios. Four ultrasound-guided amniotic punctures were performed in the 23rd, 26th, 27th and 29th weeks of gestation, each one draining the respective volumes of 1,800, 1,450, 1,700 and 1,960 ml of clear amniotic fluid. The patient started preterm labor with 30 weeks and 5 days resulting in vaginal delivery of a male neonate weighing 1,690g and measuring 43cm. The baby presented a post natal diagnosis of a sodium-losing nephropathy and was submitted to three negative polymerase chain reaction tests for HIV-1. The authors point out that the option to manage cases of HIV-1 infected pregnancies that could need invasive obstetric procedures should be to give the patient 2 mg//kg of ZDV endovenously before the procedure, in order to avoid MTCT of HIV-1, as it has demonstrated good results in this case.
Summary
Rev Bras Ginecol Obstet. 2004;26(3):249-249
Summary
Rev Bras Ginecol Obstet. 2004;26(3):249-249
Summary
Rev Bras Ginecol Obstet. 1999;21(5):251-258
DOI 10.1590/S0100-72031999000500002
Purpose: to evaluate whether prophylactic use of ampicillin could avoid or reduce maternal and perinatal infectious morbidity caused by premature rupture of membranes (PROM), and to extend the gestation period in those women. Methods: this was a prospective, randomized and double-blind study, carried out evaluating 121 pregnant women with PROM, randomized into two study groups. The treatment group (61 patients) received ampicillin and the control group (60 patients) received placebo. The placebo had the same characteristics as ampicillin (kind of packaging and color of the capsules) and was used in the same time regimen. The considered parameters for maternal infection were febrile morbidity (fever index), and the presence of chorioamnionitis and/or endometritis. The studied neonatal parameters were Apgar score (1st and 5th minutes), bacterial colonization of auditory canal, and blood culture. The statistical tests performed were Fisher's exact test, Wilcoxon, and chi². Results: it was observed that ampicillin did not prolong the gestation, nor did it reduce the postpartum febrile morbidity or the rates of chorioamnionitis and/or endometritis. Ampicillin did not reduce the perinatal infectious morbidity nor improve the birth outcomes. All these results were consistent in cases of less than 72 h PROM. The limited number of cases with time of PROM greater than 72 h did not permit statistical analysis free of type II error. Conclusions: based on these results it was possible to conclude that the prophylactic use of ampicillin by pregnant women with less than 72 h PROM did not reduce either infectious maternal or perinatal morbidity. However, the presence of group B Streptococcus agalactiae in the blood culture from a neonate in the control group showed the necessity to start antibiotic treatment of pregnant women colonized by this microorganism.
Summary
Rev Bras Ginecol Obstet. 1999;21(5):251-258
DOI 10.1590/S0100-72031999000500002
Purpose: to evaluate whether prophylactic use of ampicillin could avoid or reduce maternal and perinatal infectious morbidity caused by premature rupture of membranes (PROM), and to extend the gestation period in those women. Methods: this was a prospective, randomized and double-blind study, carried out evaluating 121 pregnant women with PROM, randomized into two study groups. The treatment group (61 patients) received ampicillin and the control group (60 patients) received placebo. The placebo had the same characteristics as ampicillin (kind of packaging and color of the capsules) and was used in the same time regimen. The considered parameters for maternal infection were febrile morbidity (fever index), and the presence of chorioamnionitis and/or endometritis. The studied neonatal parameters were Apgar score (1st and 5th minutes), bacterial colonization of auditory canal, and blood culture. The statistical tests performed were Fisher's exact test, Wilcoxon, and chi². Results: it was observed that ampicillin did not prolong the gestation, nor did it reduce the postpartum febrile morbidity or the rates of chorioamnionitis and/or endometritis. Ampicillin did not reduce the perinatal infectious morbidity nor improve the birth outcomes. All these results were consistent in cases of less than 72 h PROM. The limited number of cases with time of PROM greater than 72 h did not permit statistical analysis free of type II error. Conclusions: based on these results it was possible to conclude that the prophylactic use of ampicillin by pregnant women with less than 72 h PROM did not reduce either infectious maternal or perinatal morbidity. However, the presence of group B Streptococcus agalactiae in the blood culture from a neonate in the control group showed the necessity to start antibiotic treatment of pregnant women colonized by this microorganism.
Summary
Rev Bras Ginecol Obstet. 2016;38(6):263-265
Summary
Rev Bras Ginecol Obstet. 2016;38(6):263-265
Summary
Rev Bras Ginecol Obstet. 2006;28(5):304-309
DOI 10.1590/S0100-72032006000500007
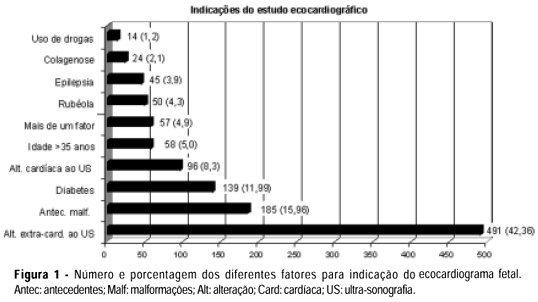
PURPOSE: to analyze the results of a screening and diagnostic program of arrhythmias and congenital heart disease in a reference hospital and the relevance of early diagnosis in the fetal and neonate evolution. METHODS: cardiac evaluation of 1159 fetuses was done in two different levels. Level I: by morphological ultrasound examination with the objective to detect the existence of either arrhythmias or structural cardiac malformations. Level II: by fetal echocardiography to establish the differential diagnosis. The results of level I in the arrhythmia group were compared with those of level II, and in the group with malformations the results of both levels were confronted with the neonate echocardiogram or necropsy. The kappa index was calculated to evaluate the concordance between the two levels. RESULTS: all detected arrhythmias in level I were confirmed in level II, there were no false negative cases and five patients with severe arrhythmia required pharmacological therapy. The diagnosis of structural malformation by level I had sensitivity of 72% and specificity of 98% and there were 28% of false-positive cases. In level II, the sensitivity and specificity of the diagnosis of congenital heart disease were 100 and 99%, respectively. The kappa index was 57% and indicated a moderate degree of concordance between the two levels. Fifty-one percent of the fetuses with diagnosis of cardiac malformations required pharmacological or invasive intervention immediately after birth. CONCLUSION: morphological ultrasound examination is a important tool in the screening of arrhythmias and congenital heart defects during fetal life. The sensitivity and specificity of the fetal echocardiogram were very high and the early diagnosis made it possible to treat the fetus with severe cardiac disease either during pregnancy or immediately after birth.
Summary
Rev Bras Ginecol Obstet. 2006;28(5):304-309
DOI 10.1590/S0100-72032006000500007
PURPOSE: to analyze the results of a screening and diagnostic program of arrhythmias and congenital heart disease in a reference hospital and the relevance of early diagnosis in the fetal and neonate evolution. METHODS: cardiac evaluation of 1159 fetuses was done in two different levels. Level I: by morphological ultrasound examination with the objective to detect the existence of either arrhythmias or structural cardiac malformations. Level II: by fetal echocardiography to establish the differential diagnosis. The results of level I in the arrhythmia group were compared with those of level II, and in the group with malformations the results of both levels were confronted with the neonate echocardiogram or necropsy. The kappa index was calculated to evaluate the concordance between the two levels. RESULTS: all detected arrhythmias in level I were confirmed in level II, there were no false negative cases and five patients with severe arrhythmia required pharmacological therapy. The diagnosis of structural malformation by level I had sensitivity of 72% and specificity of 98% and there were 28% of false-positive cases. In level II, the sensitivity and specificity of the diagnosis of congenital heart disease were 100 and 99%, respectively. The kappa index was 57% and indicated a moderate degree of concordance between the two levels. Fifty-one percent of the fetuses with diagnosis of cardiac malformations required pharmacological or invasive intervention immediately after birth. CONCLUSION: morphological ultrasound examination is a important tool in the screening of arrhythmias and congenital heart defects during fetal life. The sensitivity and specificity of the fetal echocardiogram were very high and the early diagnosis made it possible to treat the fetus with severe cardiac disease either during pregnancy or immediately after birth.
Summary
Rev Bras Ginecol Obstet. 2004;26(1):31-36
DOI 10.1590/S0100-72032004000100005
PURPOSE: to experimentally evaluate the diabetogenic effects of antiretroviral drugs on pregnant Wistar rats and the perinatal effects on the offspring. METHODS: adult female pregnant Wistar rats weighing 200-230 g were used. The antiretroviral drugs zidovudine (ZDV), lamivudine (3TC) and nelfinavir (NFV) were used alone and in association at daily doses of ten times the dose normally used in pregnant women, proportionally to the animal's body weight. Seven groups were studied, including the control. The experiment started on day 0 of pregnancy and the pregnant animals were sacrificed on day 21. The fetuses were counted and weighed. Blood determinations of glucose, insulin, glucagon and lactate were performed on day 21. The retroperitoneal adipose tissue was weighed. Data were analyzed statistically by Student's t-test. RESULTS: the groups treated with 3TC, ZDV + 3TC and ZDV + 3TC + NFV showed decreasing values of maternal daily body weight gain, retroperitoneal adipose tissue weight and weight of fetuses (control group: 6.2 g; 3TC group variation: 4.1-5.6 g). The serum lactate levels were also decreased when compared to the control in these groups (control group: 5.8 mmol/mL; 3TC group variations: 3.2-3.7 mmol/mL). All antiretroviral-treated groups showed a decreasing number of fetuses when compared to the control (control group: 14.7; drug group variation: 11.1-12.7). All treated groups also showed decreasing serum values of insulin (control group: 6.2 µIU/mL; drug group variation: 2.1 to 2.7 µIU/mL) and increasing serum levels of glucagon when compared to the control (control group: 88.2 pg/mL; drug group variation: 99.7 to 120.7 pg/mL). There was no statistical significance of glucose levels when comparing treated groups to the control. CONCLUSIONS: the antiretroviral drugs interfered in carbohydrate metabolism of pregnant rats and reduced the number of fetuses. 3TC caused less maternal body weight gain, decreased fetus weight and lactate and insulin levels and increased serum glucagon.
Summary
Rev Bras Ginecol Obstet. 2004;26(1):31-36
DOI 10.1590/S0100-72032004000100005
PURPOSE: to experimentally evaluate the diabetogenic effects of antiretroviral drugs on pregnant Wistar rats and the perinatal effects on the offspring. METHODS: adult female pregnant Wistar rats weighing 200-230 g were used. The antiretroviral drugs zidovudine (ZDV), lamivudine (3TC) and nelfinavir (NFV) were used alone and in association at daily doses of ten times the dose normally used in pregnant women, proportionally to the animal's body weight. Seven groups were studied, including the control. The experiment started on day 0 of pregnancy and the pregnant animals were sacrificed on day 21. The fetuses were counted and weighed. Blood determinations of glucose, insulin, glucagon and lactate were performed on day 21. The retroperitoneal adipose tissue was weighed. Data were analyzed statistically by Student's t-test. RESULTS: the groups treated with 3TC, ZDV + 3TC and ZDV + 3TC + NFV showed decreasing values of maternal daily body weight gain, retroperitoneal adipose tissue weight and weight of fetuses (control group: 6.2 g; 3TC group variation: 4.1-5.6 g). The serum lactate levels were also decreased when compared to the control in these groups (control group: 5.8 mmol/mL; 3TC group variations: 3.2-3.7 mmol/mL). All antiretroviral-treated groups showed a decreasing number of fetuses when compared to the control (control group: 14.7; drug group variation: 11.1-12.7). All treated groups also showed decreasing serum values of insulin (control group: 6.2 µIU/mL; drug group variation: 2.1 to 2.7 µIU/mL) and increasing serum levels of glucagon when compared to the control (control group: 88.2 pg/mL; drug group variation: 99.7 to 120.7 pg/mL). There was no statistical significance of glucose levels when comparing treated groups to the control. CONCLUSIONS: the antiretroviral drugs interfered in carbohydrate metabolism of pregnant rats and reduced the number of fetuses. 3TC caused less maternal body weight gain, decreased fetus weight and lactate and insulin levels and increased serum glucagon.
Summary
Rev Bras Ginecol Obstet. 2003;25(5):317-321
DOI 10.1590/S0100-72032003000500003
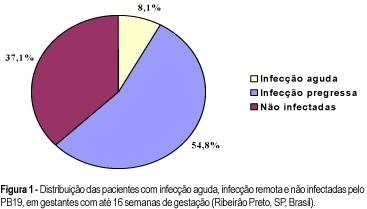
PURPOSE: to evaluate the rate of seropositivity for parvovirus B19 (PB19) among pregnant women and the rate of seroconversion against this infection during pregnancy. METHODS: prospective study carried out in the Hospital of the Medical School of Ribeirão Preto, University of São Paulo. In the first stage of the present study, we evaluated 245 pregnant women with gestational age less than 16 weeks to determine the seroprevalence of PB19 infection by ELISA. According to the serological results we determined if the PB19 infection was an acute infection (IgM positive and IgG negative or positive), or a former infection (IgM negative and IgG positive). In the second stage of this study, 73 previously seronegative pregnant women were tested again when they came to the hospital for delivery (IgM and IgG), to detect the seroconversion rate during pregnancy. RESULTS: the seroprevalence of the PB19 infection until 16 weeks of gestation was 62.9% (95% IC: 56.8-68.9), divided into acute infection (8.1%), or former infection (54.8%). Of the 73 patients, seronegative in the first stage of this investigation, seven (9.6%) showed seroconversion during pregnancy (95% IC: 2.8-16.3), two (2.7%) showed acute serological infection and five (6.9%) presented markers of past infection. The final seroprevalence of PB19 infection during pregnancy was 72.5%. CONCLUSIONS: considering that only the acute PB19 infection is associated with risk for vertical transmission, the high seroprevalence of this infection observed in this study would be protecting these fetuses against this form of infection. Despite the relatively high rate of seroconversion against PB19 infection during the pregnancy period, we did not observe any symptomatic neonate in this group.
Summary
Rev Bras Ginecol Obstet. 2003;25(5):317-321
DOI 10.1590/S0100-72032003000500003
PURPOSE: to evaluate the rate of seropositivity for parvovirus B19 (PB19) among pregnant women and the rate of seroconversion against this infection during pregnancy. METHODS: prospective study carried out in the Hospital of the Medical School of Ribeirão Preto, University of São Paulo. In the first stage of the present study, we evaluated 245 pregnant women with gestational age less than 16 weeks to determine the seroprevalence of PB19 infection by ELISA. According to the serological results we determined if the PB19 infection was an acute infection (IgM positive and IgG negative or positive), or a former infection (IgM negative and IgG positive). In the second stage of this study, 73 previously seronegative pregnant women were tested again when they came to the hospital for delivery (IgM and IgG), to detect the seroconversion rate during pregnancy. RESULTS: the seroprevalence of the PB19 infection until 16 weeks of gestation was 62.9% (95% IC: 56.8-68.9), divided into acute infection (8.1%), or former infection (54.8%). Of the 73 patients, seronegative in the first stage of this investigation, seven (9.6%) showed seroconversion during pregnancy (95% IC: 2.8-16.3), two (2.7%) showed acute serological infection and five (6.9%) presented markers of past infection. The final seroprevalence of PB19 infection during pregnancy was 72.5%. CONCLUSIONS: considering that only the acute PB19 infection is associated with risk for vertical transmission, the high seroprevalence of this infection observed in this study would be protecting these fetuses against this form of infection. Despite the relatively high rate of seroconversion against PB19 infection during the pregnancy period, we did not observe any symptomatic neonate in this group.
Summary
Rev Bras Ginecol Obstet. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.
Summary
Rev Bras Ginecol Obstet. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.