You searched for:"Francisco Jose Cândido dos Reis"
We found (25) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(1):1-2
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(1):1-2
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(9):549-552
DOI 10.1590/S0100-72031999000900008
Purpose: to evaluate the correlation between clinical and surgical staging of patients with vulvar carcinoma, according to the "Federação Internacional de Ginecologia e Obstetrícia" (FIGO 95). Methods: the authors studied 66 consecutive cases of vulvar carcinoma from 1977 to 1997. All patients were clinically staged to verify size and localization of the lesion as well as inguinal lymph node involvement and invasion of other organs. Forty-four patients were submitted to surgical treatment and 34 could be staged according to FIGO 95. Results: among the 34 patients staged through surgery, 17 (50%) showed agreement between clinical and surgical staging. Thus, in 17 patients the staging was different and in these the surgical staging was higher than the clinical in 13 cases and lower in 4 cases. We found in the clinical staging I, 2 cases that were surgical stage II and 1 case that was surgical stage III. Conclusion: the surgical staging could detect lymph node metastasis in patients with clinically negative nodes, as well as exclude false-positive cases. The clinical staging was not accurate for patients with vulvar carcinoma.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(9):549-552
DOI 10.1590/S0100-72031999000900008
Purpose: to evaluate the correlation between clinical and surgical staging of patients with vulvar carcinoma, according to the "Federação Internacional de Ginecologia e Obstetrícia" (FIGO 95). Methods: the authors studied 66 consecutive cases of vulvar carcinoma from 1977 to 1997. All patients were clinically staged to verify size and localization of the lesion as well as inguinal lymph node involvement and invasion of other organs. Forty-four patients were submitted to surgical treatment and 34 could be staged according to FIGO 95. Results: among the 34 patients staged through surgery, 17 (50%) showed agreement between clinical and surgical staging. Thus, in 17 patients the staging was different and in these the surgical staging was higher than the clinical in 13 cases and lower in 4 cases. We found in the clinical staging I, 2 cases that were surgical stage II and 1 case that was surgical stage III. Conclusion: the surgical staging could detect lymph node metastasis in patients with clinically negative nodes, as well as exclude false-positive cases. The clinical staging was not accurate for patients with vulvar carcinoma.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(12):744-749
DOI 10.1590/S0100-72032005001200007
PURPOSE: to assess to what extent the surgical staging differs from the clinical staging among cases of advanced uterine cervix carcinoma, and also to assess the percentage of cases with positive para-aortic ganglia in this group of patients. METHODS: this is a descriptive prospective study in which 36 patients with histological diagnosis of uterine cervix carcinoma considered locally advanced were included (stages IB2, IIB, IIIA and B, and IVA). The cases were submitted to clinical staging, according to FIGO criteria. All patients were to be treated with neoadjuvant chemotherapy. Age ranged from 40 to 73 years, with a mean of 56.2±7.9. The procedure started with pelvic lymphadenectomy followed by para-aortic lymphadenectomy, in case the pelvic lymph nodes were positive on surgical examination. Examination of the abdominal cavity and lymphadenectomy were done either through laparotomy or laparoscopy, chosen at random. In each case, the clinical staging was compared to the surgical staging, considered the gold standard. RESULTS: in the clinical staging (CS), 7 cases were classified as IB2 (tumors larger than 4 cm), 22 cases as CSII and 7 cases as CSIII. The surgical assessment changed the clinical staging as follows: the stage was decreased in six cases, and increased in 13. There was agreement only in 18 cases (50%). The para-aortic lymph nodes were affected in six cases. CONCLUSIONS: clinical staging of locally advanced uterine cervix carcinoma is incorrect in most of the cases. Such inconsistency may lead to excessive treatment in some cases, but about one fourth of the patients with positive para-aortic ganglia would not be adequately treated with the current standard treatment radiotherapy with chemosensitization, which aims at the local regional control of the pelvic disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(12):744-749
DOI 10.1590/S0100-72032005001200007
PURPOSE: to assess to what extent the surgical staging differs from the clinical staging among cases of advanced uterine cervix carcinoma, and also to assess the percentage of cases with positive para-aortic ganglia in this group of patients. METHODS: this is a descriptive prospective study in which 36 patients with histological diagnosis of uterine cervix carcinoma considered locally advanced were included (stages IB2, IIB, IIIA and B, and IVA). The cases were submitted to clinical staging, according to FIGO criteria. All patients were to be treated with neoadjuvant chemotherapy. Age ranged from 40 to 73 years, with a mean of 56.2±7.9. The procedure started with pelvic lymphadenectomy followed by para-aortic lymphadenectomy, in case the pelvic lymph nodes were positive on surgical examination. Examination of the abdominal cavity and lymphadenectomy were done either through laparotomy or laparoscopy, chosen at random. In each case, the clinical staging was compared to the surgical staging, considered the gold standard. RESULTS: in the clinical staging (CS), 7 cases were classified as IB2 (tumors larger than 4 cm), 22 cases as CSII and 7 cases as CSIII. The surgical assessment changed the clinical staging as follows: the stage was decreased in six cases, and increased in 13. There was agreement only in 18 cases (50%). The para-aortic lymph nodes were affected in six cases. CONCLUSIONS: clinical staging of locally advanced uterine cervix carcinoma is incorrect in most of the cases. Such inconsistency may lead to excessive treatment in some cases, but about one fourth of the patients with positive para-aortic ganglia would not be adequately treated with the current standard treatment radiotherapy with chemosensitization, which aims at the local regional control of the pelvic disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
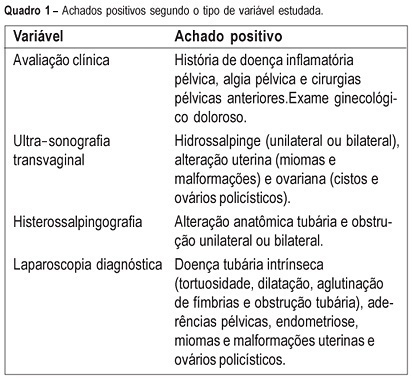
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(6):331-339
DOI 10.1590/S0100-72032005000600007
PURPOSE: to evaluate the epidemiologic data and signs of trophoblastic hyperplasia in patients with complete hydatidiform mole (CHM) and to estimate the risk associated with the persistence of the disease. METHODS:: we evaluated 214 patients with CHM submitted to uterine evacuation between 1980 and 2001. The patients were included prospectively. All patients were followed until negative bHCG with weekly clinical evaluation and bHCG quantification. We considered persistence when the patient needed another treatment after uterine evacuation. The risk factors for persistence were evaluated through univariate and multivariate analysis, and the odds ratio (OR) was calculated for each one. RESULTS: among the epidemiologic factors, only negative Rh was significant (OR=2.28). All signs of trophoblastic hyperplasia, represented by uterine size larger than expected, sonographic uterine volume, tecaluteinic cysts, and betaHCG higher than 10(5) were associated with risk for the presistence of the disease. The presence of at least one sign of trophoblastic hyperplasia showed sensitivity of 82% and predictive positive value of 35.1% (OR=4.8). The logistic regression identified larger uterine size than expected and bHCG higher than 10(5) as risk factors for persistence of the gestational trophoblastic disease (OR=4.1 and 5.5, respectively). CONCLUSIONS: the signs of trophoblastic hyperplasia showed good sensitivity to predict persistence of the disease; however, the low predictive positive value does not allow using these criteria to change treatment. It is very important to reinforce the importance of serial betaHCG quantification in these high-risk patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(6):331-339
DOI 10.1590/S0100-72032005000600007
PURPOSE: to evaluate the epidemiologic data and signs of trophoblastic hyperplasia in patients with complete hydatidiform mole (CHM) and to estimate the risk associated with the persistence of the disease. METHODS:: we evaluated 214 patients with CHM submitted to uterine evacuation between 1980 and 2001. The patients were included prospectively. All patients were followed until negative bHCG with weekly clinical evaluation and bHCG quantification. We considered persistence when the patient needed another treatment after uterine evacuation. The risk factors for persistence were evaluated through univariate and multivariate analysis, and the odds ratio (OR) was calculated for each one. RESULTS: among the epidemiologic factors, only negative Rh was significant (OR=2.28). All signs of trophoblastic hyperplasia, represented by uterine size larger than expected, sonographic uterine volume, tecaluteinic cysts, and betaHCG higher than 10(5) were associated with risk for the presistence of the disease. The presence of at least one sign of trophoblastic hyperplasia showed sensitivity of 82% and predictive positive value of 35.1% (OR=4.8). The logistic regression identified larger uterine size than expected and bHCG higher than 10(5) as risk factors for persistence of the gestational trophoblastic disease (OR=4.1 and 5.5, respectively). CONCLUSIONS: the signs of trophoblastic hyperplasia showed good sensitivity to predict persistence of the disease; however, the low predictive positive value does not allow using these criteria to change treatment. It is very important to reinforce the importance of serial betaHCG quantification in these high-risk patients.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(4):222-227
DOI 10.1590/S0100-72032005000400010
O câncer de ovário é a neoplasia ginecológica mais letal e a sobrevida global é inferior a 40% em cinco anos. Isto ocorre principalmente porque a maioria das pacientes apresenta estadios avançados no momento do diagnóstico. Nestes casos as opções terapêuticas - citorredução e quimioterapia - são apenas parcialmente efetivas. Quando diagnosticado precocemente, por outro lado, a sobrevida em cinco anos é superior a 90% e a cirurgia geralmente é o único tratamento necessário. No entanto, em função da baixa prevalência do câncer de ovário na população, mesmo testes muito específicos produzem altas taxas de resultados falso-positivos e aumento de intervenções cirúrgicas para abordar massas anexiais assintomáticas. Com base nestes fatos, é essencial a busca de métodos e estratégias para se detectar estes tumores em estádios iniciais e ao mesmo tempo evitar intervenções desnecessárias. Neste artigo são revisadas as bases e as possíveis conseqüências de estratégias para a detecção precoce dos tumores ovarianos. São discutidos os principais métodos disponíveis e os resultados de alguns estudos com este objetivo.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(4):222-227
DOI 10.1590/S0100-72032005000400010
O câncer de ovário é a neoplasia ginecológica mais letal e a sobrevida global é inferior a 40% em cinco anos. Isto ocorre principalmente porque a maioria das pacientes apresenta estadios avançados no momento do diagnóstico. Nestes casos as opções terapêuticas - citorredução e quimioterapia - são apenas parcialmente efetivas. Quando diagnosticado precocemente, por outro lado, a sobrevida em cinco anos é superior a 90% e a cirurgia geralmente é o único tratamento necessário. No entanto, em função da baixa prevalência do câncer de ovário na população, mesmo testes muito específicos produzem altas taxas de resultados falso-positivos e aumento de intervenções cirúrgicas para abordar massas anexiais assintomáticas. Com base nestes fatos, é essencial a busca de métodos e estratégias para se detectar estes tumores em estádios iniciais e ao mesmo tempo evitar intervenções desnecessárias. Neste artigo são revisadas as bases e as possíveis conseqüências de estratégias para a detecção precoce dos tumores ovarianos. São discutidos os principais métodos disponíveis e os resultados de alguns estudos com este objetivo.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(3):253-253
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(3):253-253