Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(9):464-470
To describe the blood flow velocities and impedance indices changes in the uterine arteries of leiomyomatous uteri using Doppler sonography.
This was a prospective, case-control study conducted on 140 premenopausal women with sonographic diagnosis of uterine leiomyoma and 140 premenopausal controls without leiomyomas. Pelvic sonography was performed to diagnose and characterize the leiomyomas. The hemodynamics of the ascending branches of both main uterine arteries was assessed by Doppler interrogation. Statistical analysis was performed mainly using non-parametric tests.
The median uterine volume of the subjects was 556 cm3, while that of the controls was 90.5 cm3 (p < 0.001). The mean peak systolic velocity (PSV), end-diastolic velocity (EDV), time-averaged maximum velocity (TAMX), time-averaged mean velocity (Tmean), acceleration time (AT), acceleration index (AI), diastolic/systolic ratio (DSR), diastolic average ratio (DAR), and inverse pulsatility index (PI) were significantly higher in the subjects (94.2 cm/s, 29.7 cm/s, 49.1 cm/s, 25.5 cm/s, 118 ms, 0.8, 0.3, 0.6, and 0.8 respectively) compared with the controls (54.2 cm/s, 7.7 cm/s, 20.0 cm/s, 10.0 cm/s, 92.0 ms, 0.6, 0.1, 0.4, and 0.4 respectively); p < 0.001 for all values. Conversely, the mean PI, resistivity index (RI), systolic/diastolic ratio (SDR) and impedance index (ImI) of the subjects (1.52, 0.70, 3.81, and 3.81 respectively) were significantly lower than those of the controls (2.38, 0.86, 7.23, and 7.24 respectively); p < 0.001 for all values.
There is a significantly increased perfusion of leiomyomatous uteri that is most likely due to uterine enlargement.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(9):464-470
To describe the blood flow velocities and impedance indices changes in the uterine arteries of leiomyomatous uteri using Doppler sonography.
This was a prospective, case-control study conducted on 140 premenopausal women with sonographic diagnosis of uterine leiomyoma and 140 premenopausal controls without leiomyomas. Pelvic sonography was performed to diagnose and characterize the leiomyomas. The hemodynamics of the ascending branches of both main uterine arteries was assessed by Doppler interrogation. Statistical analysis was performed mainly using non-parametric tests.
The median uterine volume of the subjects was 556 cm3, while that of the controls was 90.5 cm3 (p < 0.001). The mean peak systolic velocity (PSV), end-diastolic velocity (EDV), time-averaged maximum velocity (TAMX), time-averaged mean velocity (Tmean), acceleration time (AT), acceleration index (AI), diastolic/systolic ratio (DSR), diastolic average ratio (DAR), and inverse pulsatility index (PI) were significantly higher in the subjects (94.2 cm/s, 29.7 cm/s, 49.1 cm/s, 25.5 cm/s, 118 ms, 0.8, 0.3, 0.6, and 0.8 respectively) compared with the controls (54.2 cm/s, 7.7 cm/s, 20.0 cm/s, 10.0 cm/s, 92.0 ms, 0.6, 0.1, 0.4, and 0.4 respectively); p < 0.001 for all values. Conversely, the mean PI, resistivity index (RI), systolic/diastolic ratio (SDR) and impedance index (ImI) of the subjects (1.52, 0.70, 3.81, and 3.81 respectively) were significantly lower than those of the controls (2.38, 0.86, 7.23, and 7.24 respectively); p < 0.001 for all values.
There is a significantly increased perfusion of leiomyomatous uteri that is most likely due to uterine enlargement.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(8):465-470
To describe and evaluate the use of a simple, low-cost, and reproducible simulator for teaching the repair of obstetric anal sphincter injuries (OASIS).
Twenty resident doctors in obstetrics and gynecology and four obstetricians participated in the simulation. A fourth-degree tear model was created using lowcost materials (condom simulating the rectal mucosa, cotton tissue simulating the internal anal sphincter, and bovine meat simulating the external anal sphincter). The simulator was initially assembled with the aid of anatomical photos to study the anatomy and meaning of each component of the model. The laceration was created and repaired, using end-to-end or overlapping application techniques.
The model cost less than R$ 10.00 and was assembled without difficulty, which improved the knowledge of the participants of anatomy and physiology. The sutures of the layers (rectal mucosa, internal sphincter, and external sphincter) were performed in keeping with the surgical technique. All participants were satisfied with the simulation and felt it improved their knowledge and skills. Between 3 and 6 months after the training, 7 participants witnessed severe lacerations in their practice and reported that the simulation was useful for surgical correction.
The use of a simulator for repair training in OASIS is affordable (low-cost and easy to perform). The simulation seems to improve the knowledge and surgical skills necessary to repair severe lacerations. Further systematized studies should be performed for evaluation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(8):465-470
To describe and evaluate the use of a simple, low-cost, and reproducible simulator for teaching the repair of obstetric anal sphincter injuries (OASIS).
Twenty resident doctors in obstetrics and gynecology and four obstetricians participated in the simulation. A fourth-degree tear model was created using lowcost materials (condom simulating the rectal mucosa, cotton tissue simulating the internal anal sphincter, and bovine meat simulating the external anal sphincter). The simulator was initially assembled with the aid of anatomical photos to study the anatomy and meaning of each component of the model. The laceration was created and repaired, using end-to-end or overlapping application techniques.
The model cost less than R$ 10.00 and was assembled without difficulty, which improved the knowledge of the participants of anatomy and physiology. The sutures of the layers (rectal mucosa, internal sphincter, and external sphincter) were performed in keeping with the surgical technique. All participants were satisfied with the simulation and felt it improved their knowledge and skills. Between 3 and 6 months after the training, 7 participants witnessed severe lacerations in their practice and reported that the simulation was useful for surgical correction.
The use of a simulator for repair training in OASIS is affordable (low-cost and easy to perform). The simulation seems to improve the knowledge and surgical skills necessary to repair severe lacerations. Further systematized studies should be performed for evaluation.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(9):465-470
Infertility has a high prevalence in the general population, affecting 5 to 15% of couples in reproductive age. The assisted reproduction techniques ( ART ) include in vitro manipulation of gametes and embryos and are an important treatment indicated to these couples. It is well accepted that the implantation rate is positively influenced by the morphology of transferred embryos. However, we question if, apart from the assessment of embryo morphology, the number of produced embryos per cycle is also related to pregnancy rates in the first fresh transfer cycle.
To evaluate the clinical pregnancy rate according to the number of formed embryos and the transfer of top quality embryos ( TQEs ).
In a retrospective cohort study, between January 2011 and December 2012 , we evaluated women who underwent intracytoplasmic sperm injection (ICSI), aged < 40 years, andwith at least 1 formed embryo fresh transferred in cleavagestage. These women were stratified into 3 groups according to the number of formed embryos (1 embryo, 2-3 and ≥ 4 embryos). Each group was divided into 2 subgroups according to the presence or not of at least 1 transferred TQE (1 with TQE; 1 without TQE; 2-3 with TQE, 2-3 without TQE; ≥4with TQE; ≥4withoutTQE). The clinicalpregnancy rateswerecomparedineach subgroup based on the presence or absence of at least one transferred TQE.
During the study period, 636 women had at least one embryo to be transferred in thefirst fresh cycle (17.8% had 1 formed embryo [32.7% with TQEversus 67.3% without TQE], 42.1% of women had 2-3 formed embryos [55.6% with TQE versus 44.4% without TQE], and 40.1%ofpatientshad ≥4 formedembryos[73.7%withTQEversus26.3%withoutTQE]).The clinical pregnancy rate was significantly higher in the subgroup with ≥4 formed embryos with at least 1 transfered TQE (45.2%) compared with the subgroup without TQE (28.4%).
Having at least two available embryos and at least one TQE for embryo transfer are predictors of the pregnancy rates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(9):465-470
Infertility has a high prevalence in the general population, affecting 5 to 15% of couples in reproductive age. The assisted reproduction techniques ( ART ) include in vitro manipulation of gametes and embryos and are an important treatment indicated to these couples. It is well accepted that the implantation rate is positively influenced by the morphology of transferred embryos. However, we question if, apart from the assessment of embryo morphology, the number of produced embryos per cycle is also related to pregnancy rates in the first fresh transfer cycle.
To evaluate the clinical pregnancy rate according to the number of formed embryos and the transfer of top quality embryos ( TQEs ).
In a retrospective cohort study, between January 2011 and December 2012 , we evaluated women who underwent intracytoplasmic sperm injection (ICSI), aged < 40 years, andwith at least 1 formed embryo fresh transferred in cleavagestage. These women were stratified into 3 groups according to the number of formed embryos (1 embryo, 2-3 and ≥ 4 embryos). Each group was divided into 2 subgroups according to the presence or not of at least 1 transferred TQE (1 with TQE; 1 without TQE; 2-3 with TQE, 2-3 without TQE; ≥4with TQE; ≥4withoutTQE). The clinicalpregnancy rateswerecomparedineach subgroup based on the presence or absence of at least one transferred TQE.
During the study period, 636 women had at least one embryo to be transferred in thefirst fresh cycle (17.8% had 1 formed embryo [32.7% with TQEversus 67.3% without TQE], 42.1% of women had 2-3 formed embryos [55.6% with TQE versus 44.4% without TQE], and 40.1%ofpatientshad ≥4 formedembryos[73.7%withTQEversus26.3%withoutTQE]).The clinical pregnancy rate was significantly higher in the subgroup with ≥4 formed embryos with at least 1 transfered TQE (45.2%) compared with the subgroup without TQE (28.4%).
Having at least two available embryos and at least one TQE for embryo transfer are predictors of the pregnancy rates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(7):465-468
DOI 10.1590/S0100-72032001000700009
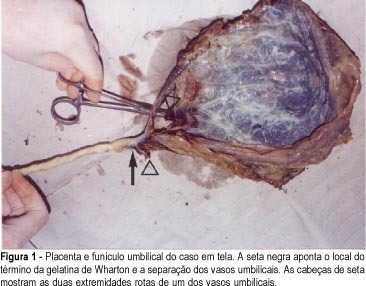
The differential diagnosis of hemorrhages during the third trimester of pregnancy due exclusively to obstetrical causes includes: abruptio placentae, low insertion of placenta (placenta previa with subtypes), rupture of the uterus, rupture of the marginal placental sinus and rupture of the vasa previa. The three first diagnoses occur more frequently, their epidemiological factors are better known and therefore, have an easier diagnosis. It is common for obstetricians with long practical experience, as well as for ultrasonographers specialized in fetal medicine and who thoroughly know their theory, not to have ever been exposed to practical obstetrical cases of vasa previa or their rupture. The reason to write this article was the fact that, during the past 32 years, we have been working constantly and uninterruptedly in obstetrical practice and we have seen only one case of rupture of vasa previa during labor, which killed the fetus. Initially, we investigated the issue in obstetrical textbooks having no luck whatsoever, except for a couple of lines on the subject. Carrying out our search in depth, we were able to learn that, even though a rarity, today's literature on the subject suggests that it is possible to have a diagnosis for this morbid entity during gestation, and to solve the problem by making the cesarian section mandatory in these cases, leading to a significant reduction in the actual fetal mortality figures which, according to experts, vary between 33 and 100%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(7):465-468
DOI 10.1590/S0100-72032001000700009
The differential diagnosis of hemorrhages during the third trimester of pregnancy due exclusively to obstetrical causes includes: abruptio placentae, low insertion of placenta (placenta previa with subtypes), rupture of the uterus, rupture of the marginal placental sinus and rupture of the vasa previa. The three first diagnoses occur more frequently, their epidemiological factors are better known and therefore, have an easier diagnosis. It is common for obstetricians with long practical experience, as well as for ultrasonographers specialized in fetal medicine and who thoroughly know their theory, not to have ever been exposed to practical obstetrical cases of vasa previa or their rupture. The reason to write this article was the fact that, during the past 32 years, we have been working constantly and uninterruptedly in obstetrical practice and we have seen only one case of rupture of vasa previa during labor, which killed the fetus. Initially, we investigated the issue in obstetrical textbooks having no luck whatsoever, except for a couple of lines on the subject. Carrying out our search in depth, we were able to learn that, even though a rarity, today's literature on the subject suggests that it is possible to have a diagnosis for this morbid entity during gestation, and to solve the problem by making the cesarian section mandatory in these cases, leading to a significant reduction in the actual fetal mortality figures which, according to experts, vary between 33 and 100%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(8):465-470
DOI 10.1590/S0100-72031999000800007
SUMMARY Objective: to evaluate the inclusion parameters in the selection of cases of (tubal) ectopic pregnancy for expectant management and to assess the results. Methods: a prospective study was carried out in 70 patients with unruptured (tubal) ectopic pregnancy, with the objective to carry out an expectant management. The main inclusion criteria in this study were the diameter of the tubal mass, that should be equal or inferior to 5,0 cm, reduced titles of beta-hCG (beta fraction of the chorionic gonadotropic hormone) as compared to the initial value within an interval of 48 h, hemodynamic stability, wishes for future pregnancy and a written permission to participate in the study. All patients were observed in the hospital and when reduction in beta-hCG titles was observed, the patients were discharged from the hospital and followed in the outpatient department, with weekly determinations of beta-hCG until levels lower than 5 mIU/ml were reached, that were considered successful. Results: of the 70 patients who underwent expectant management, only one needed a surgical intervention, because of tubal rupture. The initial values of beta-hCG of the patients ranged from 27 mIU/ml to 41,000 mIU/ml. The average diameter of the tubal mass was 2.9 cm. The presence of free liquid in the peritoneal cavity was observed in 50 patients, small amount in 26 patients, moderate in 16 and large in 8 patients. The ultrasonographic resolution of hematosalpinx occurred in 58 patients and tubal ring was visualized in 12 patients. On color Doppler, 52 were at low risk and 18 at medium risk. Conclusions: the expectant management should be applied with safety in the cases that respect the inclusion criteria, the index of success of this study being 98.6%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(8):465-470
DOI 10.1590/S0100-72031999000800007
SUMMARY Objective: to evaluate the inclusion parameters in the selection of cases of (tubal) ectopic pregnancy for expectant management and to assess the results. Methods: a prospective study was carried out in 70 patients with unruptured (tubal) ectopic pregnancy, with the objective to carry out an expectant management. The main inclusion criteria in this study were the diameter of the tubal mass, that should be equal or inferior to 5,0 cm, reduced titles of beta-hCG (beta fraction of the chorionic gonadotropic hormone) as compared to the initial value within an interval of 48 h, hemodynamic stability, wishes for future pregnancy and a written permission to participate in the study. All patients were observed in the hospital and when reduction in beta-hCG titles was observed, the patients were discharged from the hospital and followed in the outpatient department, with weekly determinations of beta-hCG until levels lower than 5 mIU/ml were reached, that were considered successful. Results: of the 70 patients who underwent expectant management, only one needed a surgical intervention, because of tubal rupture. The initial values of beta-hCG of the patients ranged from 27 mIU/ml to 41,000 mIU/ml. The average diameter of the tubal mass was 2.9 cm. The presence of free liquid in the peritoneal cavity was observed in 50 patients, small amount in 26 patients, moderate in 16 and large in 8 patients. The ultrasonographic resolution of hematosalpinx occurred in 58 patients and tubal ring was visualized in 12 patients. On color Doppler, 52 were at low risk and 18 at medium risk. Conclusions: the expectant management should be applied with safety in the cases that respect the inclusion criteria, the index of success of this study being 98.6%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(9):465-469
DOI 10.1590/S0100-72032007000900005
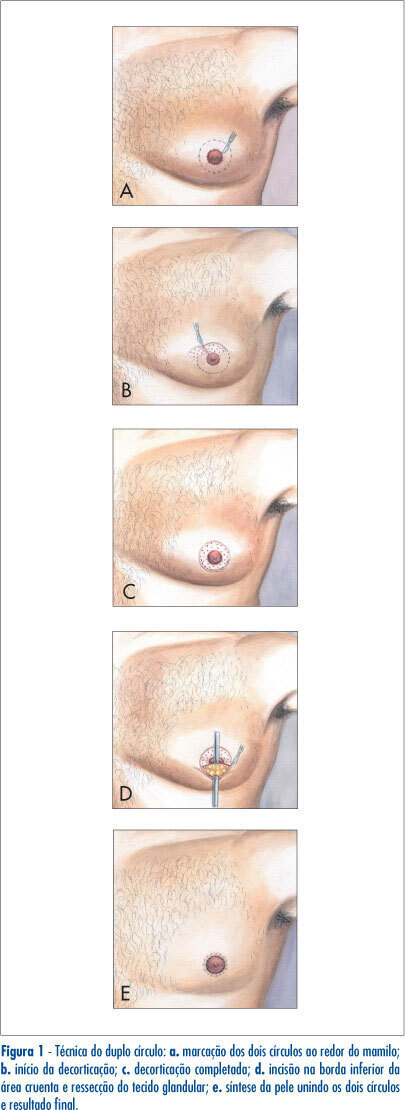
PURPOSE: to compare the double-circle (DC) technique to other techniques, with periareolar (PA) and transverse nipple-areolar (TNA) incisions, for the surgical correction of gynecomastia. METHODS: we studied the medical files of 34 patients from the Federal University of Goiás, submitted to the surgical correction of gynecomastia, from 1999 to 2004. Patients were divided according to the surgical technique used. The parametric numeric variables were compared by Tukey test. The chi2 or the Fisher's exact test was used for nominal variables. It was considered significant a p value<0.05. RESULTS: the mean age of the patients was 27.9 (+12.5) years. There were 43 gynecomastias, 34 unilateral (79.1%) and nine (20.9%) bilateral. There were 19 breasts operated (44.2%) using DC, 14 (33.6%) using PA incision, and 10 (23.3%), TNA incision. The mean drain usage was five days for DC and one day for the others (p<0.01). The suction drain was used in 19 cases (100%) of DC and two (22%) in TNA. The other patients used drains of Penrose (p<0.01). The mean surgical time was significantly larger for DC (73 minutes) than for PA (45 minutes) and for TNA (48 minutes). DC was used mainly in voluminous gynecomastias (p=0.04). The complications consisted in three (33%) hematomas in TNA (p<0.01) and one (5%) in DC; one (11%) infection in TNA; two (10%) partial necrosis of the nipple in DC; four (21%) enlarged scars in DC (p=0.04); three (16%) hypertrofic scars (p=0.08) in DC; one (2%) inversion of nipple with TNA. CONCLUSIONS: The DC was used often in voluminous gynecomastias. It was a good and secure operation, although it required a more extensive surgical time and had a larger possibility of distended scars.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(9):465-469
DOI 10.1590/S0100-72032007000900005
PURPOSE: to compare the double-circle (DC) technique to other techniques, with periareolar (PA) and transverse nipple-areolar (TNA) incisions, for the surgical correction of gynecomastia. METHODS: we studied the medical files of 34 patients from the Federal University of Goiás, submitted to the surgical correction of gynecomastia, from 1999 to 2004. Patients were divided according to the surgical technique used. The parametric numeric variables were compared by Tukey test. The chi2 or the Fisher's exact test was used for nominal variables. It was considered significant a p value<0.05. RESULTS: the mean age of the patients was 27.9 (+12.5) years. There were 43 gynecomastias, 34 unilateral (79.1%) and nine (20.9%) bilateral. There were 19 breasts operated (44.2%) using DC, 14 (33.6%) using PA incision, and 10 (23.3%), TNA incision. The mean drain usage was five days for DC and one day for the others (p<0.01). The suction drain was used in 19 cases (100%) of DC and two (22%) in TNA. The other patients used drains of Penrose (p<0.01). The mean surgical time was significantly larger for DC (73 minutes) than for PA (45 minutes) and for TNA (48 minutes). DC was used mainly in voluminous gynecomastias (p=0.04). The complications consisted in three (33%) hematomas in TNA (p<0.01) and one (5%) in DC; one (11%) infection in TNA; two (10%) partial necrosis of the nipple in DC; four (21%) enlarged scars in DC (p=0.04); three (16%) hypertrofic scars (p=0.08) in DC; one (2%) inversion of nipple with TNA. CONCLUSIONS: The DC was used often in voluminous gynecomastias. It was a good and secure operation, although it required a more extensive surgical time and had a larger possibility of distended scars.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(7):465-471
DOI 10.1590/S0100-72032003000700002
PURPOSE: to investigate the effect of antiretroviral drugs on carbohydrate metabolism in HIV-infected pregnant women and on fetal and neonatal prognosis. METHODS: a prospective study was conducted on 57 pregnant women. The women were divided into three groups: ZDV group, taking zidovudine (n=20), TT group, taking zidovudine + lamivudine + nelfinavir (n=25), and control group (n=12). Blood samples were obtained for the determination of the area under the curve (AUC) after a 75-g oral glucose test at four periods during pregnancy (1st=14-20 weeks, 2nd= 21-26 weeks, 3rd=27-32 weeks and 4th=33-38 weeks). Perinatal prognosis was based on prematurity rates, intrauterine growth restriction (IUGR), low birth weight, perinatal mortality, and vertical HIV-1 transmission. Data were analyzed statistically using the nonparametric c² test, Friedman test and Kruskal-Wallis test. RESULTS: the median values of the AUC were 11.685 mg/dL for the control group, 13.477 mg/dL for the ZDV Group, and 13.650 mg/dL for the TT group (p=0.049). The antiretroviral agents had no deleterious effects on prematurity, low birth weight, IUGR rates or on Apgar score. There was no case of vertical transmission of HIV-1. CONCLUSIONS: an association was detected between the use of triple therapy and the development of carbohydrate intolerance during pregnancy. This association was not shown with ZDV alone. The antiretroviral agents had no deleterious effects on perinatal prognosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(7):465-471
DOI 10.1590/S0100-72032003000700002
PURPOSE: to investigate the effect of antiretroviral drugs on carbohydrate metabolism in HIV-infected pregnant women and on fetal and neonatal prognosis. METHODS: a prospective study was conducted on 57 pregnant women. The women were divided into three groups: ZDV group, taking zidovudine (n=20), TT group, taking zidovudine + lamivudine + nelfinavir (n=25), and control group (n=12). Blood samples were obtained for the determination of the area under the curve (AUC) after a 75-g oral glucose test at four periods during pregnancy (1st=14-20 weeks, 2nd= 21-26 weeks, 3rd=27-32 weeks and 4th=33-38 weeks). Perinatal prognosis was based on prematurity rates, intrauterine growth restriction (IUGR), low birth weight, perinatal mortality, and vertical HIV-1 transmission. Data were analyzed statistically using the nonparametric c² test, Friedman test and Kruskal-Wallis test. RESULTS: the median values of the AUC were 11.685 mg/dL for the control group, 13.477 mg/dL for the ZDV Group, and 13.650 mg/dL for the TT group (p=0.049). The antiretroviral agents had no deleterious effects on prematurity, low birth weight, IUGR rates or on Apgar score. There was no case of vertical transmission of HIV-1. CONCLUSIONS: an association was detected between the use of triple therapy and the development of carbohydrate intolerance during pregnancy. This association was not shown with ZDV alone. The antiretroviral agents had no deleterious effects on perinatal prognosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(8):465-473
To analyze the effect of combined training (CT) in postural control and gait parameters in postmenopausal women.
A parallel-group, randomized, control study was conducted with 16 weeks of combined training (n = 16) versus a non-training control group (n = 12) in postmenopausal women (aged 59.3 ± 8.0). Pre and postintervention assessments included postural control (using an AMTI force platform – Advanced Mechanical Technology, Inc., Watertown, MA, USA) and gait impairments (using baropodometry). In addition, the upper limb strength and abdominal tests, as well as aerobic capacity, assessed functional indicators.
The CT intervention in postmenopausal women resulted in improved gait (stride length (p = 0.006); speed (p = 0.013); double support time (p = 0.045); and improved postural control (displacement area of postural sway in a normal base of support with eyes open (p = 0.006). Combined training increased functional indicators (abdominal - p = 0.031; aerobic capacity - p = 0.002).
In conclusion, combined aerobic plus strength training effectively improved gait and balance control in older women. The postmenopausal women from the CT group walked faster and with bigger steps after the intervention than the control group. In addition, they presented decreased postural sway in standing and decreased the percentage of double support time while walking, which means improved static and dynamic balance control and functional indicators.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(8):465-473
To analyze the effect of combined training (CT) in postural control and gait parameters in postmenopausal women.
A parallel-group, randomized, control study was conducted with 16 weeks of combined training (n = 16) versus a non-training control group (n = 12) in postmenopausal women (aged 59.3 ± 8.0). Pre and postintervention assessments included postural control (using an AMTI force platform – Advanced Mechanical Technology, Inc., Watertown, MA, USA) and gait impairments (using baropodometry). In addition, the upper limb strength and abdominal tests, as well as aerobic capacity, assessed functional indicators.
The CT intervention in postmenopausal women resulted in improved gait (stride length (p = 0.006); speed (p = 0.013); double support time (p = 0.045); and improved postural control (displacement area of postural sway in a normal base of support with eyes open (p = 0.006). Combined training increased functional indicators (abdominal - p = 0.031; aerobic capacity - p = 0.002).
In conclusion, combined aerobic plus strength training effectively improved gait and balance control in older women. The postmenopausal women from the CT group walked faster and with bigger steps after the intervention than the control group. In addition, they presented decreased postural sway in standing and decreased the percentage of double support time while walking, which means improved static and dynamic balance control and functional indicators.