Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(9):459-464
DOI 10.1590/S0100-72032007000900004
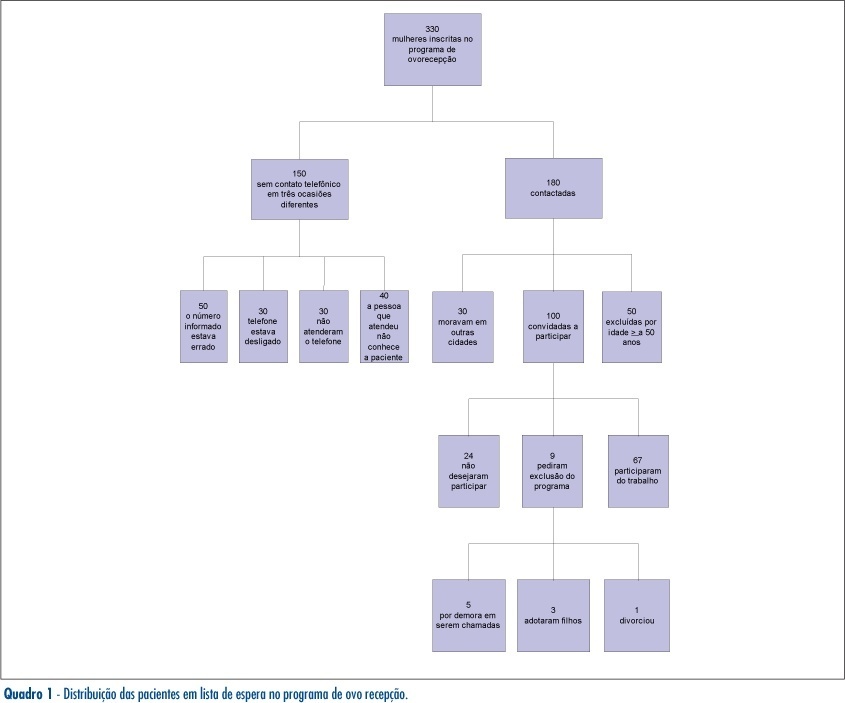
PURPOSE: describe epidemiologic profile of patients enrolled in the oocyte reception program at Hospital Regional da Asa Sul (HRAS) in Brasília, Distrito Federal, Brazil, and its main indications. METHODS: prospective descriptive study, in which 330 patients enrolled in the waiting list program were studied. Sixty-seven women, irrespective of their infertility factor and that had not been contemplated by the treatment were included. Thirty women who lived in other cities, 50 patients over 50 years old, 24 patients that didn't want to take part in the study, nine patients that asked to be left out of the program and 150 women that couldn't be found by phone calls were excluded. The 67 patients included were interviewed in order to answer a questionnaire. Their medical handbook was recovered to confirm that the investigation required to establish the cause of infertility had been done. The data was registered and analyzed by SPSS version 12.0 software. RESULTS: the patients' epidemiologic profile is age range 40 to 49 years old (82%), non-white skinned (77,6%), catholic (71,6%), married (59,7%), in high school (76,1%), secondary infertility (53,6%) from which due to tubal sterilization (40,3%) and those ones who started trying to conceive before 35 years old (91%). The main indication to enroll in this oocyte reception program was age and low ovarian reserve. CONCLUSION: the results demonstrated the indiscriminate tubal sterilization. The oocyte reception program benefits women with reserved reproductive prognostic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(9):459-464
DOI 10.1590/S0100-72032007000900004
PURPOSE: describe epidemiologic profile of patients enrolled in the oocyte reception program at Hospital Regional da Asa Sul (HRAS) in Brasília, Distrito Federal, Brazil, and its main indications. METHODS: prospective descriptive study, in which 330 patients enrolled in the waiting list program were studied. Sixty-seven women, irrespective of their infertility factor and that had not been contemplated by the treatment were included. Thirty women who lived in other cities, 50 patients over 50 years old, 24 patients that didn't want to take part in the study, nine patients that asked to be left out of the program and 150 women that couldn't be found by phone calls were excluded. The 67 patients included were interviewed in order to answer a questionnaire. Their medical handbook was recovered to confirm that the investigation required to establish the cause of infertility had been done. The data was registered and analyzed by SPSS version 12.0 software. RESULTS: the patients' epidemiologic profile is age range 40 to 49 years old (82%), non-white skinned (77,6%), catholic (71,6%), married (59,7%), in high school (76,1%), secondary infertility (53,6%) from which due to tubal sterilization (40,3%) and those ones who started trying to conceive before 35 years old (91%). The main indication to enroll in this oocyte reception program was age and low ovarian reserve. CONCLUSION: the results demonstrated the indiscriminate tubal sterilization. The oocyte reception program benefits women with reserved reproductive prognostic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(9):459-468
DOI 10.1590/S0100-72032010000900008
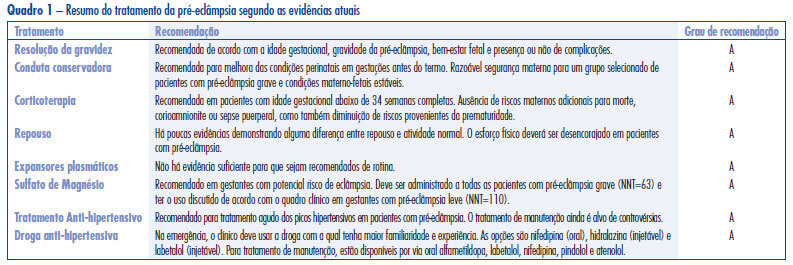
Hypertensive disorders in pregnancy deserve special attention in the setting of global public health. Currently, they represent the third cause of maternal mortality in the world and first in Brazil. From a practical standpoint, pre-eclampsia remains a syndrome that leads to serious repercussions on maternal and fetal mortality and its etiology is not well known. Currently, the best treatment for forms of pre-eclampsia is being discussed at different times in pregnancy and puerperium, with the objective to reduce the high rates of maternal and fetal morbidity and mortality. Considering the pathophysiology of the event, anticipation of delivery is the best treatment for pre-eclampsia. The use of magnesium sulfate is recommended in all cases of severe pre-eclampsia and eclampsia for prevention and treatment of seizures. Likewise, treatment of hypertensive crises is recommended. Hydralazine, nifedipine and labetalol have been the most commonly used drugs for this purpose, but their use depends on the familiarity of the treating physician. Antenatal corticoid therapy is indicated whenever there is an imminent risk of preterm delivery between 24 and 34 weeks. In contrast, there is insufficient evidence to recommend bed rest and routine plasma volume expansion, and there is an urgent need for randomized clinical trials to determine whether maintenance antihypertensive treatment in pregnant women has benefits or risks for mothers and fetuses in all clinical forms of disease, particularly in cases of pure pre-eclampsia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(9):459-468
DOI 10.1590/S0100-72032010000900008
Hypertensive disorders in pregnancy deserve special attention in the setting of global public health. Currently, they represent the third cause of maternal mortality in the world and first in Brazil. From a practical standpoint, pre-eclampsia remains a syndrome that leads to serious repercussions on maternal and fetal mortality and its etiology is not well known. Currently, the best treatment for forms of pre-eclampsia is being discussed at different times in pregnancy and puerperium, with the objective to reduce the high rates of maternal and fetal morbidity and mortality. Considering the pathophysiology of the event, anticipation of delivery is the best treatment for pre-eclampsia. The use of magnesium sulfate is recommended in all cases of severe pre-eclampsia and eclampsia for prevention and treatment of seizures. Likewise, treatment of hypertensive crises is recommended. Hydralazine, nifedipine and labetalol have been the most commonly used drugs for this purpose, but their use depends on the familiarity of the treating physician. Antenatal corticoid therapy is indicated whenever there is an imminent risk of preterm delivery between 24 and 34 weeks. In contrast, there is insufficient evidence to recommend bed rest and routine plasma volume expansion, and there is an urgent need for randomized clinical trials to determine whether maintenance antihypertensive treatment in pregnant women has benefits or risks for mothers and fetuses in all clinical forms of disease, particularly in cases of pure pre-eclampsia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):459-459
DOI 10.1590/S0100-72032000000700010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):459-459
DOI 10.1590/S0100-72032000000700010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):459-459
DOI 10.1590/S0100-72032000000700011
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):459-459
DOI 10.1590/S0100-72032000000700011
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):46-53
Magnetic resonance imaging (MRI) has been considered another tool for use during the pre- and postoperative periods of the management of pelvic-organ prolapse (POP). However, there is little consensus regarding its practical use for POP and the association betweenMRI lines of reference and physical examination.We aimedto evaluate the mid- to long-term results of two surgical techniques for apical prolapse.
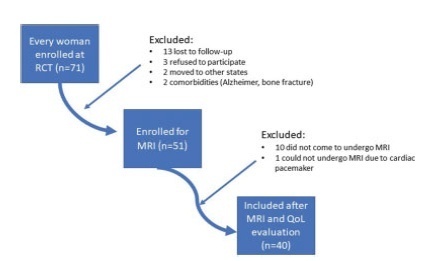
In total, 40 women with apical POP randomized from 2014 to 2016 underwent abdominal sacrocolpopexy (ASC group; n = 20) or bilateral vaginal sacrospinous fixation with an anterior mesh (VSF-AM group; n = 20). A physical examination using the POP Quantification System (POP-Q) for staging (objective cure) and the International Consultation on Incontinence Questionnaire-Vaginal Symptoms (ICIQ-VS: subjective cure), were applied and analyzed before and one year after surgery respectively. All MRI variables (pubococcigeous line [PCL], bladder base [BB], anorectal junction [ARJ], and the estimated levator ani subtended volume [eLASV]) were investigated one year after surgery. Significance was established at p < 0.05.
After a mean 27-month follow-up, according to the MRI criteria, 60% of the women were cured in the VSF-AM group versus 45% in ASC group (p= 0.52). The POP-Q and objective cure rates by MRI were correlated in the anterior vaginal wall (p= 0.007), but no correlationwas foundwith the subjective cure. The eLASVwas largeramongthe patients with surgical failure, and a cutoff of ≥ 33.5mm3 was associated with postoperative failure (area under the receiver operating characteristic curve [ROC]: 0.813; p= 0.002).
Both surgeries for prolapse were similar regarding theobjective variables (POP-Q measurements and MRI cure rates). Larger eLASV areas were associated with surgical failure.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):46-53
Magnetic resonance imaging (MRI) has been considered another tool for use during the pre- and postoperative periods of the management of pelvic-organ prolapse (POP). However, there is little consensus regarding its practical use for POP and the association betweenMRI lines of reference and physical examination.We aimedto evaluate the mid- to long-term results of two surgical techniques for apical prolapse.
In total, 40 women with apical POP randomized from 2014 to 2016 underwent abdominal sacrocolpopexy (ASC group; n = 20) or bilateral vaginal sacrospinous fixation with an anterior mesh (VSF-AM group; n = 20). A physical examination using the POP Quantification System (POP-Q) for staging (objective cure) and the International Consultation on Incontinence Questionnaire-Vaginal Symptoms (ICIQ-VS: subjective cure), were applied and analyzed before and one year after surgery respectively. All MRI variables (pubococcigeous line [PCL], bladder base [BB], anorectal junction [ARJ], and the estimated levator ani subtended volume [eLASV]) were investigated one year after surgery. Significance was established at p < 0.05.
After a mean 27-month follow-up, according to the MRI criteria, 60% of the women were cured in the VSF-AM group versus 45% in ASC group (p= 0.52). The POP-Q and objective cure rates by MRI were correlated in the anterior vaginal wall (p= 0.007), but no correlationwas foundwith the subjective cure. The eLASVwas largeramongthe patients with surgical failure, and a cutoff of ≥ 33.5mm3 was associated with postoperative failure (area under the receiver operating characteristic curve [ROC]: 0.813; p= 0.002).
Both surgeries for prolapse were similar regarding theobjective variables (POP-Q measurements and MRI cure rates). Larger eLASV areas were associated with surgical failure.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):46-46
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):46-46
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):460-460
DOI 10.1590/S0100-72032000000700013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):460-460
DOI 10.1590/S0100-72032000000700013