Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(7):449-453
To analyze the effects of estrogen alone or in combination with progestogens and tibolone (TIB) on the expression of the extracellular matrix metalloproteinases 2 and 9 (MMP-2 and MMP-9), of perlecan, and of heparanase (HPSE) of the vascular walls of the carotid arteries.
A total of 30 250-day-old ovariectomized Wistar rats were orally treated for 5 weeks with: a) 1 mg/kg of estradiol benzoate (EB); b) EB + 0.2 mg/kg of medroxyprogesterone acetate (MPA); c) EB + 0.2mg/kg of norethisterone acetate (NETA); d) EB + 2 mg/kg of dydrogesterone (DI); e) 1 mg/kg of TIB; f) placebo (CTR). Following treatment, the expression of mRNA for MMP-2, MMP-9, and HPSE was analyzed by realtime polymerase chain-reaction (PCR), and the expression of MMP-2, of MMP-9, of tissue inhibitor of metalloproteinase 2 (TIMP-2), and of perlecan was quantified by immunohistochemistry in the carotid arteries.
The groups showed significant differences on mRNA HPSE expression (p = 0.048), which was higher in the EB, EB + MPA, and TIB groups. There was no statistically significant difference in mRNA MMP-2 or MMP-9 expression. The immunohistochemical expression of MMP-2, of TIMP-2, of MMP-9, of HPSE, and of perlecan showed no differences between groups.
Estradiol alone or associated with MPA and TIB treatment can increase mRNA HSPE expression of the walls of the carotid arteries in ovariectomized rats.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(7):449-453
To analyze the effects of estrogen alone or in combination with progestogens and tibolone (TIB) on the expression of the extracellular matrix metalloproteinases 2 and 9 (MMP-2 and MMP-9), of perlecan, and of heparanase (HPSE) of the vascular walls of the carotid arteries.
A total of 30 250-day-old ovariectomized Wistar rats were orally treated for 5 weeks with: a) 1 mg/kg of estradiol benzoate (EB); b) EB + 0.2 mg/kg of medroxyprogesterone acetate (MPA); c) EB + 0.2mg/kg of norethisterone acetate (NETA); d) EB + 2 mg/kg of dydrogesterone (DI); e) 1 mg/kg of TIB; f) placebo (CTR). Following treatment, the expression of mRNA for MMP-2, MMP-9, and HPSE was analyzed by realtime polymerase chain-reaction (PCR), and the expression of MMP-2, of MMP-9, of tissue inhibitor of metalloproteinase 2 (TIMP-2), and of perlecan was quantified by immunohistochemistry in the carotid arteries.
The groups showed significant differences on mRNA HPSE expression (p = 0.048), which was higher in the EB, EB + MPA, and TIB groups. There was no statistically significant difference in mRNA MMP-2 or MMP-9 expression. The immunohistochemical expression of MMP-2, of TIMP-2, of MMP-9, of HPSE, and of perlecan showed no differences between groups.
Estradiol alone or associated with MPA and TIB treatment can increase mRNA HSPE expression of the walls of the carotid arteries in ovariectomized rats.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):449-452
DOI 10.1590/S0100-72032003000600011
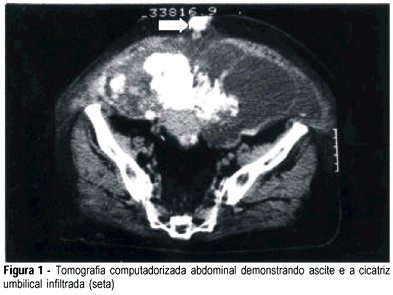
The umbilical metastatic tumoral nodule, Sister Mary Joseph's nodule, is a rare clinical sign indicative of disseminated intra-abdominal tumor, and may be the first evidence of malignancy. The authors report a case of a patient with umbilical metastatic nodule in whom the diagnosis of the primary tumor was possible by immunohistochemistry of the lesion biopsy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):449-452
DOI 10.1590/S0100-72032003000600011
The umbilical metastatic tumoral nodule, Sister Mary Joseph's nodule, is a rare clinical sign indicative of disseminated intra-abdominal tumor, and may be the first evidence of malignancy. The authors report a case of a patient with umbilical metastatic nodule in whom the diagnosis of the primary tumor was possible by immunohistochemistry of the lesion biopsy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(8):449-453
DOI 10.1590/S0100-72031998000800004
Purpose: to determine folate, vitamin B12 and ferritin levels in patients whose fetuses presented neural-tube defects (NTD). Blood folate and vitamin B12 act as cofactors of enzymes involved in DNA biosynthesis. Interruption of this process may block neural-tube closing. Vitamin supplementation with folate may reduce occurrence rates and recurrence of NTD, although there is concern about the fact that this prevention may mask vitamin B12 deficiency. Methods: vitamin B12 and ferritin determinations by enzyme immunoassay with microparticles and folic acid determination using the ion capture method (IMx ABBOTT). Results: the percentage of pregnant women with vitamin B12 deficirncy (serum levels < 150 pg/ml) was 11.8%. There was no case of folate deficiency (serum levels < 3.0 ng/ml) and prevalence of pregnant women with iron store deficiency was 47.1% (serum levels < ng/mg). Conclusions: occording to the results obtained in this study (prevalence of 11.8% of vitamin B12 and 0% of folate deficient pregnant women) we suggest that supplementation should be administered after serum vitamin B12 determination.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(8):449-453
DOI 10.1590/S0100-72031998000800004
Purpose: to determine folate, vitamin B12 and ferritin levels in patients whose fetuses presented neural-tube defects (NTD). Blood folate and vitamin B12 act as cofactors of enzymes involved in DNA biosynthesis. Interruption of this process may block neural-tube closing. Vitamin supplementation with folate may reduce occurrence rates and recurrence of NTD, although there is concern about the fact that this prevention may mask vitamin B12 deficiency. Methods: vitamin B12 and ferritin determinations by enzyme immunoassay with microparticles and folic acid determination using the ion capture method (IMx ABBOTT). Results: the percentage of pregnant women with vitamin B12 deficirncy (serum levels < 150 pg/ml) was 11.8%. There was no case of folate deficiency (serum levels < 3.0 ng/ml) and prevalence of pregnant women with iron store deficiency was 47.1% (serum levels < ng/mg). Conclusions: occording to the results obtained in this study (prevalence of 11.8% of vitamin B12 and 0% of folate deficient pregnant women) we suggest that supplementation should be administered after serum vitamin B12 determination.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):449-454
DOI 10.1590/S0100-72032000000700008
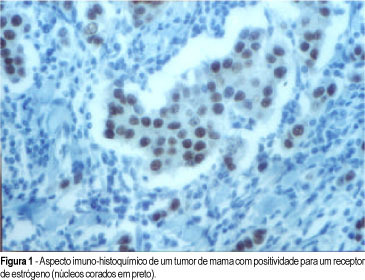
Purpose: to evaluate the prognostic value of estrogen receptor and p53 and c-erbB-2 proteins in lymph node-negative breast cancer. Methods: an immunohistochemical study was made in paraffin-embedded tissues from the file of the Instituto de Pesquisas Cito-Oncológicas of the Fundação Faculdade Federal de Ciências Médicas de Porto Alegre of fifty cases of postmenopausal women, who were treated at the Irmandade da Santa Casa de Misericórdia de Porto Alegre and at the Santa Rita Hospital from 1990 to 1994. For statistical analysis c² with Yates correction, as well as exact Fisher tests were used and Kaplan Meier curves compared with log-rank test. The mean follow-up of the patients was 3.6 years (3.1-4.5). Of the 50 cases, 14 showed recurrence during the period of follow-up. Results: the mean age was 61 years (46-78). Modified radical mastectomy was performed in 35 patients (70%) and 15 (30%) were submitted to lumpectomy/axillary dissection and postoperative radiation therapy. Fifty percent of the patients who showed recurrence did it in the first three years after the diagnosis. The mean size of the tumor was 2.8 cm (1.98-3.13) and the most frequent histological type was invasive ductal carcinoma of no special type (92%), according to the Bloom and Richardson graduation, 3 being stage I (6.6%), 35 stage II (76%) and 8 stage III (17.4%). In the tumors with recurrence, there was no grade I, 9 stage II (25.7%) and 3 stage III (37.5%). In relation to the prognosis, the disease-free interval was less when there was association of a poorly differentiated tumor with negative estrogen receptor (p = 0.006), positive p53 (p = 0.006) and positive c-erbB-2 (p = 0.001). Conclusion: postmenopausal women with lymph node-negative breast cancer showed worse prognosis in relation to disease-free interval when they presented poorly differentiated tumor associated with negative estrogen receptor, positive p53 and positive c-erbB-2.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):449-454
DOI 10.1590/S0100-72032000000700008
Purpose: to evaluate the prognostic value of estrogen receptor and p53 and c-erbB-2 proteins in lymph node-negative breast cancer. Methods: an immunohistochemical study was made in paraffin-embedded tissues from the file of the Instituto de Pesquisas Cito-Oncológicas of the Fundação Faculdade Federal de Ciências Médicas de Porto Alegre of fifty cases of postmenopausal women, who were treated at the Irmandade da Santa Casa de Misericórdia de Porto Alegre and at the Santa Rita Hospital from 1990 to 1994. For statistical analysis c² with Yates correction, as well as exact Fisher tests were used and Kaplan Meier curves compared with log-rank test. The mean follow-up of the patients was 3.6 years (3.1-4.5). Of the 50 cases, 14 showed recurrence during the period of follow-up. Results: the mean age was 61 years (46-78). Modified radical mastectomy was performed in 35 patients (70%) and 15 (30%) were submitted to lumpectomy/axillary dissection and postoperative radiation therapy. Fifty percent of the patients who showed recurrence did it in the first three years after the diagnosis. The mean size of the tumor was 2.8 cm (1.98-3.13) and the most frequent histological type was invasive ductal carcinoma of no special type (92%), according to the Bloom and Richardson graduation, 3 being stage I (6.6%), 35 stage II (76%) and 8 stage III (17.4%). In the tumors with recurrence, there was no grade I, 9 stage II (25.7%) and 3 stage III (37.5%). In relation to the prognosis, the disease-free interval was less when there was association of a poorly differentiated tumor with negative estrogen receptor (p = 0.006), positive p53 (p = 0.006) and positive c-erbB-2 (p = 0.001). Conclusion: postmenopausal women with lymph node-negative breast cancer showed worse prognosis in relation to disease-free interval when they presented poorly differentiated tumor associated with negative estrogen receptor, positive p53 and positive c-erbB-2.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(10):449-455
DOI 10.1590/SO100-720320140004946
To assess cardiometabolic risk factors during normal pregnancy and the influence of maternal obesity on them.
This study included 25 healthy pregnant women with a single pregnancy and a gestational age of less than twenty weeks. Longitudinal analysis of blood pressure, body weight, body mass index (BMI), serum concentrations of leptin, adiponectin, cortisol, total cholesterol and fractions, triglycerides, uric acid, fasting glucose, oral glucose tolerance test, HOMA-IR and insulin/glucose ratio was performed each trimester during pregnancy. In order to evaluate the impact of obesity, pregnant women were divided into two groups based on BMI for the first quarter of pregnancy: Gpn for pregnant women with BMI<25 kg/m2 and Gso for BMI≥25 kg/m2. One-Way ANOVA for repeated measurements or Friedman test and Student-t or Mann-Whitney tests for statistical comparisons and Pearson correlations test were used for statistical analysis.
The mean values for the first quarter of pregnancy for the following parameters were: age: 22 years; weight: 66.3 kg and BMI 26.4 kg/m2, with 20.2 and 30.7 kg/m2 for the Gpn and Gso groups, respectively. Mean weight gain during pregnancy was ±12.7 kg with 10.3 kg for the Gso group and 15.2 kg for the Gpn group. Regarding plasma determinations, cortisol, uric acid and lipid profile increased during all trimesters of pregnancy, except for HDL-cholesterol, which did not change. Blood pressure, insulin and HOMA-IR only increased in the third quarter of pregnancy. The Gso group tended to gain more weight and to show higher concentrations of leptin, total cholesterol, LDL-cholesterol, VLDL-cholesterol, TG, glucose, insulin, HOMA-IR, besides lower HDL-cholesterol and greater diastolic blood pressure in the 3rdquarter of pregnancy. Three pregnant women developed gestational hypertension, presented prepregnancy obesity, excessive weight gain, hyperleptinemia and an insulin/glucose ratio greater than two. Weight and BMI were positively correlated with total cholesterol and its LDL fraction, TG, uric acid, fasting blood glucose, insulin and HOMA-IR; and were negatively correlated with adiponectin and HDL-cholesterol. Leptin level was positively correlated with blood pressure.
The metabolic changes in pregnancy are more significant in obese women, suggesting, as expected, an increased risk of cardiometabolic complications. During their first visit for prenatal care, obese women should be informed about these risks, have their BMI and insulin/glucose ratio calculated along with their lipid profile to identify pregnant women at higher risk for cardiovascular diseases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(10):449-455
DOI 10.1590/SO100-720320140004946
To assess cardiometabolic risk factors during normal pregnancy and the influence of maternal obesity on them.
This study included 25 healthy pregnant women with a single pregnancy and a gestational age of less than twenty weeks. Longitudinal analysis of blood pressure, body weight, body mass index (BMI), serum concentrations of leptin, adiponectin, cortisol, total cholesterol and fractions, triglycerides, uric acid, fasting glucose, oral glucose tolerance test, HOMA-IR and insulin/glucose ratio was performed each trimester during pregnancy. In order to evaluate the impact of obesity, pregnant women were divided into two groups based on BMI for the first quarter of pregnancy: Gpn for pregnant women with BMI<25 kg/m2 and Gso for BMI≥25 kg/m2. One-Way ANOVA for repeated measurements or Friedman test and Student-t or Mann-Whitney tests for statistical comparisons and Pearson correlations test were used for statistical analysis.
The mean values for the first quarter of pregnancy for the following parameters were: age: 22 years; weight: 66.3 kg and BMI 26.4 kg/m2, with 20.2 and 30.7 kg/m2 for the Gpn and Gso groups, respectively. Mean weight gain during pregnancy was ±12.7 kg with 10.3 kg for the Gso group and 15.2 kg for the Gpn group. Regarding plasma determinations, cortisol, uric acid and lipid profile increased during all trimesters of pregnancy, except for HDL-cholesterol, which did not change. Blood pressure, insulin and HOMA-IR only increased in the third quarter of pregnancy. The Gso group tended to gain more weight and to show higher concentrations of leptin, total cholesterol, LDL-cholesterol, VLDL-cholesterol, TG, glucose, insulin, HOMA-IR, besides lower HDL-cholesterol and greater diastolic blood pressure in the 3rdquarter of pregnancy. Three pregnant women developed gestational hypertension, presented prepregnancy obesity, excessive weight gain, hyperleptinemia and an insulin/glucose ratio greater than two. Weight and BMI were positively correlated with total cholesterol and its LDL fraction, TG, uric acid, fasting blood glucose, insulin and HOMA-IR; and were negatively correlated with adiponectin and HDL-cholesterol. Leptin level was positively correlated with blood pressure.
The metabolic changes in pregnancy are more significant in obese women, suggesting, as expected, an increased risk of cardiometabolic complications. During their first visit for prenatal care, obese women should be informed about these risks, have their BMI and insulin/glucose ratio calculated along with their lipid profile to identify pregnant women at higher risk for cardiovascular diseases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(5):449-451
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(5):449-451
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(6):449-454
DOI 10.1590/S0100-72032004000600005
OBJECTIVE: to study the effect of a single contraceptive implant of nomegestrol acetate (Uniplant) on the ovarian function, cervical mucus production and sperm penetration, when inserted in women in the preovulatory phase. METHODS: twenty women with regular menstrual cycles were included in an open comparative study. All participants were investigated during one menstrual cycle before (control) and one menstrual cycle after implant insertion. Measurements of estradiol, LH, and progesterone, as well as transvaginal sonography, cervical mucus examination and sperm penetration test, were carried out. Statistical analysis was performed with the paired t-test and the non-parametric test of Wilcoxon. RESULTS: all control cycles were ovulatory and presented normal parameters. Preovulatory estradiol and LH peak decreased significantly from 603.2 ± 78.0 pmo/l and 22.5 ± 6.5 IU/l at pre-insertion to 380.7 ± 51.9 pmol/l and 4.9 ± 1.3 IU/l 48 hours after implant insertion (p < 0.05 and p < 0.01, respectively). Progesterone levels did not vary significantly (control cycle = 49.8 ± 3.3 nmol/l and treated cycle = 43.2 ± 5.2 nmol/l). Cervical mucus and sperm penetration tests were profoundly affected in 10.5% of the users 20 h after implant insertion, in 68.5% after 24 h and in 100% after 48 h. Follicular rupture occurred in the majority of the cycles 48 h after implant insertion. CONCLUSIONS: the use of a single implant of nomegestrol acetate affected estradiol and LH preovulatory peaks and disrupted the process of cervical mucus production and sperm penetration, but it was unable to prevent ovulation when inserted at the preovulatory phase, which reinforces the need to insert the implant during the first five days of the menstrual cycle.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(6):449-454
DOI 10.1590/S0100-72032004000600005
OBJECTIVE: to study the effect of a single contraceptive implant of nomegestrol acetate (Uniplant) on the ovarian function, cervical mucus production and sperm penetration, when inserted in women in the preovulatory phase. METHODS: twenty women with regular menstrual cycles were included in an open comparative study. All participants were investigated during one menstrual cycle before (control) and one menstrual cycle after implant insertion. Measurements of estradiol, LH, and progesterone, as well as transvaginal sonography, cervical mucus examination and sperm penetration test, were carried out. Statistical analysis was performed with the paired t-test and the non-parametric test of Wilcoxon. RESULTS: all control cycles were ovulatory and presented normal parameters. Preovulatory estradiol and LH peak decreased significantly from 603.2 ± 78.0 pmo/l and 22.5 ± 6.5 IU/l at pre-insertion to 380.7 ± 51.9 pmol/l and 4.9 ± 1.3 IU/l 48 hours after implant insertion (p < 0.05 and p < 0.01, respectively). Progesterone levels did not vary significantly (control cycle = 49.8 ± 3.3 nmol/l and treated cycle = 43.2 ± 5.2 nmol/l). Cervical mucus and sperm penetration tests were profoundly affected in 10.5% of the users 20 h after implant insertion, in 68.5% after 24 h and in 100% after 48 h. Follicular rupture occurred in the majority of the cycles 48 h after implant insertion. CONCLUSIONS: the use of a single implant of nomegestrol acetate affected estradiol and LH preovulatory peaks and disrupted the process of cervical mucus production and sperm penetration, but it was unable to prevent ovulation when inserted at the preovulatory phase, which reinforces the need to insert the implant during the first five days of the menstrual cycle.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(2):45-48
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(2):45-48