Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(7):423-423
DOI 10.1590/S0100-72031999000700012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(7):423-424
DOI 10.1590/S0100-72031998000700010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(7):423-424
DOI 10.1590/S0100-72031998000700010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(7):423-423
DOI 10.1590/S0100-72031998000700009
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(7):423-423
DOI 10.1590/S0100-72031998000700009
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(8):423-427
DOI 10.1590/S0100-72032007000800007
PURPOSE: to identify the incidence and associated factors of surgical scar endometriosis. METHODS: a retrospective cohort observational study performed from the medical records of female patients attended at the Clinical Hospital of Univesidade Federal de Minas Gerais (UFMG) with histopathological diagnosis of scar endometriosis from May 1978 to December 2003. RESULTS: a total of 72 patients were included in the study. The incidence of scar endometriosis after cesarean section was significantly higher than after episiotomy (0.2% and 0.06%, respectively; p<0.00001) with relative risk of 3.3. The women’s age, when diagnosed, ranged from 16 to 48 years old, (mean=30.8 years old). The scar location varied according to the previous surgery: 46 scars after cesarean sections, one after hysterectomy and one after abdominal surgery (48 lesions in the abdominal wall); 19 scars after episiotomy, one because of relapse and two after pelvic floor surgeries (22 pelvic wounds); two women had not been submitted to previous gynecological surgery (one umbilical endometrioma and one lesion in the posterior vaginal wall). Pain was the most frequent symptom (80%), followed by a node (79%) and, in more than 40%, the pain and the node suffered modification with menstruation. Other less frequent complaints were: dyspareunia, secondary infertility, pelvic pain, dysmenorrhoea, scar secretion, menorrhagia pain when evacuating. The mean time observed between the surgery and the beginning of the symptoms was of 3.7 years. The average size of the endometriomas was 3.07 cm. The diagnosis based on clinic evaluation was correct in 71% of the cases. The choice of treatment in all the cases was the surgical excision. In only one incident there was relapse and new intervention. CONCLUSIONS: scar endometriosis is a rare situation originated, in most cases, after obstetrical surgical procedure, with higher risk after cesarean section. It is a highly suggestive clinical condition, with a rare necessity of complementary diagnostic procedures, and the best treatment choice is the surgical excision.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(8):423-427
DOI 10.1590/S0100-72032007000800007
PURPOSE: to identify the incidence and associated factors of surgical scar endometriosis. METHODS: a retrospective cohort observational study performed from the medical records of female patients attended at the Clinical Hospital of Univesidade Federal de Minas Gerais (UFMG) with histopathological diagnosis of scar endometriosis from May 1978 to December 2003. RESULTS: a total of 72 patients were included in the study. The incidence of scar endometriosis after cesarean section was significantly higher than after episiotomy (0.2% and 0.06%, respectively; p<0.00001) with relative risk of 3.3. The women’s age, when diagnosed, ranged from 16 to 48 years old, (mean=30.8 years old). The scar location varied according to the previous surgery: 46 scars after cesarean sections, one after hysterectomy and one after abdominal surgery (48 lesions in the abdominal wall); 19 scars after episiotomy, one because of relapse and two after pelvic floor surgeries (22 pelvic wounds); two women had not been submitted to previous gynecological surgery (one umbilical endometrioma and one lesion in the posterior vaginal wall). Pain was the most frequent symptom (80%), followed by a node (79%) and, in more than 40%, the pain and the node suffered modification with menstruation. Other less frequent complaints were: dyspareunia, secondary infertility, pelvic pain, dysmenorrhoea, scar secretion, menorrhagia pain when evacuating. The mean time observed between the surgery and the beginning of the symptoms was of 3.7 years. The average size of the endometriomas was 3.07 cm. The diagnosis based on clinic evaluation was correct in 71% of the cases. The choice of treatment in all the cases was the surgical excision. In only one incident there was relapse and new intervention. CONCLUSIONS: scar endometriosis is a rare situation originated, in most cases, after obstetrical surgical procedure, with higher risk after cesarean section. It is a highly suggestive clinical condition, with a rare necessity of complementary diagnostic procedures, and the best treatment choice is the surgical excision.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):423-424
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):423-424
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):423-424
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(9):423-431
DOI 10.1590/SO100-720320140005030
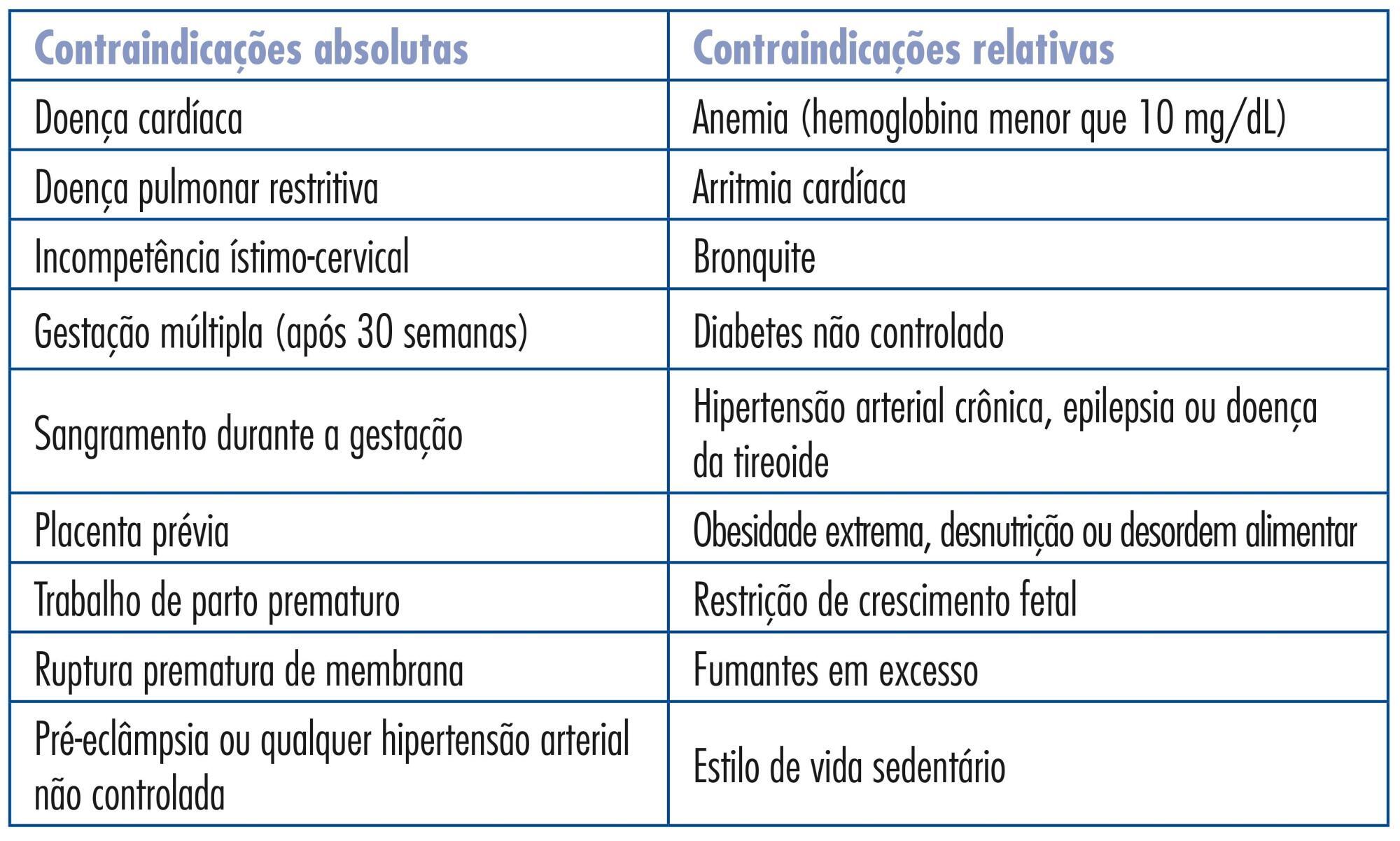
Physical exercise is recommended for all healthy pregnant women. Regular practice of exercises during pregnancy can provide many physical and psychological benefits, with no evidence of adverse outcomes for the fetus or the newborn when exercise is performed at mild to moderate intensity. However, few pregnant women engage in this practice and many still have fears and doubts about the safety of exercise. The objective of the present study was to inform the professionals who provide care for Brazilian pregnant women about the current recommendations regarding physical exercise during pregnancy based on the best scientific evidence available. In view of the perception that few systematic models are available about this topic and after performing several studies in this specific area, we assembled practical information of interest to both the professionals and the pregnant women. We also provide recommendations about the indications, contraindications, modalities (aerobics, resistance training, stretching and pelvic floor training), frequency, intensity and duration indicated for each gestational trimester. The review addresses physical exercise recommendation both for low risk pregnant women and for special populations, such as athletes and obese, hypertensive and diabetic subjects. The advantages of an active and healthy lifestyle should be always reinforced during and after gestation since pregnancy is an appropriate period to introduce new habits because pregnant women are usually more motivated to adhere to recommendations. Thus, routine exams, frequent returns and supervision are recommended in order to provide new guidelines that will have long-term beneficial effects for both mother and child.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(9):423-431
DOI 10.1590/SO100-720320140005030
Physical exercise is recommended for all healthy pregnant women. Regular practice of exercises during pregnancy can provide many physical and psychological benefits, with no evidence of adverse outcomes for the fetus or the newborn when exercise is performed at mild to moderate intensity. However, few pregnant women engage in this practice and many still have fears and doubts about the safety of exercise. The objective of the present study was to inform the professionals who provide care for Brazilian pregnant women about the current recommendations regarding physical exercise during pregnancy based on the best scientific evidence available. In view of the perception that few systematic models are available about this topic and after performing several studies in this specific area, we assembled practical information of interest to both the professionals and the pregnant women. We also provide recommendations about the indications, contraindications, modalities (aerobics, resistance training, stretching and pelvic floor training), frequency, intensity and duration indicated for each gestational trimester. The review addresses physical exercise recommendation both for low risk pregnant women and for special populations, such as athletes and obese, hypertensive and diabetic subjects. The advantages of an active and healthy lifestyle should be always reinforced during and after gestation since pregnancy is an appropriate period to introduce new habits because pregnant women are usually more motivated to adhere to recommendations. Thus, routine exams, frequent returns and supervision are recommended in order to provide new guidelines that will have long-term beneficial effects for both mother and child.