Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):373-375
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):373-375
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):373-379
To investigate the patterns of hospital births in the state of Rio de Janeiro (RJ), Brazil, between 2015 and 2016; considering the classification of obstetric characteristics proposed by Robson and the prenatal care index proposed by Kotelchuck.
Data obtained from the Information System on Live Births of the Informatics Department of the Brazilian Unified Health System (SINASC/DATASUS, in the Portuguese acronym) databases were used to group pregnant women relatively to the Robson classification. A descriptive analysis was performed for each Robson group, considering the variables: maternal age, marital status, schooling, parity, Kotelchuck prenatal adequacy index and gestational age. A logistic model estimated odds ratios (ORs) for cesarean sections (C-sections), considering the aforementioned variables.
Out of the 456,089 live births in Rio de Janeiro state between 2015 and 2016, 391,961 records were retained, 60.3% of which were C-sections. Most pregnant women (58.6%) were classified in groups 5, 2 or 3. The percentage of C-sections in the Robson groups 1, 2, 3, 4, 5 and 8 was much higher than expected. Prenatal care proved to be inadequate for women who subsequently had a vaginal delivery, had an unfavorable family structure and a lower socioeconomic status (mothers without partners and with lower schooling), compared with those undergoing cesarean delivery. For a sameRobson group, the chance of C-section increases when maternal age rises (OR = 3.33 for 41-45 years old), there is the presence of a partner (OR = 1.81) and prenatal care improves (OR = 3.19 for “adequate plus”).
There are indications that in the state of RJ, from 2015 to 2016, many cesarean deliveries were performed due to nonclinical factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):373-379
To investigate the patterns of hospital births in the state of Rio de Janeiro (RJ), Brazil, between 2015 and 2016; considering the classification of obstetric characteristics proposed by Robson and the prenatal care index proposed by Kotelchuck.
Data obtained from the Information System on Live Births of the Informatics Department of the Brazilian Unified Health System (SINASC/DATASUS, in the Portuguese acronym) databases were used to group pregnant women relatively to the Robson classification. A descriptive analysis was performed for each Robson group, considering the variables: maternal age, marital status, schooling, parity, Kotelchuck prenatal adequacy index and gestational age. A logistic model estimated odds ratios (ORs) for cesarean sections (C-sections), considering the aforementioned variables.
Out of the 456,089 live births in Rio de Janeiro state between 2015 and 2016, 391,961 records were retained, 60.3% of which were C-sections. Most pregnant women (58.6%) were classified in groups 5, 2 or 3. The percentage of C-sections in the Robson groups 1, 2, 3, 4, 5 and 8 was much higher than expected. Prenatal care proved to be inadequate for women who subsequently had a vaginal delivery, had an unfavorable family structure and a lower socioeconomic status (mothers without partners and with lower schooling), compared with those undergoing cesarean delivery. For a sameRobson group, the chance of C-section increases when maternal age rises (OR = 3.33 for 41-45 years old), there is the presence of a partner (OR = 1.81) and prenatal care improves (OR = 3.19 for “adequate plus”).
There are indications that in the state of RJ, from 2015 to 2016, many cesarean deliveries were performed due to nonclinical factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(6):373-373
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(6):373-373
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(6):373-373
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(6):373-373
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(6):373-380
DOI 10.1590/S0100-72032000000600008
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(6):373-380
DOI 10.1590/S0100-72032000000600008
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):373-380
The placenta, translates how the fetus experiences the maternal environment and is a principal influence on birth weight (BW).
To explore the relationship between placental growth measures (PGMs) and BW in a public maternity hospital.
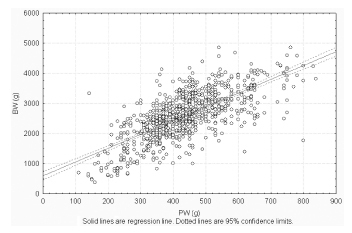
Observational retrospective study of 870 singleton live born infants at Hospital Maternidad Sardá, Universidad de Buenos Aires, Argentina, between January 2011 and August 2012 with complete data of PGMs. Details of history, clinical and obstetrical maternal data, labor and delivery and neonatal outcome data, including placental measures derived from the records, were evaluated. The following manual measurements of the placenta according to standard methods were performed: placental weight (PW, g), larger and smaller diameters (cm), eccentricity, width (cm), shape, area (cm2), BW/PW ratio (BPR) and PW/BW ratio (PBR), and efficiency. Associations between BW and PGMs were examined using multiple linear regression.
Birth weight was correlated with placental weight (R2 =0.49, p < 0.001), whereas gestational age was moderately correlated with placental weight (R2 =0.64, p < 0.001). By gestational age, there was a positive trend for PW and BPR, but an inverse relationship with PBR (p < 0.001). Placental weight alone accounted for 49% of birth weight variability (p < 0,001), whereas all PGMs accounted for 52% (p < 0,001). Combined, PGMs, maternal characteristics (parity, pre-eclampsia, tobacco use), gestational age and gender explained 77.8% of BW variations (p < 0,001). Among preterm births, 59% of BW variances were accounted for by PGMs, compared with 44% at term. All placental measures except BPR were consistently higher in females than in males, which was also not significant. Indices of placental efficiency showed weakly clinical relevance.
Reliable measures of placental growth estimate 53.6% of BW variances and project this outcome to a greater degree in preterm births than at term. These findings would contribute to the understanding of the maternal-placental programming of chronic diseases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):373-380
The placenta, translates how the fetus experiences the maternal environment and is a principal influence on birth weight (BW).
To explore the relationship between placental growth measures (PGMs) and BW in a public maternity hospital.
Observational retrospective study of 870 singleton live born infants at Hospital Maternidad Sardá, Universidad de Buenos Aires, Argentina, between January 2011 and August 2012 with complete data of PGMs. Details of history, clinical and obstetrical maternal data, labor and delivery and neonatal outcome data, including placental measures derived from the records, were evaluated. The following manual measurements of the placenta according to standard methods were performed: placental weight (PW, g), larger and smaller diameters (cm), eccentricity, width (cm), shape, area (cm2), BW/PW ratio (BPR) and PW/BW ratio (PBR), and efficiency. Associations between BW and PGMs were examined using multiple linear regression.
Birth weight was correlated with placental weight (R2 =0.49, p < 0.001), whereas gestational age was moderately correlated with placental weight (R2 =0.64, p < 0.001). By gestational age, there was a positive trend for PW and BPR, but an inverse relationship with PBR (p < 0.001). Placental weight alone accounted for 49% of birth weight variability (p < 0,001), whereas all PGMs accounted for 52% (p < 0,001). Combined, PGMs, maternal characteristics (parity, pre-eclampsia, tobacco use), gestational age and gender explained 77.8% of BW variations (p < 0,001). Among preterm births, 59% of BW variances were accounted for by PGMs, compared with 44% at term. All placental measures except BPR were consistently higher in females than in males, which was also not significant. Indices of placental efficiency showed weakly clinical relevance.
Reliable measures of placental growth estimate 53.6% of BW variances and project this outcome to a greater degree in preterm births than at term. These findings would contribute to the understanding of the maternal-placental programming of chronic diseases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(8):373-378
DOI 10.1590/S0100-72032013000800007
PURPOSE: To compare by transvaginal ultrasound the position of the intrauterine device (IUD) inside the uterine cavity, depending on the time of insertion, postpartum and post-abortion, and during the menstrual cycle. METHODS: Epidemiologic, observational and cross-sectional study carried out between February and July, 2013. A total of 290 women were included, 205 of them with insertion during the menstrual cycle and 85 during the postpartum and post-abortion periods. The independent variables were: age, parity, time of use, insertion time, number of returns to family planning, satisfaction with the method, wish to continue using the device, symptoms and complications. The dependent variable was the adequate position of the IUD inside the uterine cavity. The χ² test with Pearson's correction and the Fisher exact test were used for statistical analysis, with the level of significance set at 5%. RESULTS: The average age was 29.4 years and the average time of IUD use was 2.7 years; 39.3% of the women had symptoms associated with the method, the most frequent being menorrhagia (44.7%). The degree of satisfaction was 85% and 61.4% of the women returned two or more times for consultation about family planning. Age, parity and the position of the uterus in the pelvic cavity was not associated with a poor position of the IUD inside the uterine cavity (p>0.05). Insertion during the menstrual cycle was significantly more associated with a correct position of the IUD than postpartum and post-abortion insertion (p<0.028). CONCLUSION: Postpartum and post-abortion insertion showed worse results regarding the adequacy of IUD position, a fact that was not observed regarding age, parity or position of the uterus in the pelvic cavity.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(8):373-378
DOI 10.1590/S0100-72032013000800007
PURPOSE: To compare by transvaginal ultrasound the position of the intrauterine device (IUD) inside the uterine cavity, depending on the time of insertion, postpartum and post-abortion, and during the menstrual cycle. METHODS: Epidemiologic, observational and cross-sectional study carried out between February and July, 2013. A total of 290 women were included, 205 of them with insertion during the menstrual cycle and 85 during the postpartum and post-abortion periods. The independent variables were: age, parity, time of use, insertion time, number of returns to family planning, satisfaction with the method, wish to continue using the device, symptoms and complications. The dependent variable was the adequate position of the IUD inside the uterine cavity. The χ² test with Pearson's correction and the Fisher exact test were used for statistical analysis, with the level of significance set at 5%. RESULTS: The average age was 29.4 years and the average time of IUD use was 2.7 years; 39.3% of the women had symptoms associated with the method, the most frequent being menorrhagia (44.7%). The degree of satisfaction was 85% and 61.4% of the women returned two or more times for consultation about family planning. Age, parity and the position of the uterus in the pelvic cavity was not associated with a poor position of the IUD inside the uterine cavity (p>0.05). Insertion during the menstrual cycle was significantly more associated with a correct position of the IUD than postpartum and post-abortion insertion (p<0.028). CONCLUSION: Postpartum and post-abortion insertion showed worse results regarding the adequacy of IUD position, a fact that was not observed regarding age, parity or position of the uterus in the pelvic cavity.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):373-375
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(7):373-375