You searched for:"Maria Laura Costa"
We found (27) results for your search.Summary
Rev Bras Ginecol Obstet. 2015;37(6):291-296
DOI 10.1590/SO100-720320150005169
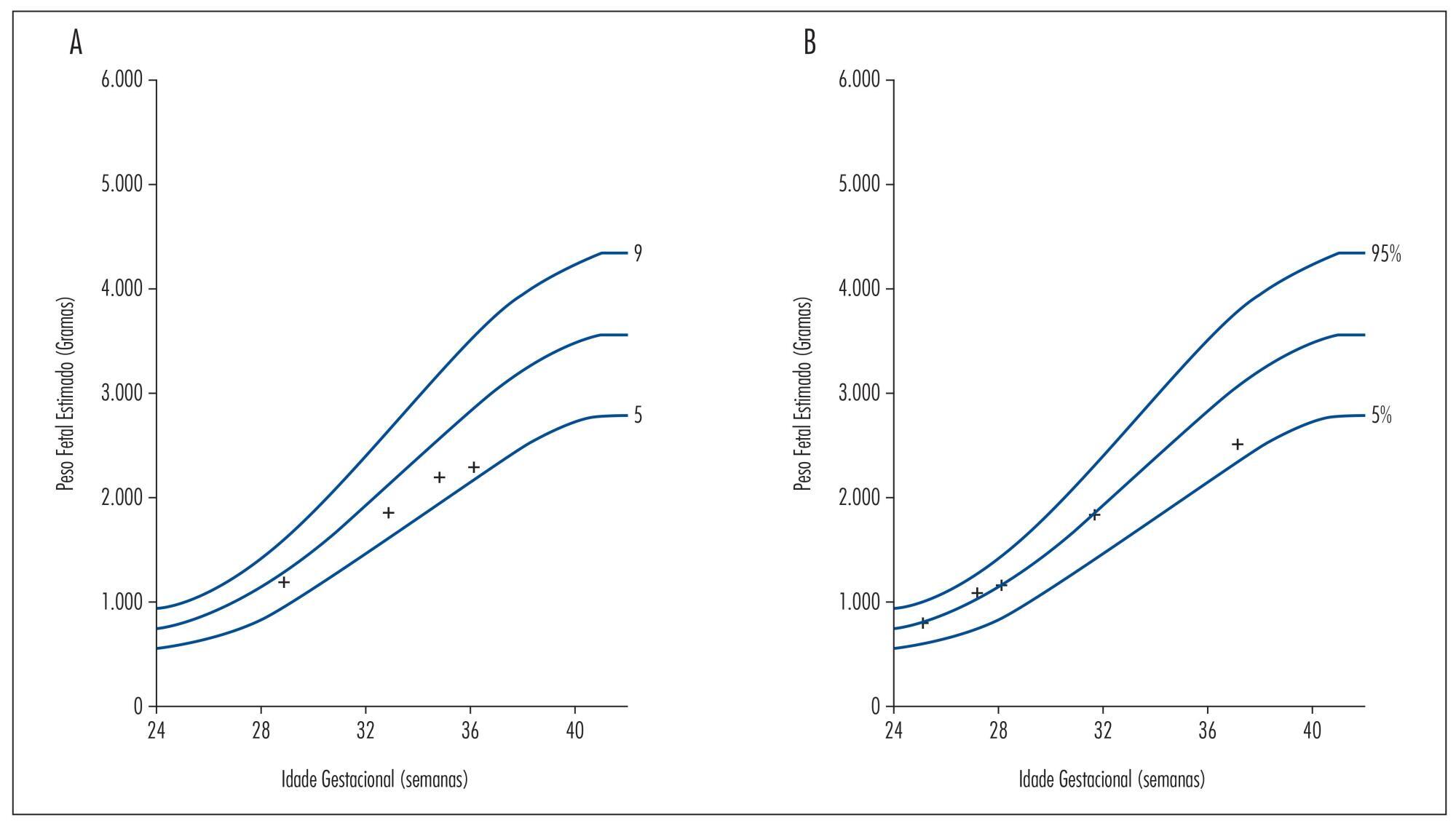
Beta thalassemia major is a rare hereditary blood disease in which impaired synthesis
of beta globin chains causes severe anemia. Medical treatment consists of chronic
blood transfusions and iron chelation. We describe two cases of adolescents with beta
thalassemia major with unplanned pregnancies and late onset of prenatal care. One had
worsening of anemia with increased transfusional requirement, fetal growth
restriction, and placental senescence. The other was also diagnosed with
hypothyroidism and low maternal weight, and was admitted twice during pregnancy due
to dengue shock syndrome and influenza H1N1-associated respiratory infection. She
also developed fetal growth restriction and underwent vaginal delivery at term
complicated by uterine hypotonia. Both patients required blood transfusions after
birth and chose medroxyprogesterone as a contraceptive method afterwards. This report
highlights the importance of medical advice on contraceptive methods for these women
and the role of a specialized prenatal follow-up in association with a
hematologist.
Summary
Rev Bras Ginecol Obstet. 2015;37(6):291-296
DOI 10.1590/SO100-720320150005169
Beta thalassemia major is a rare hereditary blood disease in which impaired synthesis
of beta globin chains causes severe anemia. Medical treatment consists of chronic
blood transfusions and iron chelation. We describe two cases of adolescents with beta
thalassemia major with unplanned pregnancies and late onset of prenatal care. One had
worsening of anemia with increased transfusional requirement, fetal growth
restriction, and placental senescence. The other was also diagnosed with
hypothyroidism and low maternal weight, and was admitted twice during pregnancy due
to dengue shock syndrome and influenza H1N1-associated respiratory infection. She
also developed fetal growth restriction and underwent vaginal delivery at term
complicated by uterine hypotonia. Both patients required blood transfusions after
birth and chose medroxyprogesterone as a contraceptive method afterwards. This report
highlights the importance of medical advice on contraceptive methods for these women
and the role of a specialized prenatal follow-up in association with a
hematologist.
Summary
Rev Bras Ginecol Obstet. 2019;41(5):318-332
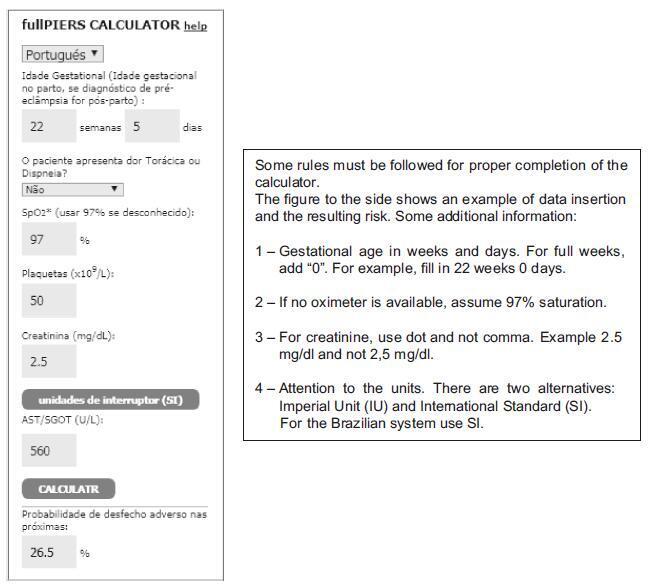
Pre-eclampsia is a multifactorial and multisystemic disease specific to gestation. It is classically diagnosed by the presence of hypertension associated with proteinuria manifested in a previously normotensive pregnant woman after the 20th week of gestation. Pre-eclampsia is also considered in the absence of proteinuria if there is target organ damage. The present review takes a general approach focused on aspects of practical interest in the clinical and obstetric care of these women. Thus, it explores the still unknown etiology, current aspects of pathophysiology and of the diagnosis, the approach to disease prediction, its adverse outcomes and prevention. Management is based on general principles, on nonpharmacological and on pharmacological clinical treatment of severe or nonsevere situations with emphasis on the hypertensive crisis and eclampsia. Obstetric management is based on preeclampsia without or with signs of clinical and/or laboratory deterioration, stratification of gestational age
Summary
Rev Bras Ginecol Obstet. 2019;41(5):318-332
Pre-eclampsia is a multifactorial and multisystemic disease specific to gestation. It is classically diagnosed by the presence of hypertension associated with proteinuria manifested in a previously normotensive pregnant woman after the 20th week of gestation. Pre-eclampsia is also considered in the absence of proteinuria if there is target organ damage. The present review takes a general approach focused on aspects of practical interest in the clinical and obstetric care of these women. Thus, it explores the still unknown etiology, current aspects of pathophysiology and of the diagnosis, the approach to disease prediction, its adverse outcomes and prevention. Management is based on general principles, on nonpharmacological and on pharmacological clinical treatment of severe or nonsevere situations with emphasis on the hypertensive crisis and eclampsia. Obstetric management is based on preeclampsia without or with signs of clinical and/or laboratory deterioration, stratification of gestational age
Summary
Rev Bras Ginecol Obstet. 2023;45(7):371-376
To compare cesarean section (CS) rates according to the Robson Ten Group Classification System (RTGCS) and its indications in pregnant women admitted for childbirth during the first wave of the coronavirus disease 2019 (COVID-19) pandemic with those of the previous year.
We conducted a cross-sectional study to compare women admitted for childbirth from April to October 2019 (before the pandemic) and from March to September 2020 (during the pandemic). The CSs and their indications were classified on admission according to the RTGCS, and we also collected data on the route of delivery (vaginal or CS). Both periods were compared using the Chi-squared (χ2) test or the Fisher exact test.
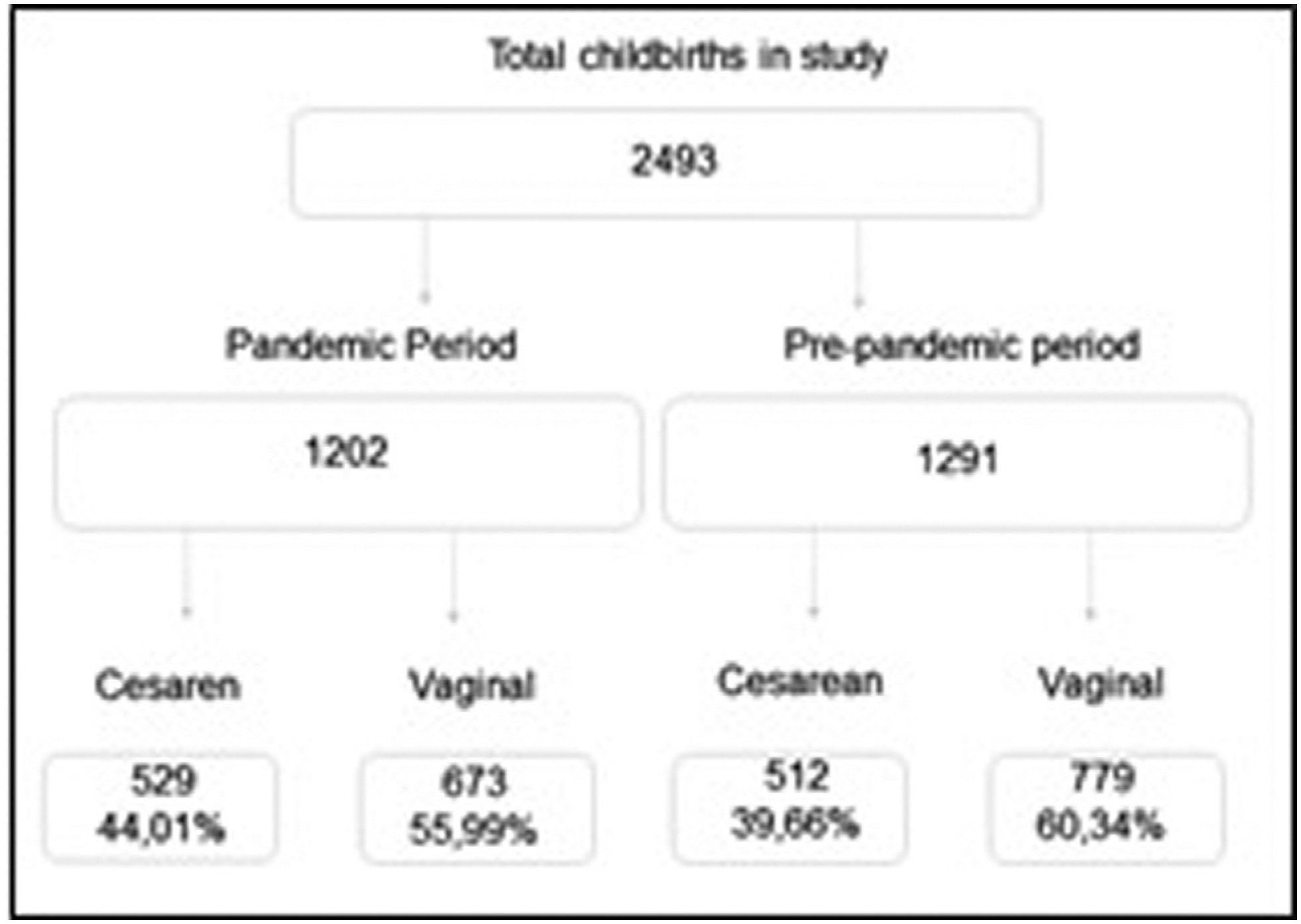
In total, 2,493 women were included, 1,291 in the prepandemic and 1,202 in the pandemic period. There was a a significant increase in the CS rate (from 39.66% to 44.01%; p = 0.028), mostly due to maternal request (from 9.58% to 25.38%; p < 0.01). Overall, groups 5 and 2 contributed the most to the CS rates. The rates decreased among group 1 and increased among group 2 during the pandemic, with no changes in group 10.
There was an apparent change in the RTGSC comparing both periods, with a significant increase in CS rates, mainly by maternal request, most likely because of changes during the pandemic and uncertainties and fear concerning COVID-19.
Summary
Rev Bras Ginecol Obstet. 2023;45(7):371-376
To compare cesarean section (CS) rates according to the Robson Ten Group Classification System (RTGCS) and its indications in pregnant women admitted for childbirth during the first wave of the coronavirus disease 2019 (COVID-19) pandemic with those of the previous year.
We conducted a cross-sectional study to compare women admitted for childbirth from April to October 2019 (before the pandemic) and from March to September 2020 (during the pandemic). The CSs and their indications were classified on admission according to the RTGCS, and we also collected data on the route of delivery (vaginal or CS). Both periods were compared using the Chi-squared (χ2) test or the Fisher exact test.
In total, 2,493 women were included, 1,291 in the prepandemic and 1,202 in the pandemic period. There was a a significant increase in the CS rate (from 39.66% to 44.01%; p = 0.028), mostly due to maternal request (from 9.58% to 25.38%; p < 0.01). Overall, groups 5 and 2 contributed the most to the CS rates. The rates decreased among group 1 and increased among group 2 during the pandemic, with no changes in group 10.
There was an apparent change in the RTGSC comparing both periods, with a significant increase in CS rates, mainly by maternal request, most likely because of changes during the pandemic and uncertainties and fear concerning COVID-19.
Summary
Rev Bras Ginecol Obstet. 2021;43(5):377-383
The coronavirus disease 2019 (COVID-19) is a pandemic viral disease, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The impact of the disease among the obstetric population remains unclear, and the study of the placenta can provide valuable information. Adequate sampling of the placental tissue can help characterize the pathways of viral infections.
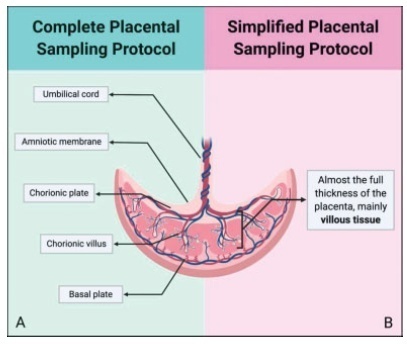
A protocol of placental sampling is proposed, aiming at guaranteeing representativity of the placenta and describing the adequate conservation of samples and their integrity for future analysis. The protocol is presented in its complete and simplified versions, allowing its implementation in different complexity settings.
Sampling with the minimum possible interval from childbirth is the key for adequate sampling and storage. This protocol has already been implemented during the Zika virus outbreak.
A protocol for adequate sampling and storage of placental tissue is fundamental for adequate evaluation of viral infections on the placenta. During the COVID-19 pandemic, implementation of this protocol may help to elucidate critical aspects of the SARS-CoV-2 infection.
Summary
Rev Bras Ginecol Obstet. 2021;43(5):377-383
The coronavirus disease 2019 (COVID-19) is a pandemic viral disease, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The impact of the disease among the obstetric population remains unclear, and the study of the placenta can provide valuable information. Adequate sampling of the placental tissue can help characterize the pathways of viral infections.
A protocol of placental sampling is proposed, aiming at guaranteeing representativity of the placenta and describing the adequate conservation of samples and their integrity for future analysis. The protocol is presented in its complete and simplified versions, allowing its implementation in different complexity settings.
Sampling with the minimum possible interval from childbirth is the key for adequate sampling and storage. This protocol has already been implemented during the Zika virus outbreak.
A protocol for adequate sampling and storage of placental tissue is fundamental for adequate evaluation of viral infections on the placenta. During the COVID-19 pandemic, implementation of this protocol may help to elucidate critical aspects of the SARS-CoV-2 infection.
Summary
Rev Bras Ginecol Obstet. 2019;41(6):379-386
Several factors might affect the health and the quality of life of women who had a severe maternal morbidity (SMM) or a maternal near-miss (MNM) episode. The objective of the present study was to explore the perspectives of the professionals on the repercussions of SMM or of MNM after interviewing women who survived such episodes.
Selected cases that captured the attention of professionals were reported. The professionals built individually 10 narratives, which were analyzed with the technique of content analysis.
According to the perspectives of the professionals, women surviving a severe maternal condition and their families experienced clinical and psychosocial consequences. Some cases portrayed the intense psychological distress in mourning for the loss of the fetus or of their reproductive capacity and changes in family dynamics generating emotional overload, depression, and gender violence.
The analysis of narratives may offer an idea on the complexity of the perception of care by professionals and on the need for an interdisciplinary follow-up of women surviving an SMM or an MNM episode.
Summary
Rev Bras Ginecol Obstet. 2019;41(6):379-386
Several factors might affect the health and the quality of life of women who had a severe maternal morbidity (SMM) or a maternal near-miss (MNM) episode. The objective of the present study was to explore the perspectives of the professionals on the repercussions of SMM or of MNM after interviewing women who survived such episodes.
Selected cases that captured the attention of professionals were reported. The professionals built individually 10 narratives, which were analyzed with the technique of content analysis.
According to the perspectives of the professionals, women surviving a severe maternal condition and their families experienced clinical and psychosocial consequences. Some cases portrayed the intense psychological distress in mourning for the loss of the fetus or of their reproductive capacity and changes in family dynamics generating emotional overload, depression, and gender violence.
The analysis of narratives may offer an idea on the complexity of the perception of care by professionals and on the need for an interdisciplinary follow-up of women surviving an SMM or an MNM episode.
Summary
Rev Bras Ginecol Obstet. 2019;41(7):419-424
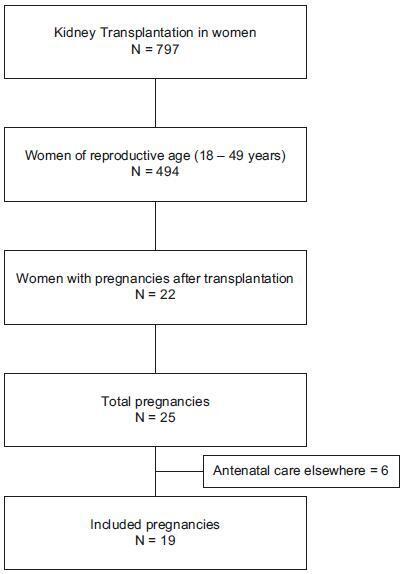
To assess maternal and perinatal outcomes in pregnancies after kidney transplantation in a tertiary center in Brazil.
Retrospective cohort of pregnancies in women with kidney transplantation at the Universidade Estadual de Campinas, from January 1995 until December 2017. Medical charts were reviewed, andmaternal and perinatal outcomes were described as means and frequencies. Renal function and blood pressure were evaluated during pregnancy and postpartum.
A total of 22 women had at least 1 pregnancy during the considered timeinterval, and 3 of them had > 1 pregnancy, totalizing 25 pregnancies. The mean age at transplantation was of 24.6 ± 4.2 years old, and the mean time interval until pregnancy was of 67.8 ± 46.3months. Themost frequent complication during pregnancywas hypertension, which affected 11 (64.7%)women. The gestational age at delivery was 34.7 ± 4weeks, and 47% of these pregnancies were preterm (< 37 weeks). A total of 88.2% of the women delivered by cesarean section. Renal function, measured by serum creatinine, remained stable during pregnancy, and the systolic blood pressure increased significantly, while the diastolic blood pressure did not differ during pregnancy.
Pregnancy after kidney transplantation is a rare event. Pre-eclampsia and prematurity were frequent complications, and cesarean section rates were very high. A specialized antenatal and postpartum care with a multiprofessional approach and continuous monitoring of graft function are essential for the early diagnosis of complications and improved outcomes.
Summary
Rev Bras Ginecol Obstet. 2019;41(7):419-424
To assess maternal and perinatal outcomes in pregnancies after kidney transplantation in a tertiary center in Brazil.
Retrospective cohort of pregnancies in women with kidney transplantation at the Universidade Estadual de Campinas, from January 1995 until December 2017. Medical charts were reviewed, andmaternal and perinatal outcomes were described as means and frequencies. Renal function and blood pressure were evaluated during pregnancy and postpartum.
A total of 22 women had at least 1 pregnancy during the considered timeinterval, and 3 of them had > 1 pregnancy, totalizing 25 pregnancies. The mean age at transplantation was of 24.6 ± 4.2 years old, and the mean time interval until pregnancy was of 67.8 ± 46.3months. Themost frequent complication during pregnancywas hypertension, which affected 11 (64.7%)women. The gestational age at delivery was 34.7 ± 4weeks, and 47% of these pregnancies were preterm (< 37 weeks). A total of 88.2% of the women delivered by cesarean section. Renal function, measured by serum creatinine, remained stable during pregnancy, and the systolic blood pressure increased significantly, while the diastolic blood pressure did not differ during pregnancy.
Pregnancy after kidney transplantation is a rare event. Pre-eclampsia and prematurity were frequent complications, and cesarean section rates were very high. A specialized antenatal and postpartum care with a multiprofessional approach and continuous monitoring of graft function are essential for the early diagnosis of complications and improved outcomes.
Summary
Rev Bras Ginecol Obstet. 2022;44(5):475-482
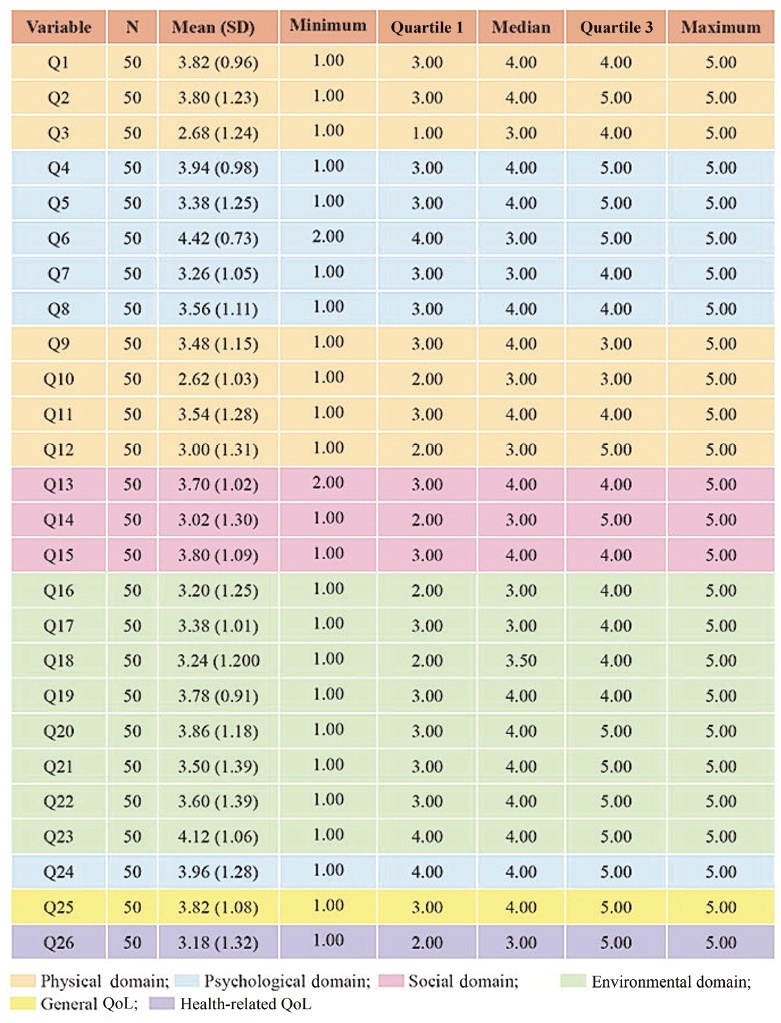
To assess the quality of life (QoL) of pregnant women with systemic lupus erythematosus (SLE) treated at a high-risk prenatal outpatient clinic during the third trimester of gestation.
An observational descriptive study was performed in a high-risk prenatal outpatient clinic. Women in the third trimester of pregnancy and undergoing antenatal care between July 2017 and July 2019 answered the abbreviated World Health Organization Quality of Life (WHOQOL-BREF) questionnaire, consisting of 26 questions divided into 4 domains (physical, psychological, social and environmental).
We interviewed 50 pregnant women with a mean gestational age of 30 weeks (standard deviation [SD]: 10 weeks) who were diagnosed with SLE. The average age of the participants was 30 years (SD: 14.85), and the average time since the diagnosis of SLE was of 9.06 years (SD: 6.8 years). Most participants had a partner, did not plan their pregnancy (76%), and did not use contraception prior to pregnancy (80%). The score of each domain ranges from 0 (the worst score) to 100 (the best score). The means ± SDs of the scores of the participants on each domain were: physical - 52.21 ± 18.44); psychological - 64.17 ± 18.56); social - 66.33 ± 27.09); and environmental - 64.56 (18.53). The means ± SDs of the general QoL, and health-related QoL items were of 70.50 ± 24.06 and 70.00 ± 30.72 respectively.
The physical domain presented the lowest scores compared with the other three domains. Pregnant women with SLE had high overall QoL scores, and their health-related QoL scores were also relatively high.
Summary
Rev Bras Ginecol Obstet. 2022;44(5):475-482
To assess the quality of life (QoL) of pregnant women with systemic lupus erythematosus (SLE) treated at a high-risk prenatal outpatient clinic during the third trimester of gestation.
An observational descriptive study was performed in a high-risk prenatal outpatient clinic. Women in the third trimester of pregnancy and undergoing antenatal care between July 2017 and July 2019 answered the abbreviated World Health Organization Quality of Life (WHOQOL-BREF) questionnaire, consisting of 26 questions divided into 4 domains (physical, psychological, social and environmental).
We interviewed 50 pregnant women with a mean gestational age of 30 weeks (standard deviation [SD]: 10 weeks) who were diagnosed with SLE. The average age of the participants was 30 years (SD: 14.85), and the average time since the diagnosis of SLE was of 9.06 years (SD: 6.8 years). Most participants had a partner, did not plan their pregnancy (76%), and did not use contraception prior to pregnancy (80%). The score of each domain ranges from 0 (the worst score) to 100 (the best score). The means ± SDs of the scores of the participants on each domain were: physical - 52.21 ± 18.44); psychological - 64.17 ± 18.56); social - 66.33 ± 27.09); and environmental - 64.56 (18.53). The means ± SDs of the general QoL, and health-related QoL items were of 70.50 ± 24.06 and 70.00 ± 30.72 respectively.
The physical domain presented the lowest scores compared with the other three domains. Pregnant women with SLE had high overall QoL scores, and their health-related QoL scores were also relatively high.
Summary
Rev Bras Ginecol Obstet. 2018;40(8):500-500
Summary
Rev Bras Ginecol Obstet. 2018;40(8):500-500