You searched for:"Jose Guilherme Cecatti"
We found (51) results for your search.Summary
Rev Bras Ginecol Obstet. 2018;40(4):171-179
To evaluate the use of tocolysis in cases of preterm birth due to spontaneous preterm labor in a Brazilian sample.
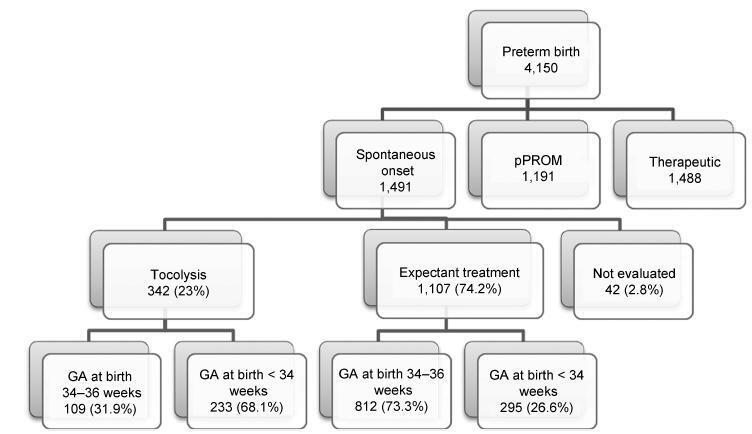
A sample of 1,491 women with preterm birth due to spontaneous preterm labor were assessed, considering treatment with tocolysis or expectant management, according to gestational age at birth (< 34 weeks and 34 to 36 þ 6 weeks) and drugs prescribed. The study took place in 20 Brazilian hospitals from April 2011 to July 2012. Bivariate analyses were conducted to evaluate associations with sociodemographic and obstetric characteristics and odds ratios with their respective 95% confidence intervals were estimated for maternal and neonatal outcomes.
A total of 1,491 cases of preterm birth were considered. Tocolysis was performed in 342 cases (23%), 233 of which (68.1%) were delivered before 34 weeks. Within the expectant management group, 73% was late preterm and with more advanced labor at the time of admission. The most used drugs were calcium channel blockers (62.3%), followed by betamimetics (33%). Among the subjects in the tocolysis group, there were more neonatal and maternal complications (majority non-severe) and an occurrence of corticosteroid use that was 29 higher than in the expectant management group.
Tocolysis is favored in cases of earlier labor and also among thosewith less than 34 weeks of gestation, using preferably calcium channel blockers, with success in achieving increased corticosteroid use. Tocolysis, in general, was related to higher maternal and neonatal complication rates, which may be due to the baseline difference between cases at admission. However, these results should raise awareness to tocolysis use.
Summary
Rev Bras Ginecol Obstet. 2018;40(4):171-179
To evaluate the use of tocolysis in cases of preterm birth due to spontaneous preterm labor in a Brazilian sample.
A sample of 1,491 women with preterm birth due to spontaneous preterm labor were assessed, considering treatment with tocolysis or expectant management, according to gestational age at birth (< 34 weeks and 34 to 36 þ 6 weeks) and drugs prescribed. The study took place in 20 Brazilian hospitals from April 2011 to July 2012. Bivariate analyses were conducted to evaluate associations with sociodemographic and obstetric characteristics and odds ratios with their respective 95% confidence intervals were estimated for maternal and neonatal outcomes.
A total of 1,491 cases of preterm birth were considered. Tocolysis was performed in 342 cases (23%), 233 of which (68.1%) were delivered before 34 weeks. Within the expectant management group, 73% was late preterm and with more advanced labor at the time of admission. The most used drugs were calcium channel blockers (62.3%), followed by betamimetics (33%). Among the subjects in the tocolysis group, there were more neonatal and maternal complications (majority non-severe) and an occurrence of corticosteroid use that was 29 higher than in the expectant management group.
Tocolysis is favored in cases of earlier labor and also among thosewith less than 34 weeks of gestation, using preferably calcium channel blockers, with success in achieving increased corticosteroid use. Tocolysis, in general, was related to higher maternal and neonatal complication rates, which may be due to the baseline difference between cases at admission. However, these results should raise awareness to tocolysis use.
Summary
Rev Bras Ginecol Obstet. 2000;22(3):175-179
DOI 10.1590/S0100-72032000000300009
Purpose: to evaluate the route of delivery in a group of low-income primipara pregnant women with a previous cesarean section, and the factors associated with the repetition of the cesarean section on the second delivery. Patients and Methods: it was a case-control study including 356 women who were assisted at the Maternity of CAISM/UNICAMP during the period between January 1993 and January 1996. The cases were 153 women whose second delivery was through a cesarean section and the controls were 203 women whose second delivery was vaginal. For analysis, means, standard deviation, Student's t-test, Mann-Whitney test, chi² test and odds ratio (OR) with 95% CI for each factor possibly associated with cesarean section on the second delivery were used. Results: the route of the second delivery was vaginal for 57% of the women. Among the several variables studied, those which showed to be significantly associated with a cesarean section on the second delivery were: higher maternal age (for women over 35 years, OR = 16.4), previous abortions (OR = 2.09), induced labor (OR = 3,83), premature rupture of membranes (OR = 2.83), not having an epidural analgesia performed during labor (OR = 5.3), the finding of some alteration in fetal well-being (OR = 2.7) and the delivery occurring during the afternoon (OR = 1.92). Conclusions: these results indicate that the factors associated with the repetition of cesarean section in women with a previous scar of cesarean section in this population are predominantly medical; however, there is still the possibility of proposing interventions directed to decreasing the rates of repeated cesarean sections.
Summary
Rev Bras Ginecol Obstet. 2000;22(3):175-179
DOI 10.1590/S0100-72032000000300009
Purpose: to evaluate the route of delivery in a group of low-income primipara pregnant women with a previous cesarean section, and the factors associated with the repetition of the cesarean section on the second delivery. Patients and Methods: it was a case-control study including 356 women who were assisted at the Maternity of CAISM/UNICAMP during the period between January 1993 and January 1996. The cases were 153 women whose second delivery was through a cesarean section and the controls were 203 women whose second delivery was vaginal. For analysis, means, standard deviation, Student's t-test, Mann-Whitney test, chi² test and odds ratio (OR) with 95% CI for each factor possibly associated with cesarean section on the second delivery were used. Results: the route of the second delivery was vaginal for 57% of the women. Among the several variables studied, those which showed to be significantly associated with a cesarean section on the second delivery were: higher maternal age (for women over 35 years, OR = 16.4), previous abortions (OR = 2.09), induced labor (OR = 3,83), premature rupture of membranes (OR = 2.83), not having an epidural analgesia performed during labor (OR = 5.3), the finding of some alteration in fetal well-being (OR = 2.7) and the delivery occurring during the afternoon (OR = 1.92). Conclusions: these results indicate that the factors associated with the repetition of cesarean section in women with a previous scar of cesarean section in this population are predominantly medical; however, there is still the possibility of proposing interventions directed to decreasing the rates of repeated cesarean sections.
Summary
Rev Bras Ginecol Obstet. 1998;20(4):181-185
DOI 10.1590/S0100-72031998000400002
With the purpose of identifying the social, demographic, pregnancy-related and medical care factors associated with maternal death, this study evaluated all deaths of women aged 10 to 49 years occurring in Recife, Pernambuco, Brazil, during 1992 and 1993. The data were obtained reviewing 1,013 death certificates, with 42 cases of identified maternal deaths. The data of these deaths were complemented with information from medical records, autopsies and also interviews with physicians from the hospitals where the death took place, and with the dead women's relatives. Almost two thirds (62%) of maternal deaths occurred among women aged 20 to 29 years and more than half of them were single. There was a higher number of deaths among caesarean deliveries than among vaginal ones. The majority of deaths occurred within the first three days of hospitalization and approximately 90% of hospital charges were sponsored by the National Health System (SUS).
Summary
Rev Bras Ginecol Obstet. 1998;20(4):181-185
DOI 10.1590/S0100-72031998000400002
With the purpose of identifying the social, demographic, pregnancy-related and medical care factors associated with maternal death, this study evaluated all deaths of women aged 10 to 49 years occurring in Recife, Pernambuco, Brazil, during 1992 and 1993. The data were obtained reviewing 1,013 death certificates, with 42 cases of identified maternal deaths. The data of these deaths were complemented with information from medical records, autopsies and also interviews with physicians from the hospitals where the death took place, and with the dead women's relatives. Almost two thirds (62%) of maternal deaths occurred among women aged 20 to 29 years and more than half of them were single. There was a higher number of deaths among caesarean deliveries than among vaginal ones. The majority of deaths occurred within the first three days of hospitalization and approximately 90% of hospital charges were sponsored by the National Health System (SUS).
Summary
Rev Bras Ginecol Obstet. 2005;27(4):197-203
DOI 10.1590/S0100-72032005000400006
PURPOSE: to apply a severity score to cases of severe maternal morbidity (SMM) and to compare the classification criteria. METHODS: a control-case study was performed as a secondary analysis of cases of SMM in a tertiary level maternity unit for a period of 12-month. A specific score for assessing the degree of severity was applied to cases identified as SMM. Twenty cases of near miss maternal morbidity (higher severity) were compared to 104 control cases (lower severity) of other severe morbidities, regarding risk factors, primary determinants and assistance requirements. Analyses were performed with means and proportions, using Student's t, Wilcoxon and chi2 statistical tests, and estimations of OR and 95% CI. RESULTS: the higher severity (near miss) was identified in 16.1% of cases and the history of abortion was the only factor statistically associated with it (OR=3.41, 95% CI 1.08-10.79). In fact, the indices of assistance complexity were more frequent in the near-miss morbidity group, which also presented less hypertension (30% against 62.5%) and more hemorrhage (35.5% against 10.6%) as primary determinant factors of severe morbidity. CONCLUSIONS: the higher severity of maternal morbidity was associated with a history of abortion and with hemorrhage as a cause. The applied score was able to identify a higher severity subgroup (near miss), which needs more complex professional and institutional care in order to avoid the occurrence of death.
Summary
Rev Bras Ginecol Obstet. 2005;27(4):197-203
DOI 10.1590/S0100-72032005000400006
PURPOSE: to apply a severity score to cases of severe maternal morbidity (SMM) and to compare the classification criteria. METHODS: a control-case study was performed as a secondary analysis of cases of SMM in a tertiary level maternity unit for a period of 12-month. A specific score for assessing the degree of severity was applied to cases identified as SMM. Twenty cases of near miss maternal morbidity (higher severity) were compared to 104 control cases (lower severity) of other severe morbidities, regarding risk factors, primary determinants and assistance requirements. Analyses were performed with means and proportions, using Student's t, Wilcoxon and chi2 statistical tests, and estimations of OR and 95% CI. RESULTS: the higher severity (near miss) was identified in 16.1% of cases and the history of abortion was the only factor statistically associated with it (OR=3.41, 95% CI 1.08-10.79). In fact, the indices of assistance complexity were more frequent in the near-miss morbidity group, which also presented less hypertension (30% against 62.5%) and more hemorrhage (35.5% against 10.6%) as primary determinant factors of severe morbidity. CONCLUSIONS: the higher severity of maternal morbidity was associated with a history of abortion and with hemorrhage as a cause. The applied score was able to identify a higher severity subgroup (near miss), which needs more complex professional and institutional care in order to avoid the occurrence of death.
Summary
Rev Bras Ginecol Obstet. 2017;39(5):209-216
In 2013, it was estimated that 289,000 maternal deaths occurred worldwide. The maternal mortality ratio has decreased in many countries in the past decades, due to early identification and treatment of obstetric complications, despite the dissimilarities observed in diverse locations and populations. Black women, for instance, have always been more susceptible to the occurrence of maternal mortality and severe morbidity. Therefore, the objective of this study is to assess skin color as a predictive factor for maternal near miss (MNM) in a sample of Brazilian women interviewed in the Brazilian National Demographic and Health Survey (DHS) of 2006.
A secondary analysis of the DHS database, a population-based crosssectional nationally representative study was conducted. This database is of public domain. The risk of maternal complications according to ethnic group and the associated sociodemographic characteristics were evaluated. For the data analysis, the odds ratios and respective 95% confidence intervals were calculated.
In the sample interviewed, 59% of women were black or brown (mixed-race). Approximately 23% of women had some complication, and 2% of these women had at least one MNM pragmatic criterion. The MNM rate was 31 per 1,000 live births, and its occurrence was not statistically different among the ethnic groups. The only factors identified that were considered to be associated with the occurrence of MNM were maternal age above 40 and women not currently attending school, but only among white women.
The 2006 DHS results did not show a higher occurrence of maternal complications, and specifically of MNM associated with black/brown skin color.
Summary
Rev Bras Ginecol Obstet. 2017;39(5):209-216
In 2013, it was estimated that 289,000 maternal deaths occurred worldwide. The maternal mortality ratio has decreased in many countries in the past decades, due to early identification and treatment of obstetric complications, despite the dissimilarities observed in diverse locations and populations. Black women, for instance, have always been more susceptible to the occurrence of maternal mortality and severe morbidity. Therefore, the objective of this study is to assess skin color as a predictive factor for maternal near miss (MNM) in a sample of Brazilian women interviewed in the Brazilian National Demographic and Health Survey (DHS) of 2006.
A secondary analysis of the DHS database, a population-based crosssectional nationally representative study was conducted. This database is of public domain. The risk of maternal complications according to ethnic group and the associated sociodemographic characteristics were evaluated. For the data analysis, the odds ratios and respective 95% confidence intervals were calculated.
In the sample interviewed, 59% of women were black or brown (mixed-race). Approximately 23% of women had some complication, and 2% of these women had at least one MNM pragmatic criterion. The MNM rate was 31 per 1,000 live births, and its occurrence was not statistically different among the ethnic groups. The only factors identified that were considered to be associated with the occurrence of MNM were maternal age above 40 and women not currently attending school, but only among white women.
The 2006 DHS results did not show a higher occurrence of maternal complications, and specifically of MNM associated with black/brown skin color.
Summary
Rev Bras Ginecol Obstet. 1999;21(4):227-232
DOI 10.1590/S0100-72031999000400008
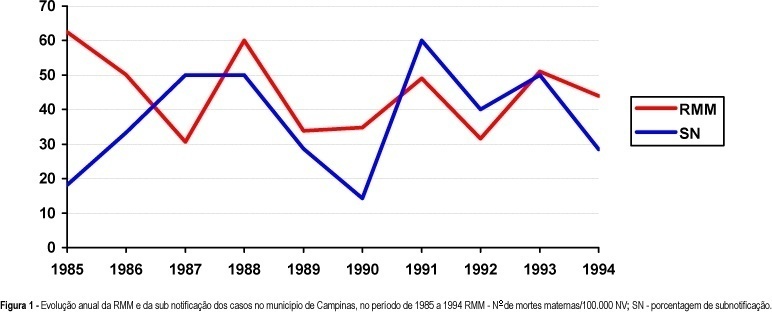
Purpose: to identify and investigate the causes of maternal death that occurred in Campinas from 1992 to 1994. Methods: a total of 204 death certificates (DC) whose causes of death were maternal (declared and/or presumed) were selected among the 1032 DC's of 10 to 49 year-old women. A complementary investigation was performed consulting hospital records, Death Survey Units, and households. Results: a total of 20 maternal deaths were confirmed, corresponding to a maternal mortality ratio of 42.2 deaths per 100,000 live births. The direct obstetrical causes were responsible for 85% of the deaths (17 cases). Abortion complications were the main causes of death (7 cases), followed by hemorrhage (4 cases), preeclampsia (3 cases) and puerperal infection (3 cases). Conclusions: despite the apparent progress concerning the reduction in deaths due to hypertensive syndromes during pregnancy, that were the main causes in earlier periods, there was no improvement in the maternal mortality ratio for this studied period. Unfortunately, this lack of progress was due to abortion complications. A better coverage and efficiency of family planning programs, besides the need for implementation of a real epidemiological surveillance of maternal deaths, as well as a better social protection of the pregnant woman, the mother, and the newborns, could reduce their occurrence and specially those due to abortions.
Summary
Rev Bras Ginecol Obstet. 1999;21(4):227-232
DOI 10.1590/S0100-72031999000400008
Purpose: to identify and investigate the causes of maternal death that occurred in Campinas from 1992 to 1994. Methods: a total of 204 death certificates (DC) whose causes of death were maternal (declared and/or presumed) were selected among the 1032 DC's of 10 to 49 year-old women. A complementary investigation was performed consulting hospital records, Death Survey Units, and households. Results: a total of 20 maternal deaths were confirmed, corresponding to a maternal mortality ratio of 42.2 deaths per 100,000 live births. The direct obstetrical causes were responsible for 85% of the deaths (17 cases). Abortion complications were the main causes of death (7 cases), followed by hemorrhage (4 cases), preeclampsia (3 cases) and puerperal infection (3 cases). Conclusions: despite the apparent progress concerning the reduction in deaths due to hypertensive syndromes during pregnancy, that were the main causes in earlier periods, there was no improvement in the maternal mortality ratio for this studied period. Unfortunately, this lack of progress was due to abortion complications. A better coverage and efficiency of family planning programs, besides the need for implementation of a real epidemiological surveillance of maternal deaths, as well as a better social protection of the pregnant woman, the mother, and the newborns, could reduce their occurrence and specially those due to abortions.
Summary
Rev Bras Ginecol Obstet. 2005;27(1):24-31
DOI 10.1590/S0100-72032005000100006
PURPOSE: to compare the effectiveness and safety of sublingual misoprostol (25 µg) versus vaginal misoprostol (25 µg) (Prostokos®) for labor induction with gestational age > 37 weeks and unripe cervices. METHODS: a randomized controlled clinical trial was performed at the Maternidade Monteiro de Morais (CISAM-UPE), in Recife - PE, Brazil, from October 2003 to February 2004. One hundred and twenty-three women with gestational age > 37 weeks, Bishop score <8, not in labor and with medical indication for interruption of pregnancy were included in this study. The women received randomly 25 µg sublingual misoprostol or 25 µg vaginal misoprostol every 6 h, not exceeding eight doses. In order to evaluate the differences between the groups, means, standard deviations, Student's t-test, c² trend and Mann-Whitney test were used. The statistical significance was considered to be 5%. RESULTS: there were no significant differences between the number of women with vaginal delivery in the sublingual group as compared with the vaginal group (65.5 vs 75.8%, p<0.22), or in the interval of time between the induction onset and delivery (24 h and 42 min vs 20 h and 37 min respectively, p=0.11). The two groups, sublingual and vaginal, also did not differ as to the hyperstimulation syndrome (1.7 vs 3.2%, p=0.95), meconium incidence (5.2 vs 4.8%, p=0.74), Apgar score <7 at 5 min (3.4 vs 4.8%, p=0.98) and other adverse effects. CONCLUSION: twenty-five micrograms of sublingual misoprostol every six h presented the same effectiveness and safety as an equal vaginally administered dose of this substance. Sublingual misoprostol seems to be acceptable and is another option to be considered for labor induction.
Summary
Rev Bras Ginecol Obstet. 2005;27(1):24-31
DOI 10.1590/S0100-72032005000100006
PURPOSE: to compare the effectiveness and safety of sublingual misoprostol (25 µg) versus vaginal misoprostol (25 µg) (Prostokos®) for labor induction with gestational age > 37 weeks and unripe cervices. METHODS: a randomized controlled clinical trial was performed at the Maternidade Monteiro de Morais (CISAM-UPE), in Recife - PE, Brazil, from October 2003 to February 2004. One hundred and twenty-three women with gestational age > 37 weeks, Bishop score <8, not in labor and with medical indication for interruption of pregnancy were included in this study. The women received randomly 25 µg sublingual misoprostol or 25 µg vaginal misoprostol every 6 h, not exceeding eight doses. In order to evaluate the differences between the groups, means, standard deviations, Student's t-test, c² trend and Mann-Whitney test were used. The statistical significance was considered to be 5%. RESULTS: there were no significant differences between the number of women with vaginal delivery in the sublingual group as compared with the vaginal group (65.5 vs 75.8%, p<0.22), or in the interval of time between the induction onset and delivery (24 h and 42 min vs 20 h and 37 min respectively, p=0.11). The two groups, sublingual and vaginal, also did not differ as to the hyperstimulation syndrome (1.7 vs 3.2%, p=0.95), meconium incidence (5.2 vs 4.8%, p=0.74), Apgar score <7 at 5 min (3.4 vs 4.8%, p=0.98) and other adverse effects. CONCLUSION: twenty-five micrograms of sublingual misoprostol every six h presented the same effectiveness and safety as an equal vaginally administered dose of this substance. Sublingual misoprostol seems to be acceptable and is another option to be considered for labor induction.

Summary
Rev Bras Ginecol Obstet. 2023;45(5):253-260
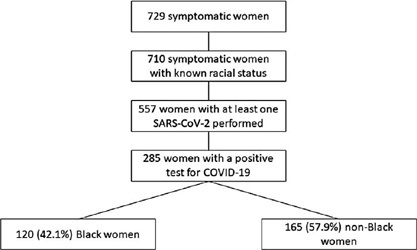
To evaluate the impact of the race (Black versus non-Black) on maternal and perinatal outcomes of pregnant women with COVID-19 in Brazil. Methods This is a subanalysis of REBRACO, a Brazilian multicenter cohort study designed to evaluate the impact of COVID-19 on pregnant women. From February2020 until February 2021, 15 maternity hospitals in Brazil collected data on women with respiratory symptoms. We selected all women with a positive test for COVID-19; then, we divided them into two groups: Black and non-Black women. Finally, we compared, between groups, sociodemographic, maternal, and perinatal outcomes. We obtained the frequency of events in each group and compared them using X2 test; p-values < 0.05 were considered significant. We also estimated the odds ratio (OR) and confidence intervals (CI).
729 symptomatic women were included in the study; of those, 285 were positive for COVID-19, 120 (42.1%) were Black, and 165 (57.9%) were non-Black. Black women had worse education (p = 0.037). The timing of access to the health system was similar between both groups, with 26.3% being included with seven or more days of symptoms. Severe acute respiratory syndrome (OR 2.22 CI 1.17–4.21), intensive care unit admission (OR 2.00 CI 1.07–3.74), and desaturation at admission (OR 3.72 CI 1.41–9.84) were more likely to occur among Black women. Maternal death was higher among Black women (7.8% vs. 2.6%, p = 0.048). Perinatal outcomes were similar between both groups.
Brazilian Black women were more likely to die due to the consequences of COVID-19.
Summary
Rev Bras Ginecol Obstet. 2023;45(5):253-260
To evaluate the impact of the race (Black versus non-Black) on maternal and perinatal outcomes of pregnant women with COVID-19 in Brazil. Methods This is a subanalysis of REBRACO, a Brazilian multicenter cohort study designed to evaluate the impact of COVID-19 on pregnant women. From February2020 until February 2021, 15 maternity hospitals in Brazil collected data on women with respiratory symptoms. We selected all women with a positive test for COVID-19; then, we divided them into two groups: Black and non-Black women. Finally, we compared, between groups, sociodemographic, maternal, and perinatal outcomes. We obtained the frequency of events in each group and compared them using X2 test; p-values < 0.05 were considered significant. We also estimated the odds ratio (OR) and confidence intervals (CI).
729 symptomatic women were included in the study; of those, 285 were positive for COVID-19, 120 (42.1%) were Black, and 165 (57.9%) were non-Black. Black women had worse education (p = 0.037). The timing of access to the health system was similar between both groups, with 26.3% being included with seven or more days of symptoms. Severe acute respiratory syndrome (OR 2.22 CI 1.17–4.21), intensive care unit admission (OR 2.00 CI 1.07–3.74), and desaturation at admission (OR 3.72 CI 1.41–9.84) were more likely to occur among Black women. Maternal death was higher among Black women (7.8% vs. 2.6%, p = 0.048). Perinatal outcomes were similar between both groups.
Brazilian Black women were more likely to die due to the consequences of COVID-19.