You searched for:"Edward Araujo Júnior"
We found (57) results for your search.Summary
Rev Bras Ginecol Obstet. 2022;44(2):118-124
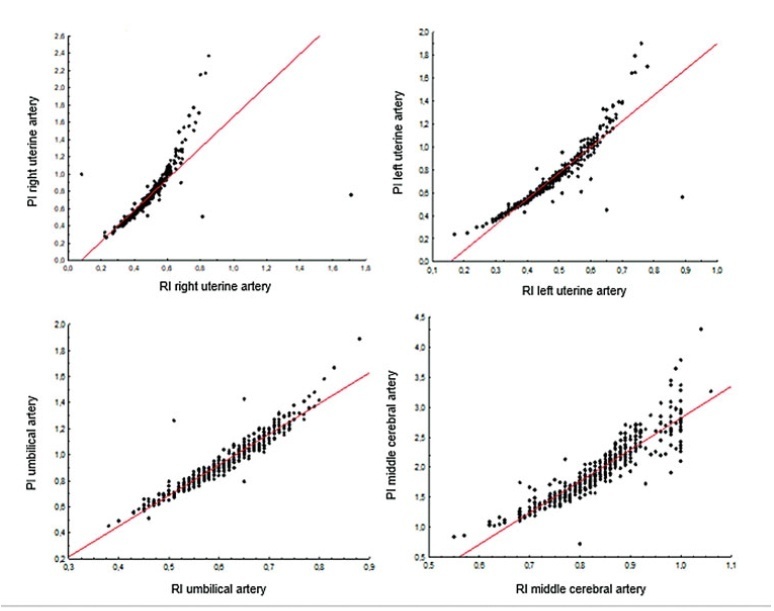
To assess the degree of correlation/agreement of maternal-fetal Doppler parameters between normal and growth-restricted fetuses (fetal growth restriction [FGR]).
The present observational and retrospective study included 274 singleton pregnancies. The following maternal-fetal Doppler parameters were assessed: uterine artery (UAt), umbilical artery (UA), middle cerebral artery (MCA), cerebroplacental ratio (CPR), and umbilical-cerebral ratio (U/C). The assessment of FGR was based on the Figueiras and Gratacós9 criteria. Spearman correlation coefficients were estimated to assess the correlation between resistance (RI) and pulsatility (PI) indices of Doppler parameters. The agreement between two Doppler parameters was assessed by the Kappa coefficient.
In total, 502 Doppler examinations were included, and FGR was observed in 19 out of 274 fetuses. A strong correlation was observed between RI and PI of UAt, UA, and MCA in all of the samples (p<0.001). Of the 502 Doppler examinations, there was agreement between U/C and CPR percentiles for 480 (95.6%) and disagreement for 22 (4.4%), with Kappa coefficient of 0.26, thereby corresponding to weak agreement. Of the 68 cases with estimated fetal weight ≤ 9th percentile (small for gestational age [SGA]), there was agreement between U/C>1.0 and CPR<5th percentile in 61 (88.4%) and disagreement in 7 (5.8%) with Kappa coefficient of 0.49, thereby corresponding to moderate agreement.
Strong correlation was observed among RI and PI UAt, UA, and MCA Doppler examinations in the present study; however, weak agreement was observed between U/C and CPR in the normal and FGR fetuses. In SGA, U/C and CPR demonstrated moderate agreement.
Summary
Rev Bras Ginecol Obstet. 2022;44(2):118-124
To assess the degree of correlation/agreement of maternal-fetal Doppler parameters between normal and growth-restricted fetuses (fetal growth restriction [FGR]).
The present observational and retrospective study included 274 singleton pregnancies. The following maternal-fetal Doppler parameters were assessed: uterine artery (UAt), umbilical artery (UA), middle cerebral artery (MCA), cerebroplacental ratio (CPR), and umbilical-cerebral ratio (U/C). The assessment of FGR was based on the Figueiras and Gratacós9 criteria. Spearman correlation coefficients were estimated to assess the correlation between resistance (RI) and pulsatility (PI) indices of Doppler parameters. The agreement between two Doppler parameters was assessed by the Kappa coefficient.
In total, 502 Doppler examinations were included, and FGR was observed in 19 out of 274 fetuses. A strong correlation was observed between RI and PI of UAt, UA, and MCA in all of the samples (p<0.001). Of the 502 Doppler examinations, there was agreement between U/C and CPR percentiles for 480 (95.6%) and disagreement for 22 (4.4%), with Kappa coefficient of 0.26, thereby corresponding to weak agreement. Of the 68 cases with estimated fetal weight ≤ 9th percentile (small for gestational age [SGA]), there was agreement between U/C>1.0 and CPR<5th percentile in 61 (88.4%) and disagreement in 7 (5.8%) with Kappa coefficient of 0.49, thereby corresponding to moderate agreement.
Strong correlation was observed among RI and PI UAt, UA, and MCA Doppler examinations in the present study; however, weak agreement was observed between U/C and CPR in the normal and FGR fetuses. In SGA, U/C and CPR demonstrated moderate agreement.
Summary
Rev Bras Ginecol Obstet. 2023;45(3):127-133
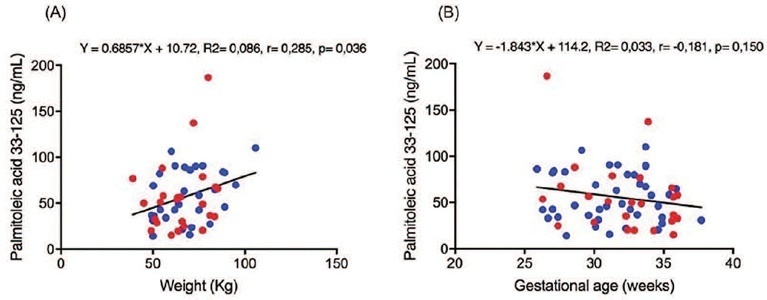
To assess the maternal blood levels of fatty acids (FAs) in pregnancies with fetal growth restriction (FGR).
This prospective cross-sectional study included pregnant women with gestational age between 26 and 37 + 6 weeks with FGR and appropriate for gestational age (AGA) fetuses. The levels of saturated, trans, monounsaturated, and polyunsaturated FAs were measured using centrifugation and liquid chromatography. The Student’s t-test, Mann-Whitney test, and general linear model, with gestational age and maternal weight as covariants, were used to compare FA levels and the FGR and AGA groups. The Chi-square was used to evaluate the association between groups and studied variables.
Maternal blood sample was collected from 64 pregnant women, being 24 FGR and 40 AGA. A weak positive correlation was found between the palmitoleic acid level and maternal weight (r = 0.285, p = 0.036). A weak negative correlation was found between the gamma-linoleic acid level and gestational age (r = −0.277, p = 0.026). The median of the elaidic acid level (2.3 vs. 4.7ng/ml, p = 0.045) and gamma-linoleic acid (6.3 vs. 6.6ng/ml, p = 0.024) was significantly lower in the FGR than the AGA group. The palmitoleic acid level was significantly higher in the FGR than AGA group (50.5 vs. 47.6ng/ml, p = 0.033).
Pregnant women with FGR had lower elaidic acid and gamma-linoleic acid levels and higher palmitoleic acid levels than AGA fetuses.
Summary
Rev Bras Ginecol Obstet. 2023;45(3):127-133
To assess the maternal blood levels of fatty acids (FAs) in pregnancies with fetal growth restriction (FGR).
This prospective cross-sectional study included pregnant women with gestational age between 26 and 37 + 6 weeks with FGR and appropriate for gestational age (AGA) fetuses. The levels of saturated, trans, monounsaturated, and polyunsaturated FAs were measured using centrifugation and liquid chromatography. The Student’s t-test, Mann-Whitney test, and general linear model, with gestational age and maternal weight as covariants, were used to compare FA levels and the FGR and AGA groups. The Chi-square was used to evaluate the association between groups and studied variables.
Maternal blood sample was collected from 64 pregnant women, being 24 FGR and 40 AGA. A weak positive correlation was found between the palmitoleic acid level and maternal weight (r = 0.285, p = 0.036). A weak negative correlation was found between the gamma-linoleic acid level and gestational age (r = −0.277, p = 0.026). The median of the elaidic acid level (2.3 vs. 4.7ng/ml, p = 0.045) and gamma-linoleic acid (6.3 vs. 6.6ng/ml, p = 0.024) was significantly lower in the FGR than the AGA group. The palmitoleic acid level was significantly higher in the FGR than AGA group (50.5 vs. 47.6ng/ml, p = 0.033).
Pregnant women with FGR had lower elaidic acid and gamma-linoleic acid levels and higher palmitoleic acid levels than AGA fetuses.
Summary
Rev Bras Ginecol Obstet. 2014;36(4):143-145
DOI 10.1590/S0100-7203201400040001
Summary
Rev Bras Ginecol Obstet. 2014;36(4):143-145
DOI 10.1590/S0100-7203201400040001
Summary
Rev Bras Ginecol Obstet. 2015;37(4):149-151
DOI 10.1590/SO100-720320150005250
Summary
Rev Bras Ginecol Obstet. 2015;37(4):149-151
DOI 10.1590/SO100-720320150005250

Summary
Rev Bras Ginecol Obstet. 2007;29(3):165-165
Summary
Rev Bras Ginecol Obstet. 2007;29(3):165-165
Summary
Rev Bras Ginecol Obstet. 2019;41(1):17-23
To assess and compare the sensitivity and specificity of ultrasonography and magnetic resonance imaging in the diagnosis of placenta accreta in patients with placenta previa.
This retrospective cohort study included 37 women, and was conducted between January 2013 and October 2015; 16 out of the 37 women suffered from placenta accreta. Histopathology was considered the gold standard for the diagnosis of placenta accreta; in its absence, a description of the intraoperative findings was used. The associations among the variables were investigated using the Pearson chi-squared test and the Mann-Whitney U-test.
The mean age of the patients was 31.8 ± 7.3 years, the mean number of pregnancies was 2.8 ± 1.1, the mean number of births was 1.4 ± 0.7, and the mean number of previous cesarean sections was 1.2 ± 0.8. Patients with placenta accreta had a higher frequency of history of cesarean section than those without it (63.6% versus 36.4% respectively; p < 0.001). The mean gestational age at birth among women diagnosed with placenta previa accreta was 35.4 ± 1.1 weeks. The mean birth weight was 2,635.9 ± 374.1 g. The sensitivity of the ultrasound was 87.5%, with a positive predictive value (PPV) of 65.1%, and a negative predictive value (NPV) of 75.0%. The sensitivity of the magnetic resonance imaging was 92.9%, with a PPV of
The ultrasound and the magnetic resonance imaging showed similar sensitivity and specificity for the diagnosis of placenta accreta.
Summary
Rev Bras Ginecol Obstet. 2019;41(1):17-23
To assess and compare the sensitivity and specificity of ultrasonography and magnetic resonance imaging in the diagnosis of placenta accreta in patients with placenta previa.
This retrospective cohort study included 37 women, and was conducted between January 2013 and October 2015; 16 out of the 37 women suffered from placenta accreta. Histopathology was considered the gold standard for the diagnosis of placenta accreta; in its absence, a description of the intraoperative findings was used. The associations among the variables were investigated using the Pearson chi-squared test and the Mann-Whitney U-test.
The mean age of the patients was 31.8 ± 7.3 years, the mean number of pregnancies was 2.8 ± 1.1, the mean number of births was 1.4 ± 0.7, and the mean number of previous cesarean sections was 1.2 ± 0.8. Patients with placenta accreta had a higher frequency of history of cesarean section than those without it (63.6% versus 36.4% respectively; p < 0.001). The mean gestational age at birth among women diagnosed with placenta previa accreta was 35.4 ± 1.1 weeks. The mean birth weight was 2,635.9 ± 374.1 g. The sensitivity of the ultrasound was 87.5%, with a positive predictive value (PPV) of 65.1%, and a negative predictive value (NPV) of 75.0%. The sensitivity of the magnetic resonance imaging was 92.9%, with a PPV of
The ultrasound and the magnetic resonance imaging showed similar sensitivity and specificity for the diagnosis of placenta accreta.
Summary
Rev Bras Ginecol Obstet. 2020;42(4):174-180
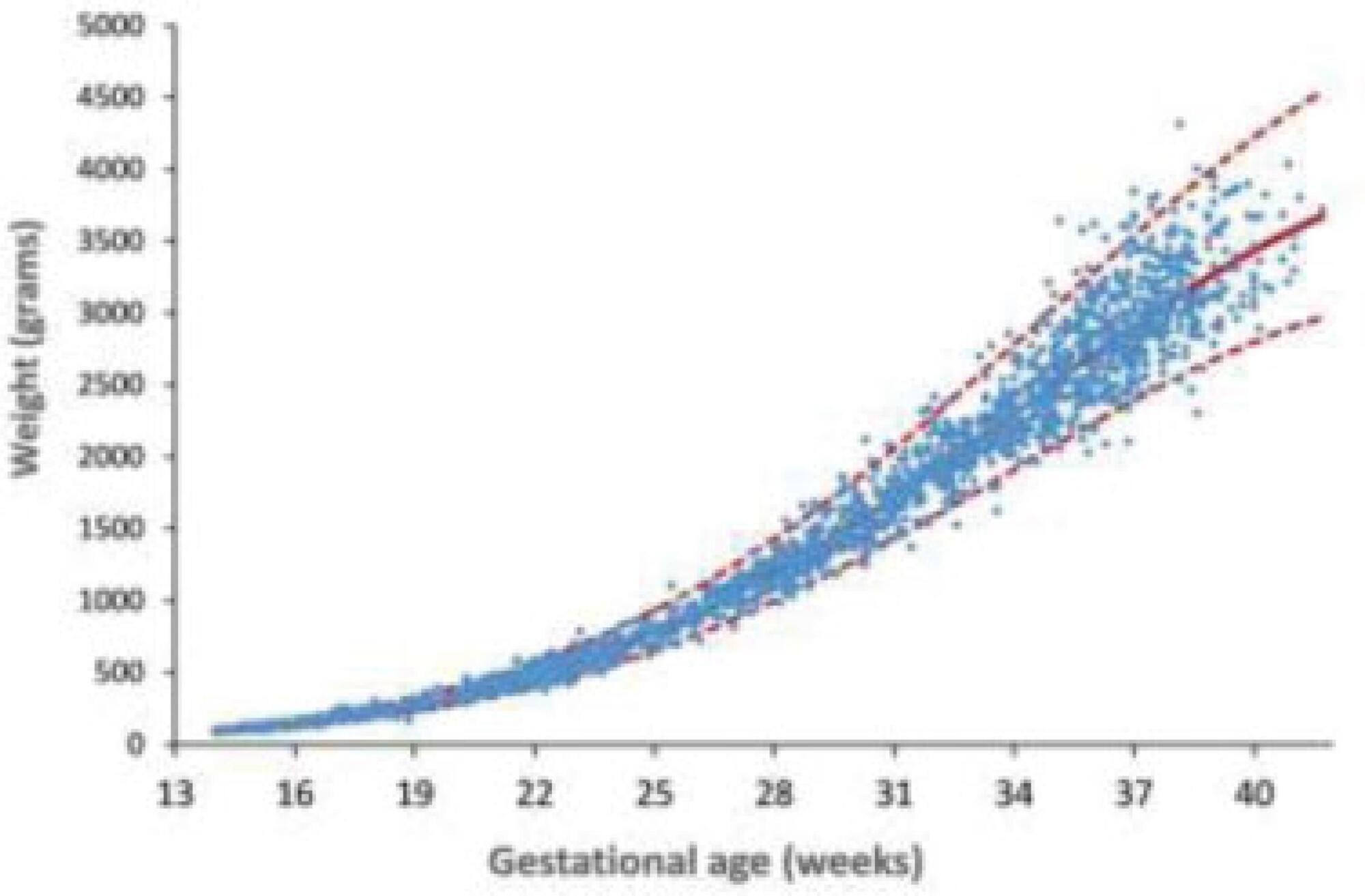
To develop reference curves of estimated fetal weight for a local population in Curitiba, South of Brazil, and compare them with the curves established for other populations.
An observational, cross-sectional, retrospective study was conducted. A reference model for estimated fetal weight was developed using a local sample of 2,211 singleton pregnancies with low risk of growth disorders and well-defined gestational age. This model was compared graphically with the Hadlock and Intergrowth 21st curves.
Reference curves for estimated fetal weight were developed for a local population. The coefficient of determination was R2 = 99.11%, indicating that 99.11% of the fetal weight variations were explained by the model. Compared with Hadlock curves, the 50th, 90th, and 97th percentiles in this model were lower, whereas the 10th percentile nearly overlapped, and the 3rd percentile was slightly higher in the proposed model. The percentiles were higher in the proposed model compared with the Intergrowth 21st curves, particularly for the 3rd, 10th, and 50th percentiles.
We provide a local reference curve for estimated fetal weight. The proposed model was different from other models, and these differences might be due to the use of different populations for model construction.
Summary
Rev Bras Ginecol Obstet. 2020;42(4):174-180
To develop reference curves of estimated fetal weight for a local population in Curitiba, South of Brazil, and compare them with the curves established for other populations.
An observational, cross-sectional, retrospective study was conducted. A reference model for estimated fetal weight was developed using a local sample of 2,211 singleton pregnancies with low risk of growth disorders and well-defined gestational age. This model was compared graphically with the Hadlock and Intergrowth 21st curves.
Reference curves for estimated fetal weight were developed for a local population. The coefficient of determination was R2 = 99.11%, indicating that 99.11% of the fetal weight variations were explained by the model. Compared with Hadlock curves, the 50th, 90th, and 97th percentiles in this model were lower, whereas the 10th percentile nearly overlapped, and the 3rd percentile was slightly higher in the proposed model. The percentiles were higher in the proposed model compared with the Intergrowth 21st curves, particularly for the 3rd, 10th, and 50th percentiles.
We provide a local reference curve for estimated fetal weight. The proposed model was different from other models, and these differences might be due to the use of different populations for model construction.
Summary
Rev Bras Ginecol Obstet. 2020;42(4):181-187
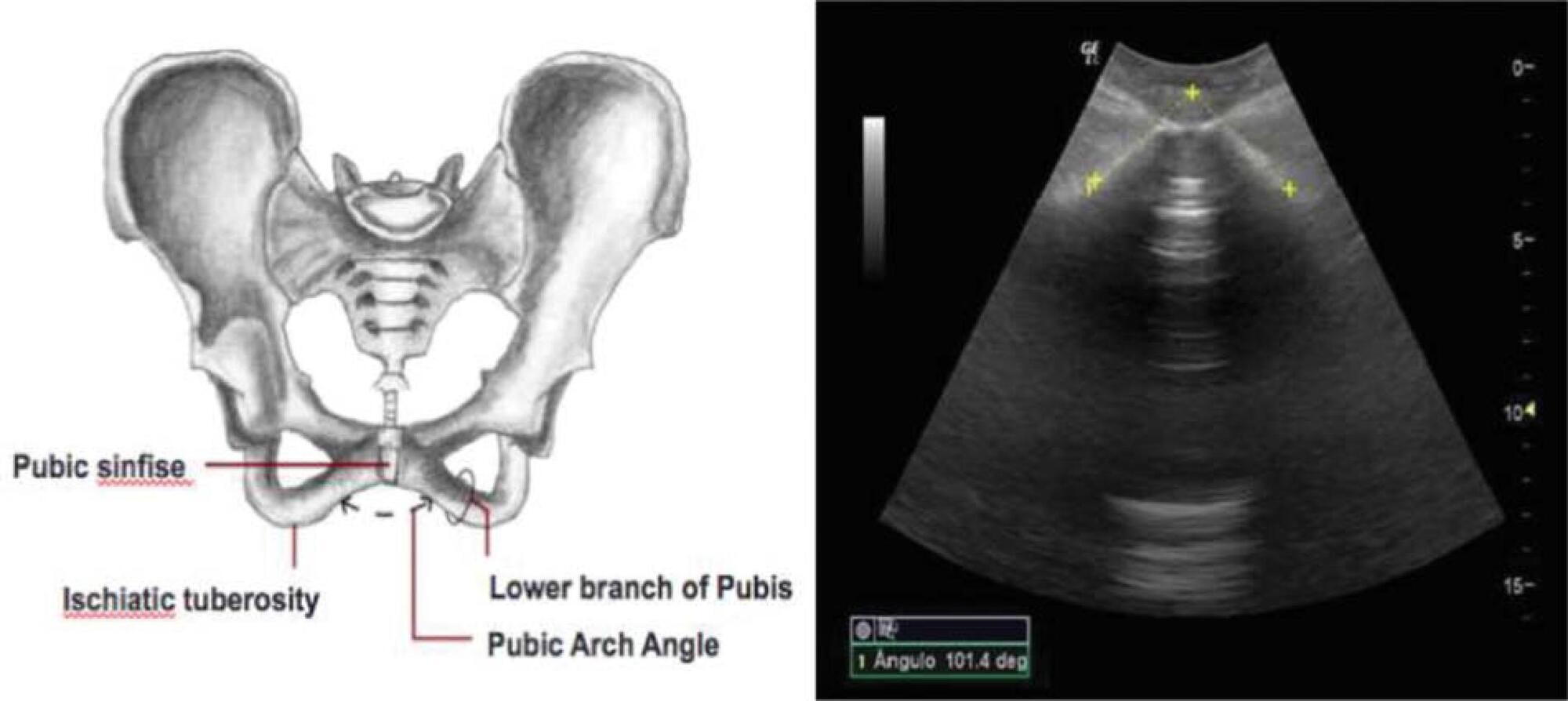
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.
Summary
Rev Bras Ginecol Obstet. 2020;42(4):181-187
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.