You searched for:"Carlos Augusto Alencar Júnior"
We found (20) results for your search.Summary
Rev Bras Ginecol Obstet. 2011;33(11):361-366
DOI 10.1590/S0100-72032011001100007
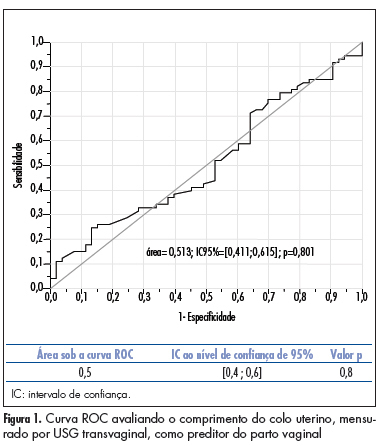
PURPOSE: to compare the accuracy of transvaginal ultrasonographic measurement of the uterine cervix with Bishop’s score for the prediction of vaginal delivery after labor induction, with 25 mcg of misoprostol. METHODS: a prospective study for the validation of a diagnostic test was conducted on 126 pregnant women with indication for labor induction. The patients were evaluated by Bishop’s score and transvaginal ultrasonography for cervical measurement. They also undergone obstetric transabdominal ultrasound to evaluate static and fetal weight, as well as the amniotic fluid index, and basal cardiotocography for the evaluation of fetal vitality. Labor was induced with vaginal and sublingual misoprostol, one of the tablets containing 25 mcg of the drug and the other only placebo. The tablets were administered every six hours, with a maximum number of eight. Frequency tables were obtained, and measures of central tendency and dispersion were calculated. ROC curves were constructed for the evaluation of Bishop’s score and ultrasonographic measurement of the uterine cervix for the prediction of vaginal delivery. RESULTS: the area under the ROC curve was 0.5 (p=0.8) for the ultrasonographic measurement of the uterine cervix, and 0.6 (p=0.02) for Bishop’s score (cut point ³4). Bishop’s score had a sensitivity of 56.2% and specificity of 67.9% for prediction of vaginal delivery, with a positive likelihood ratio of 1.75 and a negative one of 0.65. CONCLUSIONS: ultrasonographic measurement of the uterine cervix was not a good predictor of evolution to vaginal delivery among patients with misoprostol-induced labor. Bishop’s score was a better predictor of vaginal delivery under these circumstances.
Summary
Rev Bras Ginecol Obstet. 2011;33(11):361-366
DOI 10.1590/S0100-72032011001100007
PURPOSE: to compare the accuracy of transvaginal ultrasonographic measurement of the uterine cervix with Bishop’s score for the prediction of vaginal delivery after labor induction, with 25 mcg of misoprostol. METHODS: a prospective study for the validation of a diagnostic test was conducted on 126 pregnant women with indication for labor induction. The patients were evaluated by Bishop’s score and transvaginal ultrasonography for cervical measurement. They also undergone obstetric transabdominal ultrasound to evaluate static and fetal weight, as well as the amniotic fluid index, and basal cardiotocography for the evaluation of fetal vitality. Labor was induced with vaginal and sublingual misoprostol, one of the tablets containing 25 mcg of the drug and the other only placebo. The tablets were administered every six hours, with a maximum number of eight. Frequency tables were obtained, and measures of central tendency and dispersion were calculated. ROC curves were constructed for the evaluation of Bishop’s score and ultrasonographic measurement of the uterine cervix for the prediction of vaginal delivery. RESULTS: the area under the ROC curve was 0.5 (p=0.8) for the ultrasonographic measurement of the uterine cervix, and 0.6 (p=0.02) for Bishop’s score (cut point ³4). Bishop’s score had a sensitivity of 56.2% and specificity of 67.9% for prediction of vaginal delivery, with a positive likelihood ratio of 1.75 and a negative one of 0.65. CONCLUSIONS: ultrasonographic measurement of the uterine cervix was not a good predictor of evolution to vaginal delivery among patients with misoprostol-induced labor. Bishop’s score was a better predictor of vaginal delivery under these circumstances.
Summary
Rev Bras Ginecol Obstet. 2006;28(7):377-379
Summary
Rev Bras Ginecol Obstet. 2006;28(7):377-379
Summary
Rev Bras Ginecol Obstet. 2000;22(6):381-384
DOI 10.1590/S0100-72032000000600009
Parkinson's disease is characterized by tremor, stiffness of the musculature, bradykinesia, and postural and march abnormalities. It attacks all ethnic groups, with no sex preference, frequently in the 45-50-year range. The diagnosis is essentially clinical. The association with pregnancy is rare. The experience with that association is scarse, some questions remaining without answer. The authors describe a case of Parkinson's disease and gestation with satisfactory evolution, in spite of the clinical worsening during pregnancy. The mother presented elevation of blood pressure levels, alterations of the hepatic enzymes, and oligohydramnios. She used, independently, selegiline until the third month, and, later on, amantadine. The newborn presented low weight, respiratory distress and jaundice, being discharged from the hospital, with no other complications, on the fourth day of life.
Summary
Rev Bras Ginecol Obstet. 2000;22(6):381-384
DOI 10.1590/S0100-72032000000600009
Parkinson's disease is characterized by tremor, stiffness of the musculature, bradykinesia, and postural and march abnormalities. It attacks all ethnic groups, with no sex preference, frequently in the 45-50-year range. The diagnosis is essentially clinical. The association with pregnancy is rare. The experience with that association is scarse, some questions remaining without answer. The authors describe a case of Parkinson's disease and gestation with satisfactory evolution, in spite of the clinical worsening during pregnancy. The mother presented elevation of blood pressure levels, alterations of the hepatic enzymes, and oligohydramnios. She used, independently, selegiline until the third month, and, later on, amantadine. The newborn presented low weight, respiratory distress and jaundice, being discharged from the hospital, with no other complications, on the fourth day of life.
Summary
Rev Bras Ginecol Obstet. 2001;23(6):383-390
DOI 10.1590/S0100-72032001000600007
Purpose: to evaluate the ultrasonographic parameters associated with perinatal mortality increase in cases of fetal hydrocephalus. Method: 45 cases of fetal hydrocephalus were followed-up between January 1996 and December 1999. Fetal hydrocephalus was diagnosed when the ratio of lateral ventricles and the corresponding cerebral hemispheres was above 0.35 or when the measurement of the atrium of the lateral ventricles was above 10 mm. In all examinations the type of hydrocephalus, severity, symmetry, evolution and time of diagnosis were defined. The patients were submitted to morphologic ultrasound in the search of other anatomical abnormalities. The amniotic fluid index and fetal deaths were registered. The main ultrasonographic findings were correlated with perinatal mortality. For statistical analysis, chi² test and exact Fisher test were used. The value of p<0,05 was considered to be significant. Results: a total of 20 deaths were observed (44.4%), 6 occurred intra-uterus and 14 in the neonatal period. The diagnosis of hydrocephalus was established at a mean gestational age of 29 weeks. There was no association between perinatal mortality and alterations in the amniotic fluid volume, time of diagnosis, symmetry and type of hydrocephalus and the presence of other intra- or extracranial anomalies. On the other hand, the severity of the disease was associated significantly with perinatal death (p<0.0001). Conclusion: among all the analyzed ultrasonographic parameters, only the severity of hydrocephalus presented statistical association with perinatal death.
Summary
Rev Bras Ginecol Obstet. 2001;23(6):383-390
DOI 10.1590/S0100-72032001000600007
Purpose: to evaluate the ultrasonographic parameters associated with perinatal mortality increase in cases of fetal hydrocephalus. Method: 45 cases of fetal hydrocephalus were followed-up between January 1996 and December 1999. Fetal hydrocephalus was diagnosed when the ratio of lateral ventricles and the corresponding cerebral hemispheres was above 0.35 or when the measurement of the atrium of the lateral ventricles was above 10 mm. In all examinations the type of hydrocephalus, severity, symmetry, evolution and time of diagnosis were defined. The patients were submitted to morphologic ultrasound in the search of other anatomical abnormalities. The amniotic fluid index and fetal deaths were registered. The main ultrasonographic findings were correlated with perinatal mortality. For statistical analysis, chi² test and exact Fisher test were used. The value of p<0,05 was considered to be significant. Results: a total of 20 deaths were observed (44.4%), 6 occurred intra-uterus and 14 in the neonatal period. The diagnosis of hydrocephalus was established at a mean gestational age of 29 weeks. There was no association between perinatal mortality and alterations in the amniotic fluid volume, time of diagnosis, symmetry and type of hydrocephalus and the presence of other intra- or extracranial anomalies. On the other hand, the severity of the disease was associated significantly with perinatal death (p<0.0001). Conclusion: among all the analyzed ultrasonographic parameters, only the severity of hydrocephalus presented statistical association with perinatal death.
Summary
Rev Bras Ginecol Obstet. 2006;28(7):410-415
DOI 10.1590/S0100-72032006000700006
PURPOSE: to verify, through pelvic ultrasound, the existence of changes in the internal genitalia of girls with central precocious puberty, submitted to treatment with gonadotrophin-releasing hormone (GnRH) analogs. METHODS: pelvic ultrasound was performed in 18 girls with idiopathic central precocious puberty, before and after three months of onset of the treatment with GnRH analogs, to investigate the impact of the therapy on the internal genitalia. Ovarian and uterine volumes, uterine longitudinal length, relation between the longitudinal diameter of the uterine corpus and the uterine cervix, the relation between the anterior-posterior diameter of the uterine corpus and the uterine cervix, and endometrial echogenicity were evaluated. Statistical analysis was performed through Shapiro-Willkis's test, to assess data normality. When normality was present, Student's test t was applied. For data without normality, a non-parametric test (the signal test) was used. RESULTS: after therapy, statistically significant decline of the mean uterine volume (from 5.4 cm³ to 3.0 cm³, p<0.001), of the mean ovarian volume (from 2.2 cm³ to 1.1 cm³, p= 0.004), of the mean uterine longitudinal length (from 4.2cm to 3.4 cm, p=0.001), and of the mean endometrial echogenicity (from 1.8 mm to 0.6 mm, p=0.018) occurred. CONCLUSION: In girls with idiopathic central precocious puberty, pelvic ultrasound is a valid method to assess the efficacy of treatment with GnRH analogs. The main parameters of the therapeutic response were the decrease of uterine and ovarian volume, of uterine longitudinal length, and atrophy or absence of endometrial echogenicity.
Summary
Rev Bras Ginecol Obstet. 2006;28(7):410-415
DOI 10.1590/S0100-72032006000700006
PURPOSE: to verify, through pelvic ultrasound, the existence of changes in the internal genitalia of girls with central precocious puberty, submitted to treatment with gonadotrophin-releasing hormone (GnRH) analogs. METHODS: pelvic ultrasound was performed in 18 girls with idiopathic central precocious puberty, before and after three months of onset of the treatment with GnRH analogs, to investigate the impact of the therapy on the internal genitalia. Ovarian and uterine volumes, uterine longitudinal length, relation between the longitudinal diameter of the uterine corpus and the uterine cervix, the relation between the anterior-posterior diameter of the uterine corpus and the uterine cervix, and endometrial echogenicity were evaluated. Statistical analysis was performed through Shapiro-Willkis's test, to assess data normality. When normality was present, Student's test t was applied. For data without normality, a non-parametric test (the signal test) was used. RESULTS: after therapy, statistically significant decline of the mean uterine volume (from 5.4 cm³ to 3.0 cm³, p<0.001), of the mean ovarian volume (from 2.2 cm³ to 1.1 cm³, p= 0.004), of the mean uterine longitudinal length (from 4.2cm to 3.4 cm, p=0.001), and of the mean endometrial echogenicity (from 1.8 mm to 0.6 mm, p=0.018) occurred. CONCLUSION: In girls with idiopathic central precocious puberty, pelvic ultrasound is a valid method to assess the efficacy of treatment with GnRH analogs. The main parameters of the therapeutic response were the decrease of uterine and ovarian volume, of uterine longitudinal length, and atrophy or absence of endometrial echogenicity.
Summary
Rev Bras Ginecol Obstet. 2003;25(6):419-423
DOI 10.1590/S0100-72032003000600006
PURPOSE: to evaluate the perinatal outcomes of pregnancies complicated by oligohydramnios, not due to premature rupture of membranes (PRM), diagnosed until the 26th week of gestation. PATIENTS AND METHODS: we analyzed retrospectively the cases of oligohydramnios that occurred from January 1994 to December 2000, and were diagnosed until the 26th week of gestation. Oligohydramnios was present when the amniotic fluid index was less or equal to 5.0 cm. After diagnosis the patients were followed-up with serial ultrasound evaluation, with emphasis on the maintenance of the oligohydramnios state. When remission of the oligohydramnios occurred, patients remained in the study. Cases due to PRM, fetal death detected on the first examination and the women who gave birth in another institution were excluded from the study. Concerning the patients, the presence of clinical and obstetric diseases was investigated. As regards the newborns, we evaluated birth weight, time of admission/death, occurrence of death or malformations. RESULTS: twenty-seven cases of oligohydramnios were analyzed. Thirteen fetuses had congenital anomalies, and among them, eight had anomalies of the urinary tract, four of the nervous system and one had cystic hygroma. Fourteen patients had a clinical or an obstetric disease, mainly hypertension (10 cases). In addition, we found three cases of placenta previa and one case of thyropathy. There were thirteen fetal deaths and fourteen neonatal deaths. CONCLUSION: oligohydramnios not due to PRM, occurring in the second trimester of gestation, independent of the etiology or the presence of congenital anomalies, was associated with a fatal perinatal result.
Summary
Rev Bras Ginecol Obstet. 2003;25(6):419-423
DOI 10.1590/S0100-72032003000600006
PURPOSE: to evaluate the perinatal outcomes of pregnancies complicated by oligohydramnios, not due to premature rupture of membranes (PRM), diagnosed until the 26th week of gestation. PATIENTS AND METHODS: we analyzed retrospectively the cases of oligohydramnios that occurred from January 1994 to December 2000, and were diagnosed until the 26th week of gestation. Oligohydramnios was present when the amniotic fluid index was less or equal to 5.0 cm. After diagnosis the patients were followed-up with serial ultrasound evaluation, with emphasis on the maintenance of the oligohydramnios state. When remission of the oligohydramnios occurred, patients remained in the study. Cases due to PRM, fetal death detected on the first examination and the women who gave birth in another institution were excluded from the study. Concerning the patients, the presence of clinical and obstetric diseases was investigated. As regards the newborns, we evaluated birth weight, time of admission/death, occurrence of death or malformations. RESULTS: twenty-seven cases of oligohydramnios were analyzed. Thirteen fetuses had congenital anomalies, and among them, eight had anomalies of the urinary tract, four of the nervous system and one had cystic hygroma. Fourteen patients had a clinical or an obstetric disease, mainly hypertension (10 cases). In addition, we found three cases of placenta previa and one case of thyropathy. There were thirteen fetal deaths and fourteen neonatal deaths. CONCLUSION: oligohydramnios not due to PRM, occurring in the second trimester of gestation, independent of the etiology or the presence of congenital anomalies, was associated with a fatal perinatal result.
Summary
Rev Bras Ginecol Obstet. 1998;20(8):481-484
DOI 10.1590/S0100-72031998000800009
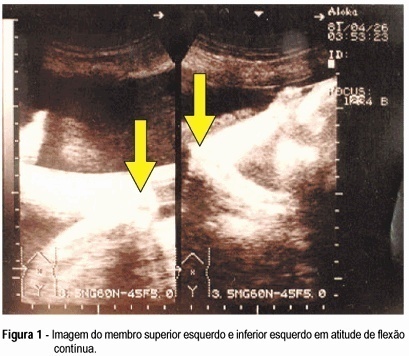
Arthrogryposis multiplex congenita is characterized by multiple joint contractures present at birth. Prenatal diagnosis is difficult. There are few reports in the literature. Fetal akinesia, abnormal limb position, intrauterine growth retardation, and polyhydramnios are the main findings of the ultrasonographic diagnosis. The authors describe a case of arthrogryposis multiplex congenita ultrasonographically diagnosed in the third gestational trimester. The main findings were absence of fetal movements, polyhydramnios, symmetrical and non-symmetrical fetal growth retardation with marked decrease of abdominal and thoracic circumference, low-set ears, micrognathia, continuous flexure contracture of limbs, internal rotation of the femur, and clubfoot on the right.
Summary
Rev Bras Ginecol Obstet. 1998;20(8):481-484
DOI 10.1590/S0100-72031998000800009
Arthrogryposis multiplex congenita is characterized by multiple joint contractures present at birth. Prenatal diagnosis is difficult. There are few reports in the literature. Fetal akinesia, abnormal limb position, intrauterine growth retardation, and polyhydramnios are the main findings of the ultrasonographic diagnosis. The authors describe a case of arthrogryposis multiplex congenita ultrasonographically diagnosed in the third gestational trimester. The main findings were absence of fetal movements, polyhydramnios, symmetrical and non-symmetrical fetal growth retardation with marked decrease of abdominal and thoracic circumference, low-set ears, micrognathia, continuous flexure contracture of limbs, internal rotation of the femur, and clubfoot on the right.
Summary
Rev Bras Ginecol Obstet. 2003;25(7):491-499
DOI 10.1590/S0100-72032003000700005
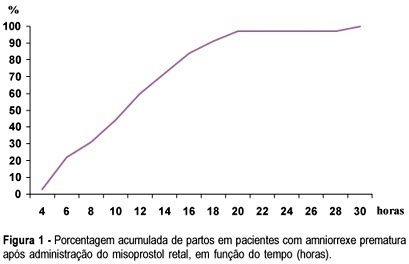
PURPOSE: to investigate whether rectally administered misoprostol is an effective method for induction of labor in patients with premature ruptured membranes at term. METHODS: a pilot trial was conducted, enrolling 32 women with alive, singleton, cephalic fetus and ruptured membranes between 36 and 41 weeks of pregnancy, with Bishop score <6 and without evidence of labor. They received rectal misoprostol (tablets of 50 mg) every 4 h until active labor was diagnosed. Patients with ruptured membranes for >18 h received antibiotics (crystalline penicillin) for prophylaxis of streptococcal infeccion. Outcomes included time from induction to labor and induction to delivery, incidence of tachysystole, mode of delivery, incidence of chorioamnionitis and neonatal outcome. Statistical analysis was performed using the public domain software Epi-Info 2002. Means and standard deviations were calculated, as well as frequency distributions. Survival analysis was performed to determine percent of deliveries according to time (hours) since the administration of the first tablet. RESULTS: the mean (±SD) induction-to-labor and induction-to-delivery intervals were 299.8±199.9 and 681±340.5 min, respectively. The frequency of tachysystole was 9.4%. About 72% of patients achieved vaginal delivery. Chorioamnionitis was diagnosed in 12.5% of the patients. Median Apgar scores at 1st and 5th min were 8 and 9, respectively. There was no case of Apgar <7 at the 5th min. Neonatal sepsis occurred in 12.5% of the neonates. CONCLUSION: induction of labor with rectal misoprostol in the setting of premature rupture of membranes was effective, with 72% of vaginal deliveries and a low rate of chorioamnionitis. These findings must be confirmed by large randomized controlled trials.
Summary
Rev Bras Ginecol Obstet. 2003;25(7):491-499
DOI 10.1590/S0100-72032003000700005
PURPOSE: to investigate whether rectally administered misoprostol is an effective method for induction of labor in patients with premature ruptured membranes at term. METHODS: a pilot trial was conducted, enrolling 32 women with alive, singleton, cephalic fetus and ruptured membranes between 36 and 41 weeks of pregnancy, with Bishop score <6 and without evidence of labor. They received rectal misoprostol (tablets of 50 mg) every 4 h until active labor was diagnosed. Patients with ruptured membranes for >18 h received antibiotics (crystalline penicillin) for prophylaxis of streptococcal infeccion. Outcomes included time from induction to labor and induction to delivery, incidence of tachysystole, mode of delivery, incidence of chorioamnionitis and neonatal outcome. Statistical analysis was performed using the public domain software Epi-Info 2002. Means and standard deviations were calculated, as well as frequency distributions. Survival analysis was performed to determine percent of deliveries according to time (hours) since the administration of the first tablet. RESULTS: the mean (±SD) induction-to-labor and induction-to-delivery intervals were 299.8±199.9 and 681±340.5 min, respectively. The frequency of tachysystole was 9.4%. About 72% of patients achieved vaginal delivery. Chorioamnionitis was diagnosed in 12.5% of the patients. Median Apgar scores at 1st and 5th min were 8 and 9, respectively. There was no case of Apgar <7 at the 5th min. Neonatal sepsis occurred in 12.5% of the neonates. CONCLUSION: induction of labor with rectal misoprostol in the setting of premature rupture of membranes was effective, with 72% of vaginal deliveries and a low rate of chorioamnionitis. These findings must be confirmed by large randomized controlled trials.