You searched for:"Alberto Borges Peixoto"
We found (11) results for your search.Summary
Rev Bras Ginecol Obstet. 2019;41(12):688-696
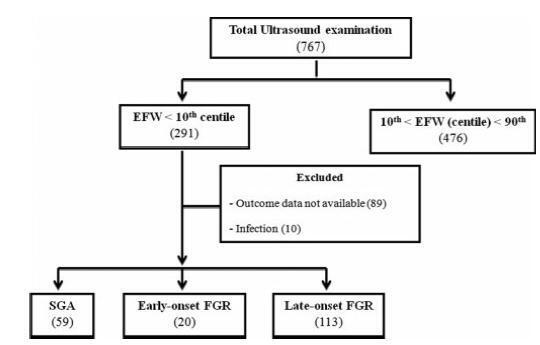
To evaluate the association between early-onset fetal growth restriction (FGR), late-onset FGR, small for gestational age (SGA) and adequate for gestational age (AGA) fetuses and adverse perinatal outcomes.
This was a retrospective longitudinal study in which 4 groups were evaluated: 1 - early-onset FGR (before 32 weeks) (n=20), 2 - late-onset FGR (at or after 32 weeks) (n=113), 3 - SGA (n=59), 4 - AGA (n=476). The Kaplan-Meier curve was used to compare the time from the diagnosis of FGR to birth. Logistic regression was used to determine the best predictors of adverse perinatal outcomes in fetuses with FGR and SGA.
A longer timebetween the diagnosis and birthwas observed forAGAthan for late FGR fetuses (p<0.001). The model including the type of FGR and the gestational age at birth was significant in predicting the risk of hospitalization in the neonatal intensive care unit (ICU) (p<0.001). The model including only the type of FGR predicted the risk of needing neonatal resuscitation (p<0.001), of respiratory distress (p<0.001), and of birth at<32, 34, and 37 weeks of gestation, respectively (p<0.001).
Fetal growth restriction and SGA were associated with adverse perinatal outcomes. The type of FGR at the moment of diagnosis was an independent variable to predict respiratory distress and the need for neonatal resuscitation. The model including both the type of FGR and the gestational age at birth predicted the risk of needing neonatal ICU hospitalization.
Summary
Rev Bras Ginecol Obstet. 2019;41(12):688-696
To evaluate the association between early-onset fetal growth restriction (FGR), late-onset FGR, small for gestational age (SGA) and adequate for gestational age (AGA) fetuses and adverse perinatal outcomes.
This was a retrospective longitudinal study in which 4 groups were evaluated: 1 - early-onset FGR (before 32 weeks) (n=20), 2 - late-onset FGR (at or after 32 weeks) (n=113), 3 - SGA (n=59), 4 - AGA (n=476). The Kaplan-Meier curve was used to compare the time from the diagnosis of FGR to birth. Logistic regression was used to determine the best predictors of adverse perinatal outcomes in fetuses with FGR and SGA.
A longer timebetween the diagnosis and birthwas observed forAGAthan for late FGR fetuses (p<0.001). The model including the type of FGR and the gestational age at birth was significant in predicting the risk of hospitalization in the neonatal intensive care unit (ICU) (p<0.001). The model including only the type of FGR predicted the risk of needing neonatal resuscitation (p<0.001), of respiratory distress (p<0.001), and of birth at<32, 34, and 37 weeks of gestation, respectively (p<0.001).
Fetal growth restriction and SGA were associated with adverse perinatal outcomes. The type of FGR at the moment of diagnosis was an independent variable to predict respiratory distress and the need for neonatal resuscitation. The model including both the type of FGR and the gestational age at birth predicted the risk of needing neonatal ICU hospitalization.
Summary
Rev Bras Ginecol Obstet. 2020;42(11):717-725
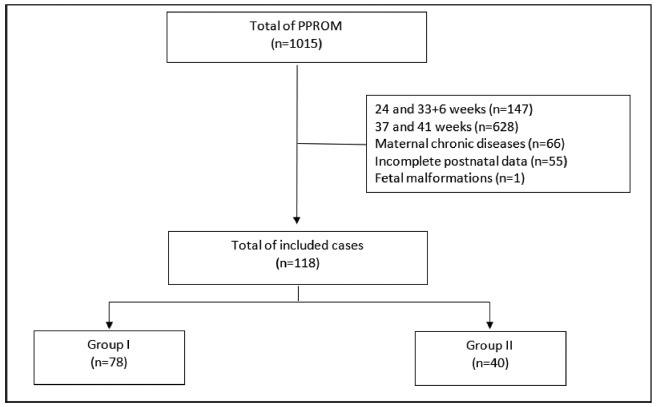
To compare the type of management (active versus expectant) for preterm premature rupture of membranes (PPROM) between 34 and 36 + 6 weeks of gestation and the associated adverse perinatal outcomes in 2 tertiary hospitals in the southeast of Brazil.
In the present retrospective cohort study, data were obtained by reviewing the medical records of patients admitted to two tertiary centers with different protocols for PPROM management. The participants were divided into two groups based on PPROM management: group I (active) and group II (expectant). For statistical analysis, the Student t-test, the chi-squared test, and binary logistic regression were used.
Of the 118 participants included, 78 underwent active (group I) and 40 expectant management (group II). Compared with group II, group I had significantly lower mean amniotic fluid index (5.5 versus 11.3 cm, p = 0.002), polymerase chain reaction at admission (1.5 versus 5.2 mg/dl, p = 0.002), time of prophylactic antibiotics (5.4 versus 18.4 hours, p < 0.001), latency time (20.9 versus 33.6 hours, p = 0.001), and gestational age at delivery (36.5 versus 37.2 weeks, p = 0.025). There were no significant associations between the groups and the presence of adverse perinatal outcomes. Gestational age at diagnosis was the only significant predictor of adverse composite outcome (x2 [1] = 3.1, p = 0.0001, R2 Nagelkerke = 0.138).
There was no association between active versus expectant management in pregnant women with PPROM between 34 and 36 + 6 weeks of gestation and adverse perinatal outcomes.
Summary
Rev Bras Ginecol Obstet. 2020;42(11):717-725
To compare the type of management (active versus expectant) for preterm premature rupture of membranes (PPROM) between 34 and 36 + 6 weeks of gestation and the associated adverse perinatal outcomes in 2 tertiary hospitals in the southeast of Brazil.
In the present retrospective cohort study, data were obtained by reviewing the medical records of patients admitted to two tertiary centers with different protocols for PPROM management. The participants were divided into two groups based on PPROM management: group I (active) and group II (expectant). For statistical analysis, the Student t-test, the chi-squared test, and binary logistic regression were used.
Of the 118 participants included, 78 underwent active (group I) and 40 expectant management (group II). Compared with group II, group I had significantly lower mean amniotic fluid index (5.5 versus 11.3 cm, p = 0.002), polymerase chain reaction at admission (1.5 versus 5.2 mg/dl, p = 0.002), time of prophylactic antibiotics (5.4 versus 18.4 hours, p < 0.001), latency time (20.9 versus 33.6 hours, p = 0.001), and gestational age at delivery (36.5 versus 37.2 weeks, p = 0.025). There were no significant associations between the groups and the presence of adverse perinatal outcomes. Gestational age at diagnosis was the only significant predictor of adverse composite outcome (x2 [1] = 3.1, p = 0.0001, R2 Nagelkerke = 0.138).
There was no association between active versus expectant management in pregnant women with PPROM between 34 and 36 + 6 weeks of gestation and adverse perinatal outcomes.
Summary
Rev Bras Ginecol Obstet. 2021;43(10):743-748
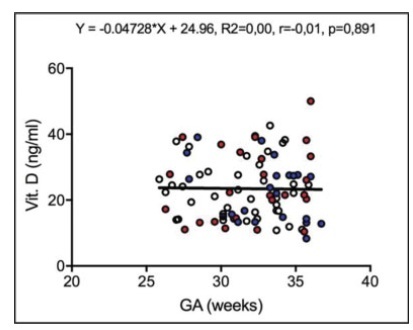
To assess maternal serum levels of vitamin D in fetuses appropriate for gestational age (AGA), small for gestational age (SGA), and with fetal growth restriction (FGR) according to estimated fetal weight (EFW).
This cross-sectional study included 87 pregnant women between 26 and 36 weeks of gestation: 38 in the AGA group, 24 in the SGA group, and 25 in the FGR group. Maternal serum vitamin D levels were assessed using the chemiluminescence method. The Fisher exact test was used to compare the results between the groups.
The mean ± standard deviation (SD) of maternal age (years) and body mass index (kg/m2) in the AGA, SGA, and FGR groups were 25.26 8.40 / 26.57 ± 4.37; 25.04 ± 8.44 / 26.09 ± 3.94; and 25.48 ± 7.52 / 26.24 ± 4.66, respectively (p > 0.05). The maternal serum vitamin D levels (mean ± SD) of the AGA, SGA, and FGR groups were 22.47 ± 8.35 ng/mL, 24.80 ± 10.76 ng/mL, and 23.61 ± 9.98 ng/mL, respectively, but without significant differences between the groups (p = 0.672).
Maternal serum vitamin D levels did not present significant differences among pregnant women with AGA, SGA, or FGR fetuses between 26 and 36 weeks of gestation according to EFW.
Summary
Rev Bras Ginecol Obstet. 2021;43(10):743-748
To assess maternal serum levels of vitamin D in fetuses appropriate for gestational age (AGA), small for gestational age (SGA), and with fetal growth restriction (FGR) according to estimated fetal weight (EFW).
This cross-sectional study included 87 pregnant women between 26 and 36 weeks of gestation: 38 in the AGA group, 24 in the SGA group, and 25 in the FGR group. Maternal serum vitamin D levels were assessed using the chemiluminescence method. The Fisher exact test was used to compare the results between the groups.
The mean ± standard deviation (SD) of maternal age (years) and body mass index (kg/m2) in the AGA, SGA, and FGR groups were 25.26 8.40 / 26.57 ± 4.37; 25.04 ± 8.44 / 26.09 ± 3.94; and 25.48 ± 7.52 / 26.24 ± 4.66, respectively (p > 0.05). The maternal serum vitamin D levels (mean ± SD) of the AGA, SGA, and FGR groups were 22.47 ± 8.35 ng/mL, 24.80 ± 10.76 ng/mL, and 23.61 ± 9.98 ng/mL, respectively, but without significant differences between the groups (p = 0.672).
Maternal serum vitamin D levels did not present significant differences among pregnant women with AGA, SGA, or FGR fetuses between 26 and 36 weeks of gestation according to EFW.