Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(5):347-350
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(5):347-350
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(6):347-347
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(6):347-347
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(6):347-350
DOI 10.1590/S0100-72031999000600008
Purpose: to evaluate safety and efficacy of intra-amniotic injection of methotrexate (MTX) for treatment of viable cervical pregnancy. Methods: four women with viable cervical pregnancy confirmed by ultrasound (US) were treated with transvaginal injection of MTX (1 mg/kg) under sonographic control. The follow-up was made with serial dosages of beta-hCG on days 1, 4 and 7 after injection and weekly until the titers were negative. Results: the patients were treated with success. The time for the titers of beta-hCG to become negative after the treatment was: 62 days (case 1), 84 days (case 2), 28 days (case 3) and 10 days (case 4). Conclusion: intra-amniotic injection of MTX can be used to avoid surgery in cases of viable cervical pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(6):347-350
DOI 10.1590/S0100-72031999000600008
Purpose: to evaluate safety and efficacy of intra-amniotic injection of methotrexate (MTX) for treatment of viable cervical pregnancy. Methods: four women with viable cervical pregnancy confirmed by ultrasound (US) were treated with transvaginal injection of MTX (1 mg/kg) under sonographic control. The follow-up was made with serial dosages of beta-hCG on days 1, 4 and 7 after injection and weekly until the titers were negative. Results: the patients were treated with success. The time for the titers of beta-hCG to become negative after the treatment was: 62 days (case 1), 84 days (case 2), 28 days (case 3) and 10 days (case 4). Conclusion: intra-amniotic injection of MTX can be used to avoid surgery in cases of viable cervical pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(8):347-352
DOI 10.1590/SO100-720320150005209
To investigate the association of the HLA-A, -B and -DRB1 alleles with the occurrence of Recurrent Spontaneous Abortion.
A case-control study of 200 women aged 18 to 35 years, consisting of a convenience sample of 100 women who had idiopathic recurrent spontaneous abortion and 100 women without abortion and with two or more children. Peripheral blood genomic DNA was extracted from 500l of Buffy Coat stored at -20°C. HLA typing was performed by the PCR-SSOP method (Polymerase Chain Reaction - Specific Sequence of Oligonucleotides Probes, One Lambda(r), CA, USA). The regions of the amplified DNA were exon 2 and 3 for the A and B loci and only exon 3 for the DRB1 locus. The HLA FUSIONTM program (One Lambda, Canoga Park, CA, USA, version 3.0) was used for HLA-A, HLA-B and HLA-DRB1 genotyping. Absolute frequencies and percentages and calculation of mean and standard deviation were used for standard statistical analysis. The qualitative variables were compared by the χ2 test with Yates correction or by Fisher's exact test. The odds ratio with the 95%CI was used for the comparisons, with the level of significance set at p<0.05.
The frequency of the A*34 allele was significantly higher in the case group compared to control (4.0 versus 0.5%; p<0.05). Alleles A*24 (6.0 versus 12.5%; p<0.05) and B*35 (8.0 versus 20.5%; p<0.05) were significantly less frequent in the case group. Among the class II alleles, DRB1*03 showed a slightly higher frequency in the case group (11.0 versus 5.5%, p = 0.056).
It was shown that the HLA-A*34 allele is a risk factor for recurrent spontaneous abortion, while the HLA-A*24 and HLA-B*35 alleles are associated with protection, and no allele of the DRB1 locus was associated with RSA.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(8):347-352
DOI 10.1590/SO100-720320150005209
To investigate the association of the HLA-A, -B and -DRB1 alleles with the occurrence of Recurrent Spontaneous Abortion.
A case-control study of 200 women aged 18 to 35 years, consisting of a convenience sample of 100 women who had idiopathic recurrent spontaneous abortion and 100 women without abortion and with two or more children. Peripheral blood genomic DNA was extracted from 500l of Buffy Coat stored at -20°C. HLA typing was performed by the PCR-SSOP method (Polymerase Chain Reaction - Specific Sequence of Oligonucleotides Probes, One Lambda(r), CA, USA). The regions of the amplified DNA were exon 2 and 3 for the A and B loci and only exon 3 for the DRB1 locus. The HLA FUSIONTM program (One Lambda, Canoga Park, CA, USA, version 3.0) was used for HLA-A, HLA-B and HLA-DRB1 genotyping. Absolute frequencies and percentages and calculation of mean and standard deviation were used for standard statistical analysis. The qualitative variables were compared by the χ2 test with Yates correction or by Fisher's exact test. The odds ratio with the 95%CI was used for the comparisons, with the level of significance set at p<0.05.
The frequency of the A*34 allele was significantly higher in the case group compared to control (4.0 versus 0.5%; p<0.05). Alleles A*24 (6.0 versus 12.5%; p<0.05) and B*35 (8.0 versus 20.5%; p<0.05) were significantly less frequent in the case group. Among the class II alleles, DRB1*03 showed a slightly higher frequency in the case group (11.0 versus 5.5%, p = 0.056).
It was shown that the HLA-A*34 allele is a risk factor for recurrent spontaneous abortion, while the HLA-A*24 and HLA-B*35 alleles are associated with protection, and no allele of the DRB1 locus was associated with RSA.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(8):347-352
DOI 10.1590/SO100-720320140005061
To evaluate the validity of cervicovaginal cytology performed at LAPER, the main Laboratory of Pathology of the State of Roraima, Brazil, by interrater agreement (external monitoring) and agreement with histopathologic results.
One hundred women were included, a population-based convenience sample. Their cervical cytological exams were evaluated by the laboratory staff and reviewed by expert medical pathologists, external to the laboratory. Cohen's Kappa index, sensitivity and specificity were evaluated. The study was approved by LAPER coordination and Federal University of Roraima Research Ethics Commitee.
Regarding the prevalence of human papillomavirus-related atypical, there was no concordance between the results issued by LAPER and by the external pathologists (k=0.21). A low sensitivity (28.5%) and specificity (89,2%) was detected for the diagnostic performance of LAPER, with a high proportion of false positive and false negative results. The cytological reports of the external pathologists showed higher sensitivity and specificity (71.4 and 98.9%, respectively), ruling out the possibility that errors related to collection methods and staining would explain the low performance of the laboratory.
A low diagnostic accuracy of cervicovaginal cytology can be a barrier against the control of cervical cancer in Roraima. We emphasize the need for professional training and internal and external monitoring in Brazilian states with a high incidence of cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(8):347-352
DOI 10.1590/SO100-720320140005061
To evaluate the validity of cervicovaginal cytology performed at LAPER, the main Laboratory of Pathology of the State of Roraima, Brazil, by interrater agreement (external monitoring) and agreement with histopathologic results.
One hundred women were included, a population-based convenience sample. Their cervical cytological exams were evaluated by the laboratory staff and reviewed by expert medical pathologists, external to the laboratory. Cohen's Kappa index, sensitivity and specificity were evaluated. The study was approved by LAPER coordination and Federal University of Roraima Research Ethics Commitee.
Regarding the prevalence of human papillomavirus-related atypical, there was no concordance between the results issued by LAPER and by the external pathologists (k=0.21). A low sensitivity (28.5%) and specificity (89,2%) was detected for the diagnostic performance of LAPER, with a high proportion of false positive and false negative results. The cytological reports of the external pathologists showed higher sensitivity and specificity (71.4 and 98.9%, respectively), ruling out the possibility that errors related to collection methods and staining would explain the low performance of the laboratory.
A low diagnostic accuracy of cervicovaginal cytology can be a barrier against the control of cervical cancer in Roraima. We emphasize the need for professional training and internal and external monitoring in Brazilian states with a high incidence of cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):348-355
To identify the epidemiological risk factors for congenital anomalies (CAs) and the impact of these fetal malformations on the perinatal outcomes.
This prospective cohort study comprised 275 women whose fetuses had CAs. Maternal variables to establish potential risk factors for each group of CA and perinatal outcomes were evaluated. The primary outcome was CA. Secondary outcomes included: fetal growth restriction (FGR); fetal distress (FD); premature rupture of membranes (PROM); oligohydramnios or polyhydramnios; preterm delivery (PTD); stillbirth; cesarean section; low birth weight; Apgar score < 7 at the 1st and 5th minutes; need for assisted ventilation at birth; neonatal infection; need for surgical treatment; early neonatal death; and hospitalization time. Chi-square (x2) test and multilevel regression analysis were applied to compare the groups and determine the effects of maternal characteristics on the incidence of CAs.
The general prevalence of CAs was of 2.4%. Several maternal characteristics were associated to CAs, such as: age; skin color; level of education; parity; folic acid supplementation; tobacco use; and history of previous miscarriage. There were no significant differences among the CA groups in relation to FGR, FD, PROM, 1-minute Apgar score > 7, and need for assisted ventilation at birth. On the other hand, the prevalence of the other considered outcomes varied significantly among groups. Preterm delivery was significantly more frequent in gastrointestinal tract/abdominal wall defects. The stillbirth rate was increased in all CAs, mainly in isolated fetal hydrops (odds ratio [OR]: 27.13; 95% confidence interval [95%CI]: 2.90-253.47). Hospitalization time was higher for the urinary tract and congenital heart disease groups (p < 0.01). Neonatal death was significantly less frequent in the central nervous system anomalies group.
It was possible to identify several risk factors for CAs. Adverse perinatal outcomes were presented in all CA groups, and may differ according to the type of CA considered.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(5):348-351
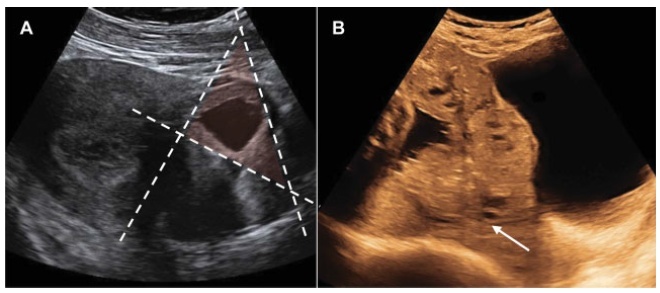
Vasa previa (VP) is a dangerous obstetric condition associated with perinatal mortality and morbidity. In vitro fertilization (IVF) is a risk factor for VP due to the high incidence of abnormal placentation. The diagnosis should be made prenatally, because fetal mortality can be extremely high. We report two cases to demonstrate the accuracy of transvaginal ultrasound in the prenatal diagnosis of VP. A 40-year-old primiparous Caucasian woman with IVF pregnancy was diagnosed with VP at 29 weeks of gestation and was hospitalized for observation at 31 weeks of gestation. She delivered a male newborn weighing 2,380 g, with an Apgar score of 10 at 5 minutes, by elective cesarean section at 34 weeks + 4 days of gestation, without complications. A 36-yearold primiparous Caucasian woman with IVF pregnancy was diagnosed with placenta previa, bilobed placenta increta and VP. The cord insertion was velamentous. She was hospitalized for observation at 26 weeks of gestation. She delivered a female newborn weighing 2,140 g, with an Apgar score of 9 at 5 minutes, by emergency cesarean section at 33 weeks + 4 days of gestation due to vaginal bleeding. The prenatal diagnosis of VP was associated with a favorable outcome in the two cases, supporting previous observations that IVF is a risk factor for VP and that all IVF pregnancies should be screened by transvaginal ultrasound.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(5):348-351
Vasa previa (VP) is a dangerous obstetric condition associated with perinatal mortality and morbidity. In vitro fertilization (IVF) is a risk factor for VP due to the high incidence of abnormal placentation. The diagnosis should be made prenatally, because fetal mortality can be extremely high. We report two cases to demonstrate the accuracy of transvaginal ultrasound in the prenatal diagnosis of VP. A 40-year-old primiparous Caucasian woman with IVF pregnancy was diagnosed with VP at 29 weeks of gestation and was hospitalized for observation at 31 weeks of gestation. She delivered a male newborn weighing 2,380 g, with an Apgar score of 10 at 5 minutes, by elective cesarean section at 34 weeks + 4 days of gestation, without complications. A 36-yearold primiparous Caucasian woman with IVF pregnancy was diagnosed with placenta previa, bilobed placenta increta and VP. The cord insertion was velamentous. She was hospitalized for observation at 26 weeks of gestation. She delivered a female newborn weighing 2,140 g, with an Apgar score of 9 at 5 minutes, by emergency cesarean section at 33 weeks + 4 days of gestation due to vaginal bleeding. The prenatal diagnosis of VP was associated with a favorable outcome in the two cases, supporting previous observations that IVF is a risk factor for VP and that all IVF pregnancies should be screened by transvaginal ultrasound.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(11):348-353
DOI 10.1590/S0100-72032011001100005
PURPOSE: To describe the obstetric outcome of women with overweight/obesity treated at the prenatal care clinic of a public maternity hospital in Rio de Janeiro. METHODS: A descriptive cross-sectional study which investigated 433 women (³20 years-old, without any chronic diseases) and their newborns treated at public hospitals in Rio de Janeiro. Information was collected from medical records and through interviews. The characteristics of mothers and newborns evaluated were divided into maternal (social habits, anthropometric measurements and clinical, obstetric, and prenatal care) and newborn groups (birth conditions). Data regarding the categories of nutritional status were analyzed using the odds ratio (OR) and 95% confidence interval (CI). RESULTS: The prevalence of overweight/obesity in this sample was 24.5% (n=106). There was an association between inadequate weight gain and the prevalence of overweight/obesity (OR 2.7, 95%CI 1.5-4.9, p<0.05). Overweight/obese women had an increased risk for preeclampsia (OR 3.3, 95%CI 1.1--9.9, p=0.03). Regarding birth conditions, mean birth weight was 3291.3 g (±455.2), with rates of low birth weight of 4.7% (n=5) and rates of macrosomia of 2.8% (n=3). CONCLUSIONS: There was an alarming prevalence of inadequate nutritional status before and during pregnancy, which may be associated with increased risk of perinatal morbidity and mortality. This suggests the need for nutritional monitoring of these pregnant women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(11):348-353
DOI 10.1590/S0100-72032011001100005
PURPOSE: To describe the obstetric outcome of women with overweight/obesity treated at the prenatal care clinic of a public maternity hospital in Rio de Janeiro. METHODS: A descriptive cross-sectional study which investigated 433 women (³20 years-old, without any chronic diseases) and their newborns treated at public hospitals in Rio de Janeiro. Information was collected from medical records and through interviews. The characteristics of mothers and newborns evaluated were divided into maternal (social habits, anthropometric measurements and clinical, obstetric, and prenatal care) and newborn groups (birth conditions). Data regarding the categories of nutritional status were analyzed using the odds ratio (OR) and 95% confidence interval (CI). RESULTS: The prevalence of overweight/obesity in this sample was 24.5% (n=106). There was an association between inadequate weight gain and the prevalence of overweight/obesity (OR 2.7, 95%CI 1.5-4.9, p<0.05). Overweight/obese women had an increased risk for preeclampsia (OR 3.3, 95%CI 1.1--9.9, p=0.03). Regarding birth conditions, mean birth weight was 3291.3 g (±455.2), with rates of low birth weight of 4.7% (n=5) and rates of macrosomia of 2.8% (n=3). CONCLUSIONS: There was an alarming prevalence of inadequate nutritional status before and during pregnancy, which may be associated with increased risk of perinatal morbidity and mortality. This suggests the need for nutritional monitoring of these pregnant women.