Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):295-296
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):295-296
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):295-295
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):295-295
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(6):295-302
DOI 10.1590/S0100-72032011000600006
PURPOSE: To evaluate bone mineral density (BMD) and their risk factors associated with postmenopausal osteoporosis. METHODS: A cross-sectional clinical study was performed on 431 women (aged 40 - 75 years). Inclusion criteria: amenorrhea >12 months and age >45 years or, bilateral oophorectomy >40 years with BMD values (T-score of lumbar spine/femur neck) by DXA of the last 12 months. Risk factors evaluated: age, age and time of menopause, smoking, physical activity (30 min/5 times/week), rheumatoid arthritis (RA), use of corticotherapy and hormone therapy (HT), previous fracture, maternal hip fracture and body mass index (BMI=weight/height²). The χ2 test and the logistic regression method (Odds Ratio - OR) were used to determine osteoporosis risk. RESULTS: According to WHO criteria, 106 (24.6%) women showed osteoporosis (T-score <-2.5 DP), 188 (43.6%) osteopenia (-1.0/-2.4 DP), and 137 (31.8%) were normal (>-1.0 DP). Osteoporosis was detected in 12% of women aged 40 - 49 years, in 21.8% of women aged 50 - 59 years and in 45.7% of women aged >60 years (p<0.001). Osteoporosis occurred in 11.8% of women with a menopause period <5 years, in 29.4% with a menopause period from 6 to 10 years, and in 41% of women with a menopause period >10 years (p<0.001). Of the women with early menopause, 80% showed osteopenia/osteoporosis (p=0.03), and of those with BMI <20 kg/m², 50% were osteoporotic (p<0.001). The risk for osteoporosis detection increased with age (OR=1.1; CI95%=1.0-1.1), time of menopause (OR=1.1; CI95%=1.0-1.1), smoking (OR=1.9; CI95%=1.2-3.2), RA (OR=3.6; CI95%=1.3-9.6) and maternal fracture history (OR=2.1; CI95%=1.1-3.0) (p<0.05). In contrast, HT use (OR=0.3; 95%CI=0.2-0.6) and high BMI (OR=0.9; 95%CI=0.8-0.9) reduced the risk (p<0.05). CONCLUSION: In postmenopausal women, age, time of menopause, smoking and maternal history of fracture were clinical indicators of risk for osteoporosis, whereas HT use and high BMI proved to be protective factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(6):295-302
DOI 10.1590/S0100-72032011000600006
PURPOSE: To evaluate bone mineral density (BMD) and their risk factors associated with postmenopausal osteoporosis. METHODS: A cross-sectional clinical study was performed on 431 women (aged 40 - 75 years). Inclusion criteria: amenorrhea >12 months and age >45 years or, bilateral oophorectomy >40 years with BMD values (T-score of lumbar spine/femur neck) by DXA of the last 12 months. Risk factors evaluated: age, age and time of menopause, smoking, physical activity (30 min/5 times/week), rheumatoid arthritis (RA), use of corticotherapy and hormone therapy (HT), previous fracture, maternal hip fracture and body mass index (BMI=weight/height²). The χ2 test and the logistic regression method (Odds Ratio - OR) were used to determine osteoporosis risk. RESULTS: According to WHO criteria, 106 (24.6%) women showed osteoporosis (T-score <-2.5 DP), 188 (43.6%) osteopenia (-1.0/-2.4 DP), and 137 (31.8%) were normal (>-1.0 DP). Osteoporosis was detected in 12% of women aged 40 - 49 years, in 21.8% of women aged 50 - 59 years and in 45.7% of women aged >60 years (p<0.001). Osteoporosis occurred in 11.8% of women with a menopause period <5 years, in 29.4% with a menopause period from 6 to 10 years, and in 41% of women with a menopause period >10 years (p<0.001). Of the women with early menopause, 80% showed osteopenia/osteoporosis (p=0.03), and of those with BMI <20 kg/m², 50% were osteoporotic (p<0.001). The risk for osteoporosis detection increased with age (OR=1.1; CI95%=1.0-1.1), time of menopause (OR=1.1; CI95%=1.0-1.1), smoking (OR=1.9; CI95%=1.2-3.2), RA (OR=3.6; CI95%=1.3-9.6) and maternal fracture history (OR=2.1; CI95%=1.1-3.0) (p<0.05). In contrast, HT use (OR=0.3; 95%CI=0.2-0.6) and high BMI (OR=0.9; 95%CI=0.8-0.9) reduced the risk (p<0.05). CONCLUSION: In postmenopausal women, age, time of menopause, smoking and maternal history of fracture were clinical indicators of risk for osteoporosis, whereas HT use and high BMI proved to be protective factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):296-303
DOI 10.1590/S0100-72032012000700002
PURPOSE: To determine the pattern of alcohol use before and during pregnancy and associated risk factors in puerperal women hospitalized in a public university hospital in Southeastern Brazil. METHODS: Between June and September 2009, 493 puerperae were consecutively evaluated. Those with cognitive impairment were excluded from the study. The AUDIT and CAGE questionnaires were used to diagnose alcohol use/abuse before pregnancy, in addition to the T-ACE during pregnancy. Another questionnaire was applied to collect sociodemographic data, such as age, educational level, marital status, and household income. The χ² test was used in the statistical analysis and the Odds Ratio (OR) and 95% confidence interval (95%CI) were calculated. A p-value <0.05 was considered to be significant. RESULTS: Before pregnancy, the CAGE was positive in 50/405 (12.3%) women and the AUDIT identified alcohol use in 331 (67.1%), which was of low risk in 233 (47.3%), risky in 73 (14.8%), and harmful or indicating possible alcohol dependence in 25 (5%). During pregnancy, the CAGE was positive in 53/405 (13.1%) women and the T-ACE in 84 (17%); the AUDIT identified alcohol use in 114 women, which was of low risk in 73 (14.8%), risky in 27 (5.5%), and harmful or indicating possible alcohol dependence in 14 (2.8%). During pregnancy, alcohol use was more frequent (OR=2.8; 95%CI 1.2 - 6.2) among women with a lower educational level (8.8 versus 3.3%) and more frequent (OR=3.8; 95%CI 1.3 - 11.1) among those who did not cohabit with a partner (6 versus 1.7%). Among pregnant women who drank alcohol, 49/114 (43%) were advised to stop drinking. CONCLUSIONS: Alarming alcohol use was observed during pregnancy, especially among pregnant women with a lower educational level and those who did not cohabit with a partner. There was a low frequency of counseling aimed at abstinence and the AUDIT was the instrument that most frequently diagnosed alcohol consumption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):296-303
DOI 10.1590/S0100-72032012000700002
PURPOSE: To determine the pattern of alcohol use before and during pregnancy and associated risk factors in puerperal women hospitalized in a public university hospital in Southeastern Brazil. METHODS: Between June and September 2009, 493 puerperae were consecutively evaluated. Those with cognitive impairment were excluded from the study. The AUDIT and CAGE questionnaires were used to diagnose alcohol use/abuse before pregnancy, in addition to the T-ACE during pregnancy. Another questionnaire was applied to collect sociodemographic data, such as age, educational level, marital status, and household income. The χ² test was used in the statistical analysis and the Odds Ratio (OR) and 95% confidence interval (95%CI) were calculated. A p-value <0.05 was considered to be significant. RESULTS: Before pregnancy, the CAGE was positive in 50/405 (12.3%) women and the AUDIT identified alcohol use in 331 (67.1%), which was of low risk in 233 (47.3%), risky in 73 (14.8%), and harmful or indicating possible alcohol dependence in 25 (5%). During pregnancy, the CAGE was positive in 53/405 (13.1%) women and the T-ACE in 84 (17%); the AUDIT identified alcohol use in 114 women, which was of low risk in 73 (14.8%), risky in 27 (5.5%), and harmful or indicating possible alcohol dependence in 14 (2.8%). During pregnancy, alcohol use was more frequent (OR=2.8; 95%CI 1.2 - 6.2) among women with a lower educational level (8.8 versus 3.3%) and more frequent (OR=3.8; 95%CI 1.3 - 11.1) among those who did not cohabit with a partner (6 versus 1.7%). Among pregnant women who drank alcohol, 49/114 (43%) were advised to stop drinking. CONCLUSIONS: Alarming alcohol use was observed during pregnancy, especially among pregnant women with a lower educational level and those who did not cohabit with a partner. There was a low frequency of counseling aimed at abstinence and the AUDIT was the instrument that most frequently diagnosed alcohol consumption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(7):296-302
DOI 10.1590/SO100-720320140004958
To describe the perinatal outcomes after preterm premature rupture of membranes.
A retrospective cohort study was carried out at Instituto de Medicina Integral Prof. Fernando Figueira - IMIP from January 2008 to December 2012. A total of 124 preterm premature rupture of membranes singleton pregnancies, with gestational age <35, were included in the study. Pregnant women carrying fetuses with malformations, hypertensive syndromes, diabetes, or diagnosis of infections at admission were excluded. The pregnant women were hospitalized for conservative treatment with corticosteroids, antibiotics and tocolysis with nifedipine if necessary. The results are reported as frequency distributions and measures of central tendency and dispersion.
Seventeen patients (13.7%) had a gestational age of less than 24 weeks. Mean maternal age was 25.7 years, mean gestational age at the diagnosis of preterm premature rupture of membranes was 29 weeks, mean amniotic fluid index was 3.5 cm, and mean latency period was 10.5 days. Most patients went into spontaneous labor by the 30th week of pregnancy, and the rate of vaginal delivery was 88.2%. Chorioamnionitis was the most frequent maternal complication (34.7%). Neonatal sepsis was observed in 12% of patients, and the perinatal mortality rate was 21.5% for the group at or beyond the 24th week of gestation and 76.5% for the group with less than 24 weeks of gestational age.
A low maternal mortality rate was observed in preterm premature rupture of membranes; however, high rates of complications and perinatal death were observed, suggesting that other conduct protocols should be studied.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(7):296-302
DOI 10.1590/SO100-720320140004958
To describe the perinatal outcomes after preterm premature rupture of membranes.
A retrospective cohort study was carried out at Instituto de Medicina Integral Prof. Fernando Figueira - IMIP from January 2008 to December 2012. A total of 124 preterm premature rupture of membranes singleton pregnancies, with gestational age <35, were included in the study. Pregnant women carrying fetuses with malformations, hypertensive syndromes, diabetes, or diagnosis of infections at admission were excluded. The pregnant women were hospitalized for conservative treatment with corticosteroids, antibiotics and tocolysis with nifedipine if necessary. The results are reported as frequency distributions and measures of central tendency and dispersion.
Seventeen patients (13.7%) had a gestational age of less than 24 weeks. Mean maternal age was 25.7 years, mean gestational age at the diagnosis of preterm premature rupture of membranes was 29 weeks, mean amniotic fluid index was 3.5 cm, and mean latency period was 10.5 days. Most patients went into spontaneous labor by the 30th week of pregnancy, and the rate of vaginal delivery was 88.2%. Chorioamnionitis was the most frequent maternal complication (34.7%). Neonatal sepsis was observed in 12% of patients, and the perinatal mortality rate was 21.5% for the group at or beyond the 24th week of gestation and 76.5% for the group with less than 24 weeks of gestational age.
A low maternal mortality rate was observed in preterm premature rupture of membranes; however, high rates of complications and perinatal death were observed, suggesting that other conduct protocols should be studied.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):296-296
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):296-296
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(5):297-298
DOI 10.1590/S0100-72031999000500009
Endometrial ablation is a useful technique in patientes with abnormal uterine bleeding without response to clinical measures. Pregnancy is possible even after the destruction or resection of the endometrium. The case reported is a normal term pregnancy after endometrial ablation because ot menorrhagia without successful prior clinical treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(5):297-298
DOI 10.1590/S0100-72031999000500009
Endometrial ablation is a useful technique in patientes with abnormal uterine bleeding without response to clinical measures. Pregnancy is possible even after the destruction or resection of the endometrium. The case reported is a normal term pregnancy after endometrial ablation because ot menorrhagia without successful prior clinical treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(10):297-304
DOI 10.1590/S0100-72032011001000005
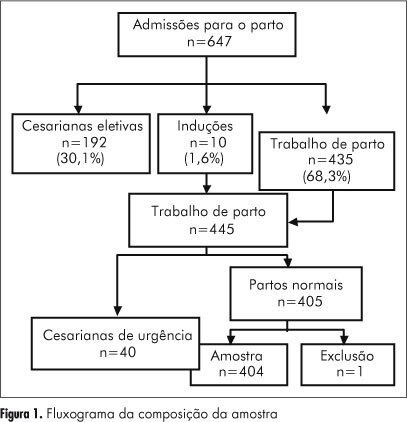
PURPOSE: To evaluate the quality of health care assistance during childbirth in the hospitals of Goiânia, in Brazil. METHODS: Thirteen hospitals were appraised from April to December 2007, and a random sample of 404 normal births was studied. Data were obtained from interviews with mothers after delivery and by consulting their medical records. The quality of assistance at birth was evaluated by using the Bologna score and by comparing the procedures used in those hospitals to standard recommended practices. RESULTS: The Bologna score presented an average value of 1.04 (95%CI=0.9-1.1). The elective caesarian rate was 30%, the emergency caesarian rate was 10%, and the rate of induced childbirth was 1.6% The percentage of childbirths attended by health care professionals was 100%, but pediatricians in the delivery room were present only in 30% of the time. During labor, half of the women had no evaluation of the uterine dynamics and 29% had no auscultation fetal monitoring. The partogram was used for only 28.5% of the women, whereas the use of oxytocin was 45.8%. CONCLUSIONS: The results indicate a poor quality of childbirth care with low values of the Bologna score, high elective and emergency caesarians rates, a high number of unnecessary and potentially harmful interventions, and an insufficient frequency of beneficial interventions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(10):297-304
DOI 10.1590/S0100-72032011001000005
PURPOSE: To evaluate the quality of health care assistance during childbirth in the hospitals of Goiânia, in Brazil. METHODS: Thirteen hospitals were appraised from April to December 2007, and a random sample of 404 normal births was studied. Data were obtained from interviews with mothers after delivery and by consulting their medical records. The quality of assistance at birth was evaluated by using the Bologna score and by comparing the procedures used in those hospitals to standard recommended practices. RESULTS: The Bologna score presented an average value of 1.04 (95%CI=0.9-1.1). The elective caesarian rate was 30%, the emergency caesarian rate was 10%, and the rate of induced childbirth was 1.6% The percentage of childbirths attended by health care professionals was 100%, but pediatricians in the delivery room were present only in 30% of the time. During labor, half of the women had no evaluation of the uterine dynamics and 29% had no auscultation fetal monitoring. The partogram was used for only 28.5% of the women, whereas the use of oxytocin was 45.8%. CONCLUSIONS: The results indicate a poor quality of childbirth care with low values of the Bologna score, high elective and emergency caesarians rates, a high number of unnecessary and potentially harmful interventions, and an insufficient frequency of beneficial interventions.