You searched for:"José Guilherme Cecatti"
We found (50) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo75
To identify the opinion of coordinators and members about the essential characteristics and to understand the research networks characteristics, to facilitate their implementation, sustainability and effectiveness so it can be replicated in low and middle-income countries.
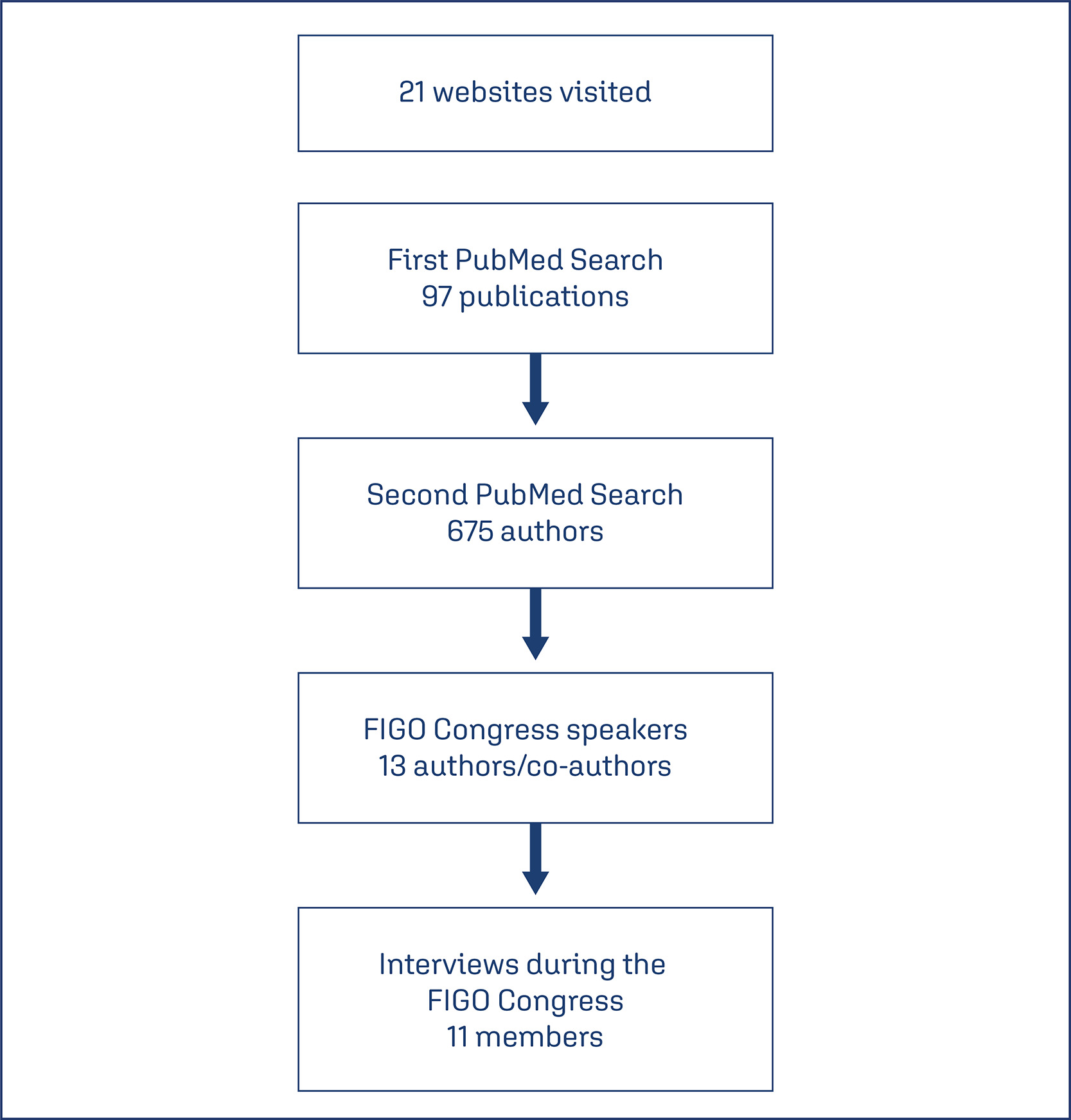
A qualitative study using a semi-structured interview technique was conducted. We selected potential members, managers and participants of networks from publications identified in PubMed. After checking the FIGO congress program, we identified authors who were assigned as speakers at the event. An invitation was sent and interviews were scheduled.
In total, eleven interviews were performed. Coordinators and members of networks have the same goal when they decide to participate in a network. In general, they cited that these individuals had to be committed, responsible and enthusiastic people. The network should be composed also of postgraduate students. A network should allow multi-leadership, co-responsibility, autonomy and empowerment of its members. Effective communication was mentioned as an important pillar for network maintenance. Another motivation is being an author or coauthor in publications. One way to maintain a network running is social or governmental commitment, after resources expire, studies continue.
Networks are different due to the social context where they are inserted, however, some characteristics are common to all of them, such as having engaged leaders. For an effective and sustainable network, commitment and motivation in a leader and members are more in need than financial resources. Ideally, to ensure the operation of the network, the institution where the leader is linked should support this network.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo75
To identify the opinion of coordinators and members about the essential characteristics and to understand the research networks characteristics, to facilitate their implementation, sustainability and effectiveness so it can be replicated in low and middle-income countries.
A qualitative study using a semi-structured interview technique was conducted. We selected potential members, managers and participants of networks from publications identified in PubMed. After checking the FIGO congress program, we identified authors who were assigned as speakers at the event. An invitation was sent and interviews were scheduled.
In total, eleven interviews were performed. Coordinators and members of networks have the same goal when they decide to participate in a network. In general, they cited that these individuals had to be committed, responsible and enthusiastic people. The network should be composed also of postgraduate students. A network should allow multi-leadership, co-responsibility, autonomy and empowerment of its members. Effective communication was mentioned as an important pillar for network maintenance. Another motivation is being an author or coauthor in publications. One way to maintain a network running is social or governmental commitment, after resources expire, studies continue.
Networks are different due to the social context where they are inserted, however, some characteristics are common to all of them, such as having engaged leaders. For an effective and sustainable network, commitment and motivation in a leader and members are more in need than financial resources. Ideally, to ensure the operation of the network, the institution where the leader is linked should support this network.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(2):101-106
DOI 10.1590/S0100-72032000000200007
Purpose: to evaluate the prevalence of anticardiolipin antibody in women with stillbirth. Patients and Methods: this was a cross-sectional study performed from May 1998 to September 1999 at the Maternity of the University of Campinas and at the Hospital and Maternity Leonor Mendes de Barros, in Brazil, which evaluated 109 pregnant women hospitalized with the diagnosis of intrauterine fetal death and gestational age of 20 or more weeks. These women underwent some laboratory examinations to identify the cause of fetal death, including anticardiolipin antibody evaluation performed through the determination of IgG and IgM serum levels. IgG and IgM results are expressed as GPL and MPL units, respectively, and, in both cases, results above 10 units are considered positive. The statistical procedures used were the mean and standard deviation estimates, Student's t test, Fisher test and chi². Results: the prevalence of anticardiolipin positivity was 18.3%. The women were predominantly young, with a mean age around 27 years. The main identified causes of fetal death were: hypertension (26.1%), hemorrhage during the third trimester (9.9%) and fetal malformation (8.1%). One third of the cases had no identified causes of fetal death. However, considering the 20 positive cases for anticardiolipin antibody, the proportion of unidentified causes decreased to 29%. Conclusions: it is important to investigate the presence of anticardiolipin antibodies among women with intrauterine fetal death with the purpose of clarifying the causes of stillbirth. If the diagnosis of antiphospholipid syndrome is confirmed, it is necessary to counsel and treat these women regarding future pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(2):101-106
DOI 10.1590/S0100-72032000000200007
Purpose: to evaluate the prevalence of anticardiolipin antibody in women with stillbirth. Patients and Methods: this was a cross-sectional study performed from May 1998 to September 1999 at the Maternity of the University of Campinas and at the Hospital and Maternity Leonor Mendes de Barros, in Brazil, which evaluated 109 pregnant women hospitalized with the diagnosis of intrauterine fetal death and gestational age of 20 or more weeks. These women underwent some laboratory examinations to identify the cause of fetal death, including anticardiolipin antibody evaluation performed through the determination of IgG and IgM serum levels. IgG and IgM results are expressed as GPL and MPL units, respectively, and, in both cases, results above 10 units are considered positive. The statistical procedures used were the mean and standard deviation estimates, Student's t test, Fisher test and chi². Results: the prevalence of anticardiolipin positivity was 18.3%. The women were predominantly young, with a mean age around 27 years. The main identified causes of fetal death were: hypertension (26.1%), hemorrhage during the third trimester (9.9%) and fetal malformation (8.1%). One third of the cases had no identified causes of fetal death. However, considering the 20 positive cases for anticardiolipin antibody, the proportion of unidentified causes decreased to 29%. Conclusions: it is important to investigate the presence of anticardiolipin antibodies among women with intrauterine fetal death with the purpose of clarifying the causes of stillbirth. If the diagnosis of antiphospholipid syndrome is confirmed, it is necessary to counsel and treat these women regarding future pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(3):103-105
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(3):103-105
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(3):105-111
DOI 10.1590/S0100-72032010000300002
PURPOSE: to evaluate the prevalence of spontaneous and induced abortion reported by a sample of Brazilian women interviewed in the National Demographic Health Survey of 1996. METHODS: this was a secondary analysis of the Brazilian DHS-96 database, with information from interviews with a representative sample of 12,612 women about their reproductive life, focusing on the prevalence of spontaneous and induced abortion in the last five years and the associated factors for the various regions of the country and for Brazil as a whole. The sampling method was implemented with a strategy selection in two stages, one for the households and the other for women. The prevalence of spontaneous and induced abortion was estimated for Brazil and regions, and the socio-demographic characteristics of the women were analyzed as a function of the abortion's experience. A multinomial regression model analysis was used for the identification of factors independently associated with both types of abortion; their OR and respective 95% CI are reported. RESULTS: the prevalence of reported spontaneous abortion was 14% and the prevalence of induced abortion was 2.4% for the country as a whole. The state with the highest prevalence of induced abortion was Rio de Janeiro with 6.5%, followed by the Northeast region with 3.1%. The places with the lowest prevalence were the state of São Paulo and the South region. Both spontaneous and induced abortion showed higher prevalences with increasing age of the women studied. Being from the urban area (OR=1.5; 95%CI=1.0-2.3), having had more than one live child (OR=2.2; 95%CI=1.5-3.2) and being non-white (OR=1.4; 95%CI=1.0-1.8) were the main risk factors for induced abortion. CONCLUSIONS: the non-modifiable risk factors for induced abortion identified in this study indicate the need for improvement of educational and contraceptive actions, with priority for these specific demographic groups.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(3):105-111
DOI 10.1590/S0100-72032010000300002
PURPOSE: to evaluate the prevalence of spontaneous and induced abortion reported by a sample of Brazilian women interviewed in the National Demographic Health Survey of 1996. METHODS: this was a secondary analysis of the Brazilian DHS-96 database, with information from interviews with a representative sample of 12,612 women about their reproductive life, focusing on the prevalence of spontaneous and induced abortion in the last five years and the associated factors for the various regions of the country and for Brazil as a whole. The sampling method was implemented with a strategy selection in two stages, one for the households and the other for women. The prevalence of spontaneous and induced abortion was estimated for Brazil and regions, and the socio-demographic characteristics of the women were analyzed as a function of the abortion's experience. A multinomial regression model analysis was used for the identification of factors independently associated with both types of abortion; their OR and respective 95% CI are reported. RESULTS: the prevalence of reported spontaneous abortion was 14% and the prevalence of induced abortion was 2.4% for the country as a whole. The state with the highest prevalence of induced abortion was Rio de Janeiro with 6.5%, followed by the Northeast region with 3.1%. The places with the lowest prevalence were the state of São Paulo and the South region. Both spontaneous and induced abortion showed higher prevalences with increasing age of the women studied. Being from the urban area (OR=1.5; 95%CI=1.0-2.3), having had more than one live child (OR=2.2; 95%CI=1.5-3.2) and being non-white (OR=1.4; 95%CI=1.0-1.8) were the main risk factors for induced abortion. CONCLUSIONS: the non-modifiable risk factors for induced abortion identified in this study indicate the need for improvement of educational and contraceptive actions, with priority for these specific demographic groups.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(3):106-114
The aim of this study is to evaluate the burden of indirect causes of maternal morbidity/mortality in Brazil.
Secondary analysis of a multicenter cross-sectional study conducted in 27 referral obstetric units within the Brazilian Network for Surveillance of Severe Maternal Morbidity.
A total of 82,388 women were surveilled: 9,555 women with severe maternal morbidity were included, and 942 (9.9%) of them had indirect causes of morbidity/ mortality. There was an increased risk of higher severity among the indirect causes group, which presented 7.56 times increased risk of maternal death (prevalence ratio [PR]: 7.56; 95% confidence interval [95%CI]: 4.99-11.45). The main indirect causes of maternal death were H1N1 influenza, sepsis, cancer and cardiovascular disease. Non-public antenatal care (PR: 2.52; 95%CI: 1.70-3.74), diabetes (PR: 1.90; 95%CI: 1.24-2.90), neoplasia (PR: 1.98; 95%CI: 1.25-3.14), kidney diseases (PR: 1.99; 95%CI: 1.14-3.49), sickle cell anemia (PR: 2.50; 95%CI: 1.16-5.41) and drug addiction (PR: 1.98; 95%CI: 1.03-3.80) were independentlyassociatedwithworseresultsintheindirectcausesgroup.Someprocedures for the management of severity were more common for the indirect causes group.
Indirect causes were present in less than 10% of the overall cases, but they represented over 40% of maternal deaths in the current study. Indirect causes of maternal morbidity/mortality were also responsible for an increased risk of higher severity, and they were associated with worse maternal and perinatal outcomes. In middle-income countries there is a mix of indirect causes of maternal morbidity/ mortality that points to some advances in the scale of obstetric transition, but also reveals the fragility of health systems.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(3):106-114
The aim of this study is to evaluate the burden of indirect causes of maternal morbidity/mortality in Brazil.
Secondary analysis of a multicenter cross-sectional study conducted in 27 referral obstetric units within the Brazilian Network for Surveillance of Severe Maternal Morbidity.
A total of 82,388 women were surveilled: 9,555 women with severe maternal morbidity were included, and 942 (9.9%) of them had indirect causes of morbidity/ mortality. There was an increased risk of higher severity among the indirect causes group, which presented 7.56 times increased risk of maternal death (prevalence ratio [PR]: 7.56; 95% confidence interval [95%CI]: 4.99-11.45). The main indirect causes of maternal death were H1N1 influenza, sepsis, cancer and cardiovascular disease. Non-public antenatal care (PR: 2.52; 95%CI: 1.70-3.74), diabetes (PR: 1.90; 95%CI: 1.24-2.90), neoplasia (PR: 1.98; 95%CI: 1.25-3.14), kidney diseases (PR: 1.99; 95%CI: 1.14-3.49), sickle cell anemia (PR: 2.50; 95%CI: 1.16-5.41) and drug addiction (PR: 1.98; 95%CI: 1.03-3.80) were independentlyassociatedwithworseresultsintheindirectcausesgroup.Someprocedures for the management of severity were more common for the indirect causes group.
Indirect causes were present in less than 10% of the overall cases, but they represented over 40% of maternal deaths in the current study. Indirect causes of maternal morbidity/mortality were also responsible for an increased risk of higher severity, and they were associated with worse maternal and perinatal outcomes. In middle-income countries there is a mix of indirect causes of maternal morbidity/ mortality that points to some advances in the scale of obstetric transition, but also reveals the fragility of health systems.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):11-20
Systemic lupus erythematosus (SLE) may cause irreversible organ damage. Pregnancy with SLE may have severe life-threatening risks. The present study aimed to determine the prevalence of severe maternal morbidity (SMM) in patients with SLE and analyze the parameters that contributed to cases of greater severity.
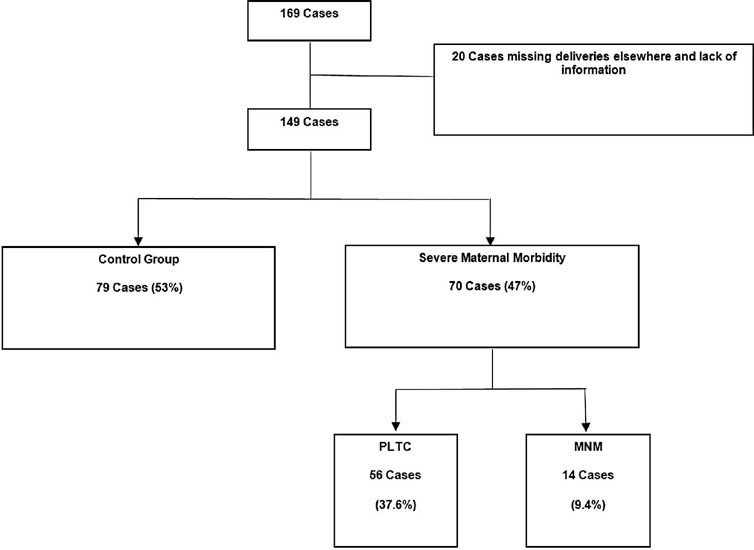
This is a cross-sectional retrospective study from analysis of data retrieved from medical records of pregnant women with SLE treated at a University Hospital in Brazil. The pregnant women were divided in a control group without complications, a group with potentially life-threatening conditions (PLTC), and a group with maternal near miss (MNM).
The maternal near miss rate was 112.9 per 1,000 live births. The majority of PLTC (83.9%) and MNM (92.9%) cases had preterm deliveries with statistically significant increased risk compared with the control group (p = 0.0042; odds ratio [OR]: 12.05; 95% confidence interval [CI]: 1.5–96.6 for the MNM group and p = 0.0001; OR: 4.84; 95%CI: 2.2–10.8 for the PLTC group). Severe maternal morbidity increases the risk of longer hospitalization (p < 0.0001; OR: 18.8; 95%CI: 7.0–50.6 and p < 0.0001; OR: 158.17; 95%CI: 17.6–1424,2 for the PLTC and MNM groups, respectively), newborns with low birthweight (p = 0.0006; OR: 3.67; 95%CI: 1.7–7.9 and p = 0.0009; OR: 17.68; 95%CI: 2–153.6) for the PLTC and MNM groups, respectively] as well as renal diseases (PLTC [8.9%; 33/56; p = 0.0069] and MNM [78.6%; 11/14; p = 0.0026]). Maternal near miss cases presented increased risk for neonatal death (p = 0.0128; OR: 38.4; 95%CI: 3.3–440.3]), and stillbirth and miscarriage (p = 0.0011; OR: 7.68; 95%CI: 2.2–26.3]).
Systemic lupus erythematosus was significantly associated with severe maternal morbidity, longer hospitalizations, and increased risk of poor obstetric and neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):11-20
Systemic lupus erythematosus (SLE) may cause irreversible organ damage. Pregnancy with SLE may have severe life-threatening risks. The present study aimed to determine the prevalence of severe maternal morbidity (SMM) in patients with SLE and analyze the parameters that contributed to cases of greater severity.
This is a cross-sectional retrospective study from analysis of data retrieved from medical records of pregnant women with SLE treated at a University Hospital in Brazil. The pregnant women were divided in a control group without complications, a group with potentially life-threatening conditions (PLTC), and a group with maternal near miss (MNM).
The maternal near miss rate was 112.9 per 1,000 live births. The majority of PLTC (83.9%) and MNM (92.9%) cases had preterm deliveries with statistically significant increased risk compared with the control group (p = 0.0042; odds ratio [OR]: 12.05; 95% confidence interval [CI]: 1.5–96.6 for the MNM group and p = 0.0001; OR: 4.84; 95%CI: 2.2–10.8 for the PLTC group). Severe maternal morbidity increases the risk of longer hospitalization (p < 0.0001; OR: 18.8; 95%CI: 7.0–50.6 and p < 0.0001; OR: 158.17; 95%CI: 17.6–1424,2 for the PLTC and MNM groups, respectively), newborns with low birthweight (p = 0.0006; OR: 3.67; 95%CI: 1.7–7.9 and p = 0.0009; OR: 17.68; 95%CI: 2–153.6) for the PLTC and MNM groups, respectively] as well as renal diseases (PLTC [8.9%; 33/56; p = 0.0069] and MNM [78.6%; 11/14; p = 0.0026]). Maternal near miss cases presented increased risk for neonatal death (p = 0.0128; OR: 38.4; 95%CI: 3.3–440.3]), and stillbirth and miscarriage (p = 0.0011; OR: 7.68; 95%CI: 2.2–26.3]).
Systemic lupus erythematosus was significantly associated with severe maternal morbidity, longer hospitalizations, and increased risk of poor obstetric and neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(3):124-132
To assess the use of the intensive care unit (ICU) and its effect on maternal mortality (MM) among women with severe maternal morbidity (SMM).
A secondary analysis of a cross-sectional study on surveillance of SMM in 27 Brazilian obstetric referral centers. The analysis focused on the association between ICU use and maternal death according to individual characteristics and disease severity. Two multivariate regressions considering use of the ICU, age, ethnicity, adequacy of care and the human development index were performed to identify the factors associated to maternal death and maternal near-miss.
Out of 82,388 deliveries during the period, there were 9,555 (11.6%) women with SMM, and the MM ratio was of 170.4/100 thousand live births. In total, 8,135 (85.1%) patients were managed in facilities in which ICUs were available; however, only 2,059 (25.3%) had been admitted to the ICU. On the multivariate analysis, when the severity of the maternal disease was measured by the maternal severity score (MMS), the strength of the association between the use of the ICU and maternal death was greatly reduced, along with inadequate care and non-availability of the ICU at the facility. On the assessment of only the more critical cases (SMO, severe maternal outcome), the same pattern of association between ICU and MM was observed. In the models used, only inadequate care and MSS were significantly associated with MM.
The current study indicates that the main variables associated with maternal death are the severity and adequacy of the case management, which is more frequent in ICU admissions. The use of the ICU without the stratification of the patients by severity may not produce the expected benefits for part of the women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(3):124-132
To assess the use of the intensive care unit (ICU) and its effect on maternal mortality (MM) among women with severe maternal morbidity (SMM).
A secondary analysis of a cross-sectional study on surveillance of SMM in 27 Brazilian obstetric referral centers. The analysis focused on the association between ICU use and maternal death according to individual characteristics and disease severity. Two multivariate regressions considering use of the ICU, age, ethnicity, adequacy of care and the human development index were performed to identify the factors associated to maternal death and maternal near-miss.
Out of 82,388 deliveries during the period, there were 9,555 (11.6%) women with SMM, and the MM ratio was of 170.4/100 thousand live births. In total, 8,135 (85.1%) patients were managed in facilities in which ICUs were available; however, only 2,059 (25.3%) had been admitted to the ICU. On the multivariate analysis, when the severity of the maternal disease was measured by the maternal severity score (MMS), the strength of the association between the use of the ICU and maternal death was greatly reduced, along with inadequate care and non-availability of the ICU at the facility. On the assessment of only the more critical cases (SMO, severe maternal outcome), the same pattern of association between ICU and MM was observed. In the models used, only inadequate care and MSS were significantly associated with MM.
The current study indicates that the main variables associated with maternal death are the severity and adequacy of the case management, which is more frequent in ICU admissions. The use of the ICU without the stratification of the patients by severity may not produce the expected benefits for part of the women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(3):145-149
DOI 10.1590/S0100-72031998000300004
Although 80 to 90% of all dead fetuses may be spontaneously eliminated after two to three weeks from death, labor induction has been the mostly used management. The purpose of the current study was to evaluate the results of labor induction for pregnancies with fetal death and gestation age above 20 weeks. It was a descriptive clinical study which was performed at the Hospital e Maternidade Leonor Mendes de Barros in São Paulo, Brazil. One hundred and twenty-two pregnancies with fetal death were evaluated regarding their social and demographic characteristics, causes of fetal death, previous pregnancies history and delivery (induction, route, complications). The statistical procedures used were estimation of mean and standard deviation and chi². The main causes of fetal death were hypertension and infections. The mostly used drug for labor induction was misoprostol (37.7%) followed by oxytocin (19.7%), while 27% of cases had spontaneous onset of labor. The mean time of induction was 3 hours. The majority of women had vaginal delivery and cesarean section was performed in 9.1% of them. It is concluded that labor induction for fetal death is safe and efficient, irrespective of the method used. Misoprostol when used in the vagina is specially useful for cases with an unripe cervix because of the modifying effect of the drug on the cervix.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(3):145-149
DOI 10.1590/S0100-72031998000300004
Although 80 to 90% of all dead fetuses may be spontaneously eliminated after two to three weeks from death, labor induction has been the mostly used management. The purpose of the current study was to evaluate the results of labor induction for pregnancies with fetal death and gestation age above 20 weeks. It was a descriptive clinical study which was performed at the Hospital e Maternidade Leonor Mendes de Barros in São Paulo, Brazil. One hundred and twenty-two pregnancies with fetal death were evaluated regarding their social and demographic characteristics, causes of fetal death, previous pregnancies history and delivery (induction, route, complications). The statistical procedures used were estimation of mean and standard deviation and chi². The main causes of fetal death were hypertension and infections. The mostly used drug for labor induction was misoprostol (37.7%) followed by oxytocin (19.7%), while 27% of cases had spontaneous onset of labor. The mean time of induction was 3 hours. The majority of women had vaginal delivery and cesarean section was performed in 9.1% of them. It is concluded that labor induction for fetal death is safe and efficient, irrespective of the method used. Misoprostol when used in the vagina is specially useful for cases with an unripe cervix because of the modifying effect of the drug on the cervix.