You searched for:"Fernanda Garanhani Surita"
We found (38) results for your search.Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo45
To explore women's experiences with postpartum intrauterine device (PPIUD) insertion and the decision-making process in the postpartum period.
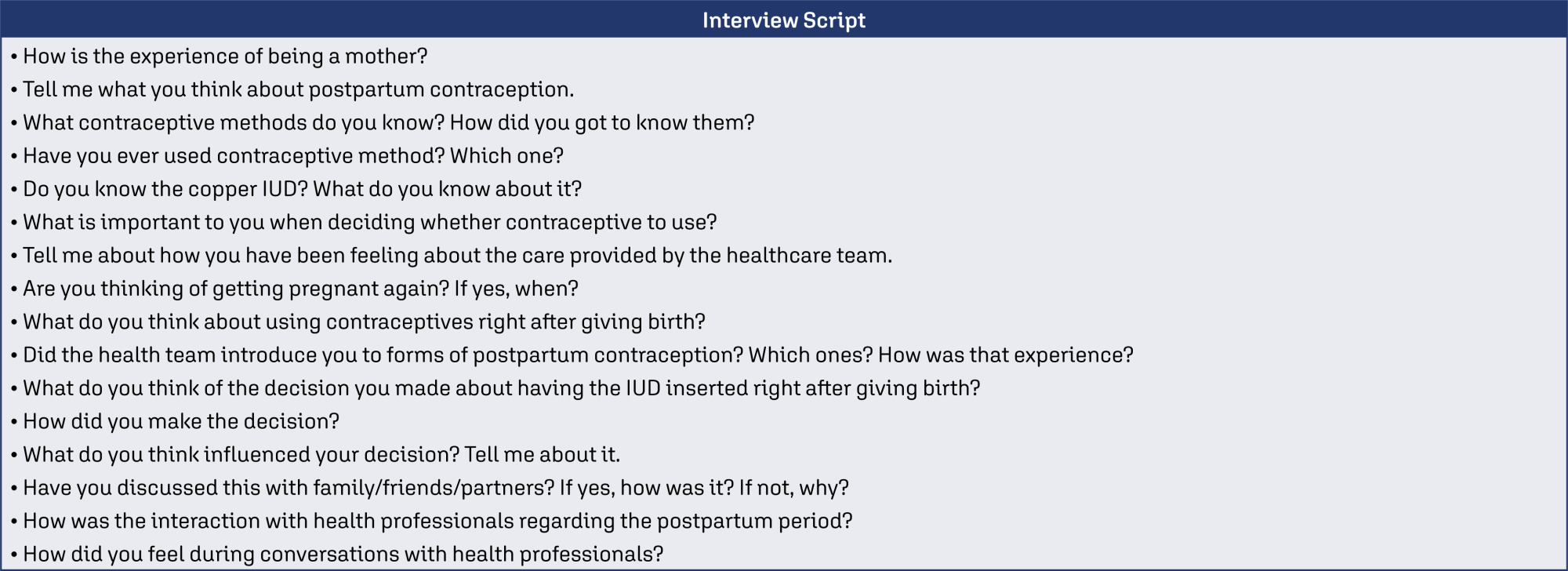
A qualitative design was employed with face-to-face interviews using a semi-structured script of open questions. The sample was intentionally selected using the concept of theoretical information saturation.
Interviews were conducted (1) in the immediate postpartum period, and (2) in the postpartum appointment. 25 women (N = 25) over 18 years old who had a birth followed by PPIUD insertion were interviewed between October 2021 and June 2022. Three categories were constructed: (1) Choice process, (2) Relationship with the health team at the time of birth and the postpartum period, and (3) To know or not to know about contraception, that is the question.
Professionals’ communication management, popular knowledge, advantages of the PPIUD and the moment PPIUD is offered play a fundamental role in the construction of knowledge about the IUD. Choice process did not end in the insertion.
Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo45
To explore women's experiences with postpartum intrauterine device (PPIUD) insertion and the decision-making process in the postpartum period.
A qualitative design was employed with face-to-face interviews using a semi-structured script of open questions. The sample was intentionally selected using the concept of theoretical information saturation.
Interviews were conducted (1) in the immediate postpartum period, and (2) in the postpartum appointment. 25 women (N = 25) over 18 years old who had a birth followed by PPIUD insertion were interviewed between October 2021 and June 2022. Three categories were constructed: (1) Choice process, (2) Relationship with the health team at the time of birth and the postpartum period, and (3) To know or not to know about contraception, that is the question.
Professionals’ communication management, popular knowledge, advantages of the PPIUD and the moment PPIUD is offered play a fundamental role in the construction of knowledge about the IUD. Choice process did not end in the insertion.
Summary
Rev Bras Ginecol Obstet. 2015;37(1):05-09
DOI 10.1590/SO100-720320140005130
To describe maternal and neonatal outcomes in pregnant women undergoing hemodialysis in a referral center in Brazilian Southeast side.
Retrospective and descriptive study, with chart review of all pregnancies undergoing hemodialysis that were followed-up at an outpatient clinic of high- risk prenatal care in Southeast Brazil.
Among the 16 women identified, 2 were excluded due to follow-up loss. In 14 women described, hypertension was the most frequent cause of chronic renal failure (half of cases). The majority (71.4%) had performed hemodialysis treatment for more than one year and all of them underwent 5 to 6 hemodialysis sessions per week. Eleven participants had chronic hypertension, 1 of which was also diabetic, and 6 of them were smokers. Regarding pregnancy complications, 1 of the hypertensive women developed malignant hypertension (with fetal growth restriction and preterm delivery at 29 weeks), 2 had acute pulmonary edema and 2 had abruption placenta. The mode of delivery was cesarean section in 9 women (64.3%). All neonates had Apgar score at five minutes above 7.
To improve perinatal and maternal outcomes of women undergoing hemodialysis, it is important to ensure multidisciplinary approach in referral center, strict control of serum urea, hemoglobin and maternal blood pressure, as well as close monitoring of fetal well-being and maternal morbidities. Another important strategy is suitable guidance for contraception in these women.
Summary
Rev Bras Ginecol Obstet. 2015;37(1):05-09
DOI 10.1590/SO100-720320140005130
To describe maternal and neonatal outcomes in pregnant women undergoing hemodialysis in a referral center in Brazilian Southeast side.
Retrospective and descriptive study, with chart review of all pregnancies undergoing hemodialysis that were followed-up at an outpatient clinic of high- risk prenatal care in Southeast Brazil.
Among the 16 women identified, 2 were excluded due to follow-up loss. In 14 women described, hypertension was the most frequent cause of chronic renal failure (half of cases). The majority (71.4%) had performed hemodialysis treatment for more than one year and all of them underwent 5 to 6 hemodialysis sessions per week. Eleven participants had chronic hypertension, 1 of which was also diabetic, and 6 of them were smokers. Regarding pregnancy complications, 1 of the hypertensive women developed malignant hypertension (with fetal growth restriction and preterm delivery at 29 weeks), 2 had acute pulmonary edema and 2 had abruption placenta. The mode of delivery was cesarean section in 9 women (64.3%). All neonates had Apgar score at five minutes above 7.
To improve perinatal and maternal outcomes of women undergoing hemodialysis, it is important to ensure multidisciplinary approach in referral center, strict control of serum urea, hemoglobin and maternal blood pressure, as well as close monitoring of fetal well-being and maternal morbidities. Another important strategy is suitable guidance for contraception in these women.
Summary
Rev Bras Ginecol Obstet. 2018;40(3):106-114
The aim of this study is to evaluate the burden of indirect causes of maternal morbidity/mortality in Brazil.
Secondary analysis of a multicenter cross-sectional study conducted in 27 referral obstetric units within the Brazilian Network for Surveillance of Severe Maternal Morbidity.
A total of 82,388 women were surveilled: 9,555 women with severe maternal morbidity were included, and 942 (9.9%) of them had indirect causes of morbidity/ mortality. There was an increased risk of higher severity among the indirect causes group, which presented 7.56 times increased risk of maternal death (prevalence ratio [PR]: 7.56; 95% confidence interval [95%CI]: 4.99-11.45). The main indirect causes of maternal death were H1N1 influenza, sepsis, cancer and cardiovascular disease. Non-public antenatal care (PR: 2.52; 95%CI: 1.70-3.74), diabetes (PR: 1.90; 95%CI: 1.24-2.90), neoplasia (PR: 1.98; 95%CI: 1.25-3.14), kidney diseases (PR: 1.99; 95%CI: 1.14-3.49), sickle cell anemia (PR: 2.50; 95%CI: 1.16-5.41) and drug addiction (PR: 1.98; 95%CI: 1.03-3.80) were independentlyassociatedwithworseresultsintheindirectcausesgroup.Someprocedures for the management of severity were more common for the indirect causes group.
Indirect causes were present in less than 10% of the overall cases, but they represented over 40% of maternal deaths in the current study. Indirect causes of maternal morbidity/mortality were also responsible for an increased risk of higher severity, and they were associated with worse maternal and perinatal outcomes. In middle-income countries there is a mix of indirect causes of maternal morbidity/ mortality that points to some advances in the scale of obstetric transition, but also reveals the fragility of health systems.
Summary
Rev Bras Ginecol Obstet. 2018;40(3):106-114
The aim of this study is to evaluate the burden of indirect causes of maternal morbidity/mortality in Brazil.
Secondary analysis of a multicenter cross-sectional study conducted in 27 referral obstetric units within the Brazilian Network for Surveillance of Severe Maternal Morbidity.
A total of 82,388 women were surveilled: 9,555 women with severe maternal morbidity were included, and 942 (9.9%) of them had indirect causes of morbidity/ mortality. There was an increased risk of higher severity among the indirect causes group, which presented 7.56 times increased risk of maternal death (prevalence ratio [PR]: 7.56; 95% confidence interval [95%CI]: 4.99-11.45). The main indirect causes of maternal death were H1N1 influenza, sepsis, cancer and cardiovascular disease. Non-public antenatal care (PR: 2.52; 95%CI: 1.70-3.74), diabetes (PR: 1.90; 95%CI: 1.24-2.90), neoplasia (PR: 1.98; 95%CI: 1.25-3.14), kidney diseases (PR: 1.99; 95%CI: 1.14-3.49), sickle cell anemia (PR: 2.50; 95%CI: 1.16-5.41) and drug addiction (PR: 1.98; 95%CI: 1.03-3.80) were independentlyassociatedwithworseresultsintheindirectcausesgroup.Someprocedures for the management of severity were more common for the indirect causes group.
Indirect causes were present in less than 10% of the overall cases, but they represented over 40% of maternal deaths in the current study. Indirect causes of maternal morbidity/mortality were also responsible for an increased risk of higher severity, and they were associated with worse maternal and perinatal outcomes. In middle-income countries there is a mix of indirect causes of maternal morbidity/ mortality that points to some advances in the scale of obstetric transition, but also reveals the fragility of health systems.
Summary
Rev Bras Ginecol Obstet. 2022;44(12):1094-1101
To assess maternal and neonatal outcomes in women with chronic kidney disease (CKD) at a referral center for high-risk pregnancy.
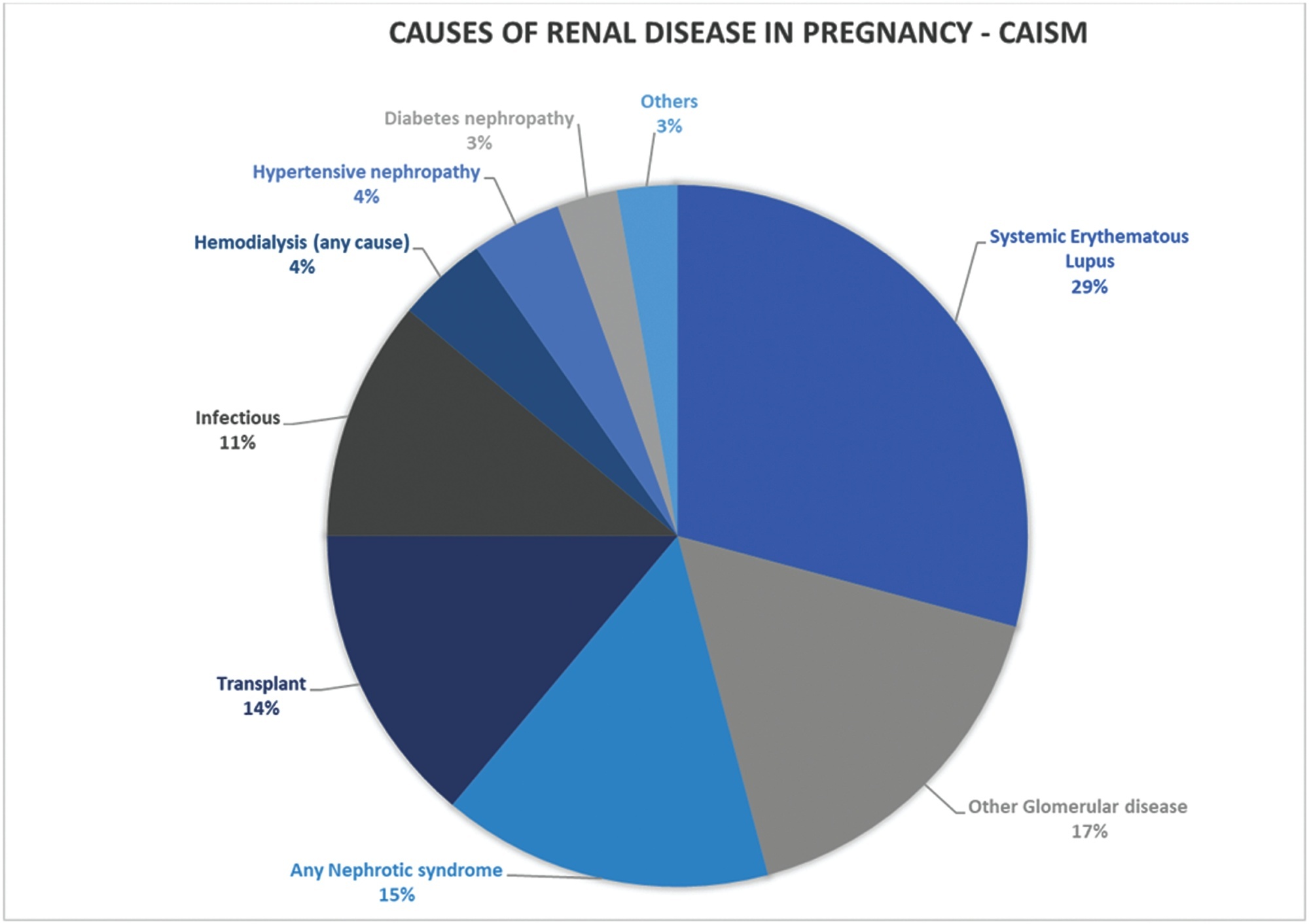
A retrospective cohort of pregnant women with CKD was followed at the Women's Hospital of Universidade Estadual de Campinas, Brazil, between 2012 and 2020. Variables related to disease etiology, treatment duration, sociodemographic variables, lifestyle, other associated diseases, obstetric history, and perinatal outcomes were assessed. The causes of CKD were grouped into 10 subgroups. Subsequently, we divided the sample according to gestational age at childbirth, as preterm and term births, comparing maternal and neonatal outcomes, and baseline characteristics as well as outcomes among such groups.
A total of 84 pregnancies were included, in 67 women with CKD. Among them, six pregnancies evolved to fetal death, five to miscarriage, and one was a twin pregnancy. We further analyzed 72 single pregnancies with live births; the mean gestational age at birth was 35 weeks and 3 days, with a mean birth weight of 2,444 g. Around half of the sample (51.39%) presented previous hypertension, and 27.7% developed preeclampsia. Among the preterm births, we observed a higher frequency of hypertensive syndromes, longer maternal intensive care unit (ICU) stay in the postpartum period, higher incidence of admission to the neonatal ICU, higher neonatal death, lower 5-minute Apgar score, and lower birth weight.
This study demonstrates increased adverse outcomes among pregnancies complicated by CKD and expands the knowledge on obstetric care among such women in an attempt to reduce maternal risks and identify factors related to prematurity in this population.
Summary
Rev Bras Ginecol Obstet. 2022;44(12):1094-1101
To assess maternal and neonatal outcomes in women with chronic kidney disease (CKD) at a referral center for high-risk pregnancy.
A retrospective cohort of pregnant women with CKD was followed at the Women's Hospital of Universidade Estadual de Campinas, Brazil, between 2012 and 2020. Variables related to disease etiology, treatment duration, sociodemographic variables, lifestyle, other associated diseases, obstetric history, and perinatal outcomes were assessed. The causes of CKD were grouped into 10 subgroups. Subsequently, we divided the sample according to gestational age at childbirth, as preterm and term births, comparing maternal and neonatal outcomes, and baseline characteristics as well as outcomes among such groups.
A total of 84 pregnancies were included, in 67 women with CKD. Among them, six pregnancies evolved to fetal death, five to miscarriage, and one was a twin pregnancy. We further analyzed 72 single pregnancies with live births; the mean gestational age at birth was 35 weeks and 3 days, with a mean birth weight of 2,444 g. Around half of the sample (51.39%) presented previous hypertension, and 27.7% developed preeclampsia. Among the preterm births, we observed a higher frequency of hypertensive syndromes, longer maternal intensive care unit (ICU) stay in the postpartum period, higher incidence of admission to the neonatal ICU, higher neonatal death, lower 5-minute Apgar score, and lower birth weight.
This study demonstrates increased adverse outcomes among pregnancies complicated by CKD and expands the knowledge on obstetric care among such women in an attempt to reduce maternal risks and identify factors related to prematurity in this population.
Summary
Rev Bras Ginecol Obstet. 2018;40(1):11-19
To evaluate the relation between changes the body mass index (BMI) percentile, reflected in the Atalah curve, and perinatal outcomes.
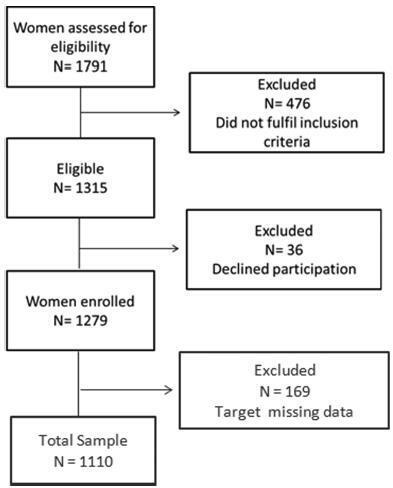
A cross-sectional study with 1,279 women was performed. Data regarding gestational weight, sociodemographic characteristics and perinatal outcomes were collected through medical charts, prenatal card and interviews in the postpartum period. Women could be classified according to the Atalah curve in the following categories: low weight, adequateweight, overweight, and obese. The BMIwas calculated at the first and at the last prenatal care visits, and these values were compared.
An increase in the BMI category according to the Atalah classification occurred in 19.9% of pregnant women, and an increase of 3.4, 5.8 and 6.4 points of BMI were found for women respectively classified in the adequate weight, overweight and obese categories at the first prenatal visit. Women with high school education presented a lower chance of increasing their BMI (odds ratio [OR] 0:47 [0.24- 0.95]). Women who evolved with an increase in the the Atalah classification were associated with cesarean section (OR 1.97-2.28), fetalmacrosomia (OR 4.13-12.54) and large for gestational age newborn (OR 2.88-9.83).
Pregnant women who gained enough weight to move up in their BMI classification according to the Atalah curve had a higher chance of cesarean section and macrosomia. Women classified as obese, according to the Atalah curve, at the first prenatal visit had a high chance of cesarean section and delivering a large for gestational age newborn.
Summary
Rev Bras Ginecol Obstet. 2018;40(1):11-19
To evaluate the relation between changes the body mass index (BMI) percentile, reflected in the Atalah curve, and perinatal outcomes.
A cross-sectional study with 1,279 women was performed. Data regarding gestational weight, sociodemographic characteristics and perinatal outcomes were collected through medical charts, prenatal card and interviews in the postpartum period. Women could be classified according to the Atalah curve in the following categories: low weight, adequateweight, overweight, and obese. The BMIwas calculated at the first and at the last prenatal care visits, and these values were compared.
An increase in the BMI category according to the Atalah classification occurred in 19.9% of pregnant women, and an increase of 3.4, 5.8 and 6.4 points of BMI were found for women respectively classified in the adequate weight, overweight and obese categories at the first prenatal visit. Women with high school education presented a lower chance of increasing their BMI (odds ratio [OR] 0:47 [0.24- 0.95]). Women who evolved with an increase in the the Atalah classification were associated with cesarean section (OR 1.97-2.28), fetalmacrosomia (OR 4.13-12.54) and large for gestational age newborn (OR 2.88-9.83).
Pregnant women who gained enough weight to move up in their BMI classification according to the Atalah curve had a higher chance of cesarean section and macrosomia. Women classified as obese, according to the Atalah curve, at the first prenatal visit had a high chance of cesarean section and delivering a large for gestational age newborn.
Summary
Rev Bras Ginecol Obstet. 2020;42(3):121-123
Summary
Rev Bras Ginecol Obstet. 2020;42(3):121-123
Summary
Rev Bras Ginecol Obstet. 2021;43(3):172-177
To evaluate the acceptability of postplacental placement of intrauterine devices (PPIUD), reasons for refusal and suggested policies to increase its use.
Cross-sectional study conducted at the Women Hospital of the Universidade de Campinas, Campinas, SP, Brazil. Postplacental placement of intrauterine devices was offered to women admitted in labor who did not present infections, uterinemalformation, twin pregnancy, preterm birth, and were at least 18 years old. In case of refusal, the parturient was asked to give their reasons and the answers were classified as misinformation about contraception or other reasons. The following were considered misinformation: fear of pain, bleeding, contraception failure and future infertility. Bivariate analysis was performed.
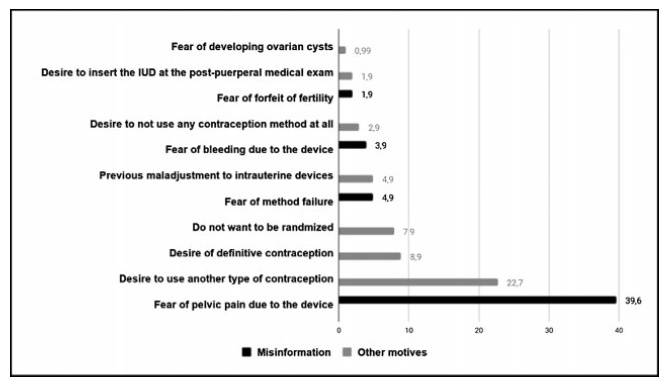
Amongst 241 invited women, the refusal rate was of 41.9%. Misinformation corresponded to 50.5% of all refusals, and the reasons were: fear of pain (39.9%); fear of contraception failure (4.9%); fear of bleeding (3.9%); fear of future infertility (1.9%); other reasons for refusal were 49.5%. Parturients aged between 18 and 27 years old refused the PPIUD more frequently due to misinformation (67.4%), and older parturients (between 28 and 43 years old) refused frequently due to other reasons (63.6%) (p=0.002). Themean age of those who declined the PPIUD due to misinformation was 27.3 ± 6.4 years old, while those who declined for other reasons had a mean age of 29.9 ± 5.9 years old (p=0.017).
The refusal of the PPIUD was high, especially amongst young women and due to misinformation. It is necessary to develop educative measures during antenatal care to counsel women about contraception, reproductive health and consequences of unintended pregnancy.
Summary
Rev Bras Ginecol Obstet. 2021;43(3):172-177
To evaluate the acceptability of postplacental placement of intrauterine devices (PPIUD), reasons for refusal and suggested policies to increase its use.
Cross-sectional study conducted at the Women Hospital of the Universidade de Campinas, Campinas, SP, Brazil. Postplacental placement of intrauterine devices was offered to women admitted in labor who did not present infections, uterinemalformation, twin pregnancy, preterm birth, and were at least 18 years old. In case of refusal, the parturient was asked to give their reasons and the answers were classified as misinformation about contraception or other reasons. The following were considered misinformation: fear of pain, bleeding, contraception failure and future infertility. Bivariate analysis was performed.
Amongst 241 invited women, the refusal rate was of 41.9%. Misinformation corresponded to 50.5% of all refusals, and the reasons were: fear of pain (39.9%); fear of contraception failure (4.9%); fear of bleeding (3.9%); fear of future infertility (1.9%); other reasons for refusal were 49.5%. Parturients aged between 18 and 27 years old refused the PPIUD more frequently due to misinformation (67.4%), and older parturients (between 28 and 43 years old) refused frequently due to other reasons (63.6%) (p=0.002). Themean age of those who declined the PPIUD due to misinformation was 27.3 ± 6.4 years old, while those who declined for other reasons had a mean age of 29.9 ± 5.9 years old (p=0.017).
The refusal of the PPIUD was high, especially amongst young women and due to misinformation. It is necessary to develop educative measures during antenatal care to counsel women about contraception, reproductive health and consequences of unintended pregnancy.
Summary
Rev Bras Ginecol Obstet. 2020;42(1):19-25
To explore the experiences of women with obesity regarding self-care and the care provided by their families and health team after childbirth.
A clinical qualitative study performed at the Postnatal Outpatient Clinic of Hospital da Mulher, Universidade Estadual de Campinas, Brazil. The sample was selected using the saturation criteria, with 16 women with obesity up to 6 months after childbirth.
The analysis comprised three categories: 1) postnatal self-care; 2) family support for woman after childbirth; and 3) postnatal health care service for women with obesity.
Women with obesity need support from the health team and from their families after childbirth, when they are overwhelmed by the exhausting care for the newborn. The present study reveals how important it is for health care professionals to broaden their perception and care provided after childbirth for women with obesity so they may experience an improvement in their quality of health and of life.
Summary
Rev Bras Ginecol Obstet. 2020;42(1):19-25
To explore the experiences of women with obesity regarding self-care and the care provided by their families and health team after childbirth.
A clinical qualitative study performed at the Postnatal Outpatient Clinic of Hospital da Mulher, Universidade Estadual de Campinas, Brazil. The sample was selected using the saturation criteria, with 16 women with obesity up to 6 months after childbirth.
The analysis comprised three categories: 1) postnatal self-care; 2) family support for woman after childbirth; and 3) postnatal health care service for women with obesity.
Women with obesity need support from the health team and from their families after childbirth, when they are overwhelmed by the exhausting care for the newborn. The present study reveals how important it is for health care professionals to broaden their perception and care provided after childbirth for women with obesity so they may experience an improvement in their quality of health and of life.
