Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):399-404
DOI 10.1590/S0100-72032004000500009
OBJECTIVE: to observe if there is any alteration in the Dopplervelocimetry of the uterine arteries of nursing and not nursing women after the insertion of the copper T 380 intrauterine device (IUD). METHODS: prospective, analytical, self-paired clinical assay, with 100 patients in whom we evaluated the color doppler flow: resistance index (RI), pulsative index (PI) and systole/diastole (SD) ratio. Nursing and not nursing women were assessed before IUD insertion as well as 30 days (one cycle) and 90 days (three cycles) after the insertion. RESULTS: the values obtained in the uterine arteries before insertion were: RI: 0.9, PI: 2.4, and SD ratio: 10.0. The values 30 days after insertion were: RI: 0.9, PI: 2.5 and SD ratio: 10.7. After three cycles we found a value of 0.9 for RI, 2.5 for PI and 10.7 for SD ratio. The comparison of the results before and after the IUD insertion showed a p value of 0.51 for RI, of 0.37 for PI and of 0.51 for SD ratio, demonstrating that after the insertion of the IUD, there were no significant changes in Dopplervelocimetry. Also, there were not significant differences between nursing and not nursing women, concerning these parameters. CONCLUSIONS: the use of copper T 380 IUD has no effect on the Doppler indices of the uterine arteries of both nursing and not nursing women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):399-404
DOI 10.1590/S0100-72032004000500009
OBJECTIVE: to observe if there is any alteration in the Dopplervelocimetry of the uterine arteries of nursing and not nursing women after the insertion of the copper T 380 intrauterine device (IUD). METHODS: prospective, analytical, self-paired clinical assay, with 100 patients in whom we evaluated the color doppler flow: resistance index (RI), pulsative index (PI) and systole/diastole (SD) ratio. Nursing and not nursing women were assessed before IUD insertion as well as 30 days (one cycle) and 90 days (three cycles) after the insertion. RESULTS: the values obtained in the uterine arteries before insertion were: RI: 0.9, PI: 2.4, and SD ratio: 10.0. The values 30 days after insertion were: RI: 0.9, PI: 2.5 and SD ratio: 10.7. After three cycles we found a value of 0.9 for RI, 2.5 for PI and 10.7 for SD ratio. The comparison of the results before and after the IUD insertion showed a p value of 0.51 for RI, of 0.37 for PI and of 0.51 for SD ratio, demonstrating that after the insertion of the IUD, there were no significant changes in Dopplervelocimetry. Also, there were not significant differences between nursing and not nursing women, concerning these parameters. CONCLUSIONS: the use of copper T 380 IUD has no effect on the Doppler indices of the uterine arteries of both nursing and not nursing women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):405-410
DOI 10.1590/S0100-72032004000500010
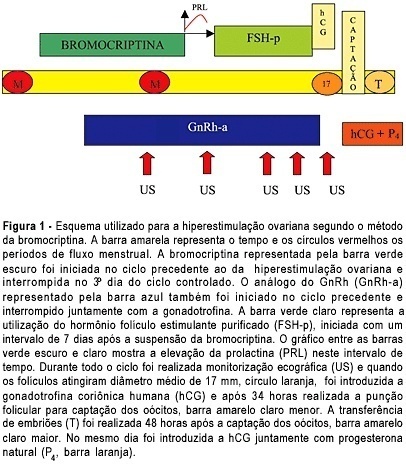
OBJECTIVE: to assess the ovarian response of poor responsive patients, submitted to the bromocriptine method. PACIENTS AND METHODS: a prospective clinical trial for the in vitro fertilization (IVF) program was performed in 10 poor responsive patients. Endocrinologically normal ovulatory women under 38 years old, who had previously failed in IVF due to poor response to ovarian stimulation with the traditional protocol, were submitted to the bromocriptine method in 12 cycles. They were given bromocriptine, a dopaminergic agonist, in the preceding cycle in order to stop the prolactin production. When the medication was removed at the beginning of the stimulation cycle, an elevation of seric prolactin by a rebound phenomenon was found. This optimized its seric concentration, improving the quality of oocytes and embryos. Serum prolactin and estradiol concentrations, number of follicles, number and quality of oocytes and cleaved embryos, fertilization and pregnancy rates were analyzed. RESULTS: there was a reduction in the dose of gonadotropin administered and in the duration of ovarian stimulation and an improvement in follicular recruitment, oocyte retrieval, embryo morphology, fertilization, and ongoing pregnancy rates. Fertilization rate was 77.7%, pregnancy rate was 44.4% and live baby rate was 25%. CONCLUSION: this study suggests that the bromocriptine method enhanced follicular recruitment and embryonic development, resulting in increased fertilization and pregnancy rates when compared with the traditional protocol for poor responsive patients. Studies with a large number of patients are necessary to confirm these results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):405-410
DOI 10.1590/S0100-72032004000500010
OBJECTIVE: to assess the ovarian response of poor responsive patients, submitted to the bromocriptine method. PACIENTS AND METHODS: a prospective clinical trial for the in vitro fertilization (IVF) program was performed in 10 poor responsive patients. Endocrinologically normal ovulatory women under 38 years old, who had previously failed in IVF due to poor response to ovarian stimulation with the traditional protocol, were submitted to the bromocriptine method in 12 cycles. They were given bromocriptine, a dopaminergic agonist, in the preceding cycle in order to stop the prolactin production. When the medication was removed at the beginning of the stimulation cycle, an elevation of seric prolactin by a rebound phenomenon was found. This optimized its seric concentration, improving the quality of oocytes and embryos. Serum prolactin and estradiol concentrations, number of follicles, number and quality of oocytes and cleaved embryos, fertilization and pregnancy rates were analyzed. RESULTS: there was a reduction in the dose of gonadotropin administered and in the duration of ovarian stimulation and an improvement in follicular recruitment, oocyte retrieval, embryo morphology, fertilization, and ongoing pregnancy rates. Fertilization rate was 77.7%, pregnancy rate was 44.4% and live baby rate was 25%. CONCLUSION: this study suggests that the bromocriptine method enhanced follicular recruitment and embryonic development, resulting in increased fertilization and pregnancy rates when compared with the traditional protocol for poor responsive patients. Studies with a large number of patients are necessary to confirm these results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):411-416
DOI 10.1590/S0100-72032004000500011
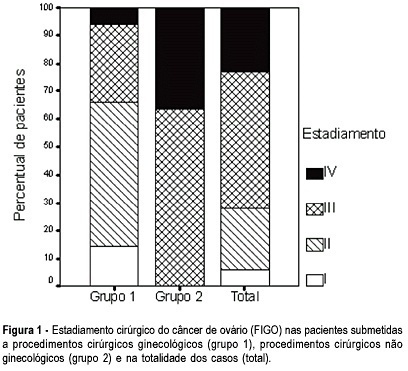
OBJECTIVE: to evaluate the incidence of non-gynecological surgical procedures used in the treatment of ovarian cancer, as well to describe their complications. METHODS: eighty-two patients with ages from 22 to 89 (mean = 54.1 ± 15.1 years), submitted to laparotomy for surgical treatment of ovarian cancer from February 1999 to October 2003 were retrospectively evaluated. This study included only patients with epithelial ovary carcinoma. The patients were divided into 2 groups, patients submitted exclusively to gynecological procedures and patients submitted to non-gynecological procedures. Statistical analysis was made with the Student's t-test or the chi-square test. RESULTS: 5 patients (6.1%) were in stage (FIGO) I, 18 (21.9%) in stage II, 40 (48.8%) in stage III, and 19 (23.2%) in stage IV. Non-gynecological procedures were done in 35 cases (42.7%), including: 17 colostomies, 16 enterectomies, 8 peritonectomies, 7 colectomies, 5 partial diaphragm resections, 4 partial cystectomies, 4 splenectomies, 2 ileostomies, and 1 hepatectomy. All patients submitted to non-gynecological procedures were included in stages III and IV. This group of patients underwent longer-lasting surgeries (5.3 ± 1.4 versus 3.1 + 0,0 h; p < 0.001). There was no significant difference between these two groups regarding hemotransfusion requirement (42,2 versus 40%; p = 0.512) and hospitalization time (11.5 ± 7.2 versus 10 ± 9.9 days; p = 0.454). Patients submitted to non-gynecological surgeries developed higher rates of postoperative complications (37 versus 17.1%; p = 0.042), and two of them (2.4%) died. CONCLUSION: non-gynecological surgical procedures are frequently used in the treatment of patients with ovarian cancer. These procedures are associated with a longer-lasting surgery and higher rates of postoperative complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):411-416
DOI 10.1590/S0100-72032004000500011
OBJECTIVE: to evaluate the incidence of non-gynecological surgical procedures used in the treatment of ovarian cancer, as well to describe their complications. METHODS: eighty-two patients with ages from 22 to 89 (mean = 54.1 ± 15.1 years), submitted to laparotomy for surgical treatment of ovarian cancer from February 1999 to October 2003 were retrospectively evaluated. This study included only patients with epithelial ovary carcinoma. The patients were divided into 2 groups, patients submitted exclusively to gynecological procedures and patients submitted to non-gynecological procedures. Statistical analysis was made with the Student's t-test or the chi-square test. RESULTS: 5 patients (6.1%) were in stage (FIGO) I, 18 (21.9%) in stage II, 40 (48.8%) in stage III, and 19 (23.2%) in stage IV. Non-gynecological procedures were done in 35 cases (42.7%), including: 17 colostomies, 16 enterectomies, 8 peritonectomies, 7 colectomies, 5 partial diaphragm resections, 4 partial cystectomies, 4 splenectomies, 2 ileostomies, and 1 hepatectomy. All patients submitted to non-gynecological procedures were included in stages III and IV. This group of patients underwent longer-lasting surgeries (5.3 ± 1.4 versus 3.1 + 0,0 h; p < 0.001). There was no significant difference between these two groups regarding hemotransfusion requirement (42,2 versus 40%; p = 0.512) and hospitalization time (11.5 ± 7.2 versus 10 ± 9.9 days; p = 0.454). Patients submitted to non-gynecological surgeries developed higher rates of postoperative complications (37 versus 17.1%; p = 0.042), and two of them (2.4%) died. CONCLUSION: non-gynecological surgical procedures are frequently used in the treatment of patients with ovarian cancer. These procedures are associated with a longer-lasting surgery and higher rates of postoperative complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):417-417
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):417-417
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):417-418
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(5):417-418