You searched for:"Ernesto Antonio Figueiró-Filho"
We found (14) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(11):820-825
To compare maternal and perinatal risk factors associated with complete uterine rupture and uterine dehiscence.
Cross-sectional study of patients with uterine rupture/dehiscence from January 1998 to December 2017 (30 years) admitted at the Labor and Delivery Unit of a tertiary teaching hospital in Canada.
There were 174 (0.1%) cases of uterine disruption (29 ruptures and 145 cases of dehiscence) out of 169,356 deliveries. There were associations between dehiscence and multiparity (odds ratio [OR]: 3.2; p=0.02), elevated maternal body mass index (BMI; OR: 3.4; p=0.02), attempt of vaginal birth after a cesarian section (OR: 2.9; p=0.05) and 5-minute low Apgar score (OR: 5.9; p<0.001). Uterine rupture was associated with preterm deliveries (36.5 ± 4.9 versus 38.2 ± 2.9; p=0.006), postpartum hemorrhage (OR: 13.9; p<0.001), hysterectomy (OR: 23.0; p=0.002), and stillbirth (OR: 8.2; p<0.001). There were no associations between uterine rupture and maternal age, gestational age, onset of labor, spontaneous or artificial rupture of membranes, use of oxytocin, type of uterine incision, and birthweight.
This large cohort demonstrated that there are different risk factors associated with either uterine rupture or dehiscence. Uterine rupture still represents a great threat to fetal-maternal health and, differently from the common belief, uterine dehiscence can also compromise perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(11):820-825
To compare maternal and perinatal risk factors associated with complete uterine rupture and uterine dehiscence.
Cross-sectional study of patients with uterine rupture/dehiscence from January 1998 to December 2017 (30 years) admitted at the Labor and Delivery Unit of a tertiary teaching hospital in Canada.
There were 174 (0.1%) cases of uterine disruption (29 ruptures and 145 cases of dehiscence) out of 169,356 deliveries. There were associations between dehiscence and multiparity (odds ratio [OR]: 3.2; p=0.02), elevated maternal body mass index (BMI; OR: 3.4; p=0.02), attempt of vaginal birth after a cesarian section (OR: 2.9; p=0.05) and 5-minute low Apgar score (OR: 5.9; p<0.001). Uterine rupture was associated with preterm deliveries (36.5 ± 4.9 versus 38.2 ± 2.9; p=0.006), postpartum hemorrhage (OR: 13.9; p<0.001), hysterectomy (OR: 23.0; p=0.002), and stillbirth (OR: 8.2; p<0.001). There were no associations between uterine rupture and maternal age, gestational age, onset of labor, spontaneous or artificial rupture of membranes, use of oxytocin, type of uterine incision, and birthweight.
This large cohort demonstrated that there are different risk factors associated with either uterine rupture or dehiscence. Uterine rupture still represents a great threat to fetal-maternal health and, differently from the common belief, uterine dehiscence can also compromise perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(1):10-16
DOI 10.1590/S0100-72032014000100004
To investigate the association of perinatal variables with the birth of very low birth weight (VLBW) preterm newborns.
It was a retrospective study of the medical records of infants born after spontaneous preterm labor with admission to a neonatal intensive care unit. Preterm infants were divided into two groups: very low birth weight (VLBW) group (weight <1,500 g) and low birth weight (LBW) group (weight ≥1,500 g and <2,500 g). Prenatal variables such as maternal complications during pregnancy and childbirth/postpartum, and fetal/neonatal complications were investigated. Statistical analysis was performed using the Fisher exact test or χ2 test, with calculation of relative risk (RR), and the Student t test for comparison of group means, with the level of significance set at p≤0.05.
Hemorrhagic comorbidities (p=0.006; RR=1.2) and hypertension (p=0.04; RR=1.5), surgical delivery (p=0.001; RR=0.5), gestational age <33 weeks (p< 0.001; RR=16.7) and Apgar score at 1st and 5th minute (p=0.006; RR=1.6; p=0.01; RR=1.9) were associated with the occurrence of VLBW. Infants with VLBW had a significant association with the occurrence of metabolic comorbidities (p=0.01; RR=1.8), neurological (p=0.01; RR=1.7) and infectious diseases (p=0.001; RR=1.9), hospitalization >4 weeks (p=0.02; RR=1.8) and early neonatal death (p=0.0001; RR=2.9).
Factors such as hypertension and bleeding comorbidities during delivery and management of gestational age of less than 33 weeks were associated with the birth of VLBW newborns. This group of infants also showed higher RR for the occurrence of early neonatal death.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(1):10-16
DOI 10.1590/S0100-72032014000100004
To investigate the association of perinatal variables with the birth of very low birth weight (VLBW) preterm newborns.
It was a retrospective study of the medical records of infants born after spontaneous preterm labor with admission to a neonatal intensive care unit. Preterm infants were divided into two groups: very low birth weight (VLBW) group (weight <1,500 g) and low birth weight (LBW) group (weight ≥1,500 g and <2,500 g). Prenatal variables such as maternal complications during pregnancy and childbirth/postpartum, and fetal/neonatal complications were investigated. Statistical analysis was performed using the Fisher exact test or χ2 test, with calculation of relative risk (RR), and the Student t test for comparison of group means, with the level of significance set at p≤0.05.
Hemorrhagic comorbidities (p=0.006; RR=1.2) and hypertension (p=0.04; RR=1.5), surgical delivery (p=0.001; RR=0.5), gestational age <33 weeks (p< 0.001; RR=16.7) and Apgar score at 1st and 5th minute (p=0.006; RR=1.6; p=0.01; RR=1.9) were associated with the occurrence of VLBW. Infants with VLBW had a significant association with the occurrence of metabolic comorbidities (p=0.01; RR=1.8), neurological (p=0.01; RR=1.7) and infectious diseases (p=0.001; RR=1.9), hospitalization >4 weeks (p=0.02; RR=1.8) and early neonatal death (p=0.0001; RR=2.9).
Factors such as hypertension and bleeding comorbidities during delivery and management of gestational age of less than 33 weeks were associated with the birth of VLBW newborns. This group of infants also showed higher RR for the occurrence of early neonatal death.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):459-465
DOI 10.1590/S0100-72032012001000005
PURPOSES: To assess whether an enoxaparin-based intervention using a score system was effective in improving perinatal outcome in women with thrombophilia. METHODS: Study Design: Prospective, not randomized, uncontrolled, performed at a Clinic of High-Risk Pregnancy from November 2009 to November 2011. We included women with a diagnosis and therapeutic intervention for thrombophilia acquired and/or inherited in the current pregnancy. The obstetric and perinatal outcomes of pregnant women before the intervention were compared with outcomes after the intervention, and statistically analyzed using the χ2 test with Yates correction, considered significant when p<0.05. The initial dose of low-molecular-weight Heparin (LMWH) was guided by a scoring system based on the clinical and gestational history of the patients and screening tests for acquired and/or inherited thrombophilia. RESULTS: We included 84 pregnant women with 175 pregnancies before diagnosis, 20.0% of which resulted in fetal ou perinatal death, 40.0% resulted in abortion, 17.7% developed preeclampsia/eclampsia, 10.3% resulted in full-term births, and 29.7% in premature births. In the 84 pregnancies after intervention, 6.0% resulted in fetal ou perinatal death, 1.2% in abortion, 4.8% developed preeclampsia/eclampsia, 22.6% resulted in premature birth, and 70.2% in full-term birth. A significant reduction in the rate of stillbirths/perinatal death (p<0.05) and abortion (p<0.0001) and a significant increase (p<0.05) in the number of live births were observed after intervention. CONCLUSION: Enoxaparin-based intervention using a score system in pregnant women with thrombophilia is effective in improving perinatal outcome.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(1):40-46
DOI 10.1590/S0100-72032012000100008
PURPOSE: To determine the frequency and the association of serum markers for inherited and acquired thrombophilias in pregnant women with a history of severe pre-eclampsia in previous pregnancies. METHODS: Case-control study consisting of 81 pregnant women with a history of severe pre-eclampsia in previous pregnancies (study group) and 32 women with no history of severe pre-eclampsia in previous pregnancies (control group). The presence of inherited thrombophilia and antiphospholipid antibodies was screened in both groups. We used the chi-square test with Yates correction to assess associations and calculate the relative risks. RESULTS: The presence of thrombophilia was detected in 60.0% of patients with a previous history of pre-eclampsia and in 6.0% of the control patients. A significant association was found between pre-eclampsia in a previous pregnancy and the presence of markers for hereditary thrombophilia/antiphospholipid antibodies (p<0.05). The relative risk to develop pre-eclampsia was found to be 1.57 (1.34
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(1):40-46
DOI 10.1590/S0100-72032012000100008
PURPOSE: To determine the frequency and the association of serum markers for inherited and acquired thrombophilias in pregnant women with a history of severe pre-eclampsia in previous pregnancies. METHODS: Case-control study consisting of 81 pregnant women with a history of severe pre-eclampsia in previous pregnancies (study group) and 32 women with no history of severe pre-eclampsia in previous pregnancies (control group). The presence of inherited thrombophilia and antiphospholipid antibodies was screened in both groups. We used the chi-square test with Yates correction to assess associations and calculate the relative risks. RESULTS: The presence of thrombophilia was detected in 60.0% of patients with a previous history of pre-eclampsia and in 6.0% of the control patients. A significant association was found between pre-eclampsia in a previous pregnancy and the presence of markers for hereditary thrombophilia/antiphospholipid antibodies (p<0.05). The relative risk to develop pre-eclampsia was found to be 1.57 (1.34
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(11):561-567
DOI 10.1590/S0100-72032007001100003
PURPOSE: to verify the association of abortion, recurrent fetal loss, miscarriage and severe pre-eclampsia with the presence of hereditary thrombophilias and antiphospholipid antibodies in pregnant women. METHODS: observational and transverse study of 48 pregnant women with past medical record of miscarriage, repeated abortion and fetal loss story (AB Group) and severe pre-eclampsia (PE Group), attended to in the High Risk Pregnancy Ambulatory of the Faculdade de Medicina (Famed) from the Universidade Federal de Mato Grosso do Sul (UFMS) from November 2006 to July 2007. The pregnant women of both groups were screened for the presence of antiphospholipid antibodies (anticardiolipin IgG and IgM, lupic anticoagulant and anti-beta2-glycoprotein I) and hereditary thrombophilias (protein C and S deficiency, antithrombin deficiency, hyperhomocysteinemia and factor V Leiden mutation). The laboratorial screening was performed during the pregnancy. The parametric data (maternal age and parity) were analyzed with Student’s tau test. The non-parametric data (presence/absence of hereditary thrombophilias and antiphospholipid antibodies, presence/absence of pre-eclampsia, fetal loss, miscarriage and repeated abortion) were analyzed with Fisher’s exact test in contingency tables. It was considered significant the association with p value <0.05. RESULTS: out of the 48 pregnant women, 31 (65%) were included in AB Group and 17 (35%) in PE Group. There was no significant difference between maternal age and parity within the groups. There was significant statistical association between recurrent fetal loss, recurrent abortions and previous miscarriages and maternal hereditary thrombophilias (p<0.05). There was no statistical association between the AB Group and the presence of antiphospholipid antibodies. Neither there were associations of the PE Group with maternal hereditary thrombophilias and the presence of antiphospholipid antibodies. CONCLUSIONS: the data obtained suggest routine laboratorial investigation for hereditary thrombophilias in pregnant women with previous obstetrical story of recurrent fetal loss, repeated abortion and miscarriage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(11):561-567
DOI 10.1590/S0100-72032007001100003
PURPOSE: to verify the association of abortion, recurrent fetal loss, miscarriage and severe pre-eclampsia with the presence of hereditary thrombophilias and antiphospholipid antibodies in pregnant women. METHODS: observational and transverse study of 48 pregnant women with past medical record of miscarriage, repeated abortion and fetal loss story (AB Group) and severe pre-eclampsia (PE Group), attended to in the High Risk Pregnancy Ambulatory of the Faculdade de Medicina (Famed) from the Universidade Federal de Mato Grosso do Sul (UFMS) from November 2006 to July 2007. The pregnant women of both groups were screened for the presence of antiphospholipid antibodies (anticardiolipin IgG and IgM, lupic anticoagulant and anti-beta2-glycoprotein I) and hereditary thrombophilias (protein C and S deficiency, antithrombin deficiency, hyperhomocysteinemia and factor V Leiden mutation). The laboratorial screening was performed during the pregnancy. The parametric data (maternal age and parity) were analyzed with Student’s tau test. The non-parametric data (presence/absence of hereditary thrombophilias and antiphospholipid antibodies, presence/absence of pre-eclampsia, fetal loss, miscarriage and repeated abortion) were analyzed with Fisher’s exact test in contingency tables. It was considered significant the association with p value <0.05. RESULTS: out of the 48 pregnant women, 31 (65%) were included in AB Group and 17 (35%) in PE Group. There was no significant difference between maternal age and parity within the groups. There was significant statistical association between recurrent fetal loss, recurrent abortions and previous miscarriages and maternal hereditary thrombophilias (p<0.05). There was no statistical association between the AB Group and the presence of antiphospholipid antibodies. Neither there were associations of the PE Group with maternal hereditary thrombophilias and the presence of antiphospholipid antibodies. CONCLUSIONS: the data obtained suggest routine laboratorial investigation for hereditary thrombophilias in pregnant women with previous obstetrical story of recurrent fetal loss, repeated abortion and miscarriage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(12):719-725
DOI 10.1590/S0100-72032005001200003
PURPOSE: to evaluate the prevalence, epidemiological profile (age and origin) and vertical transmission rate of HTLV I/II infection in pregnant women screened by the Pregnant Protection Program of the State of Mato Grosso do Sul Brazil. METHODS: it is a descriptive and transversal study of 32,512 pregnant women submitted to a prenatal screening from November 2002 to October 2003. HTLV I/II infection was diagnosed in all pregnant women by ELISA, confirmed by Western blot and PCR. Congenital HTLV infection was investigated by ELISA test, Western blot and PCR performed on the child's blood sample. The associations between data (age, origin and HTLV infection) were statistically analyzed by the chi2 test considering p<0.05 to reject the null hypothesis. RESULTS: a prevalence of 0.1% (37) 0.1% HTLV I/II among 32,512 pregnant women was found. The mean age of the infected women was 25.4 ± 6.4 years, and 78.4% of them were from other areas than the capital. There was no association between maternal age and the patients' origin and infection. In all the eight evaluated newborns, which represented 21.6% of the sample, HTLV I/II serum antibodies were found. Only one newborn infant was breast-fed. CONCLUSIONS : HTLV I/II prevalence among pregnant women of the State of Mato Grosso do Sul Brazil was lower than the rates reported by endemic HTLV countries. This rate was almost the same as that described for non-endemic areas and in some Brazilian reports. The vertical transmission rate of HTLV I/II was 100%, in spite of breast-feeding having been proscribed. Improving the follow-up of the pregnant women and their newborns in the State is mandatory, since only a few infants were investigated.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(12):719-725
DOI 10.1590/S0100-72032005001200003
PURPOSE: to evaluate the prevalence, epidemiological profile (age and origin) and vertical transmission rate of HTLV I/II infection in pregnant women screened by the Pregnant Protection Program of the State of Mato Grosso do Sul Brazil. METHODS: it is a descriptive and transversal study of 32,512 pregnant women submitted to a prenatal screening from November 2002 to October 2003. HTLV I/II infection was diagnosed in all pregnant women by ELISA, confirmed by Western blot and PCR. Congenital HTLV infection was investigated by ELISA test, Western blot and PCR performed on the child's blood sample. The associations between data (age, origin and HTLV infection) were statistically analyzed by the chi2 test considering p<0.05 to reject the null hypothesis. RESULTS: a prevalence of 0.1% (37) 0.1% HTLV I/II among 32,512 pregnant women was found. The mean age of the infected women was 25.4 ± 6.4 years, and 78.4% of them were from other areas than the capital. There was no association between maternal age and the patients' origin and infection. In all the eight evaluated newborns, which represented 21.6% of the sample, HTLV I/II serum antibodies were found. Only one newborn infant was breast-fed. CONCLUSIONS : HTLV I/II prevalence among pregnant women of the State of Mato Grosso do Sul Brazil was lower than the rates reported by endemic HTLV countries. This rate was almost the same as that described for non-endemic areas and in some Brazilian reports. The vertical transmission rate of HTLV I/II was 100%, in spite of breast-feeding having been proscribed. Improving the follow-up of the pregnant women and their newborns in the State is mandatory, since only a few infants were investigated.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):442-449
DOI 10.1590/S0100-72032005000800002
PURPOSE: to establish the frequency of acute toxoplasmosis in pregnant women, vertical transmission rate and the perinatal results of the infected fetuses and also to evaluate the relationship between the most used maternal-fetal diagnostic tests for toxoplasmosis during pregnancy and the relationship between age and acute toxoplasmosis infection during pregnancy. METHODS: longitudinal prospective study of 32,512 pregnant women attended by The Pregnancy Protection Program of the State of Mato Grosso do Sul - Brazil, from November 2002 to October 2003. ELISA (IgG and IgM) and IgG avidity test were performed for maternal diagnosis and amniotic fluid PCR for fetal investigation of the infection. The relationship between data was analyzed statistically by the chi2 or two-sided Fisher's exact test in contingency tables. RESULTS: a 0.42% frequency of acute Toxoplasma gondii infection among pregnant population was found, where 92% were previously exposed and 8% were susceptible. Among IgM-positive pregnant women, the age ranged from 14 to 39 years, with a mean of 23±5.9 years. There was no statistically significant relationship between age and maternal acute T. gondii infection (p=0.73). The vertical transmission rate was 3.9%. A statistically significant relationship was shown (p=0.001) between a lower avidity IgG test (<30%) and the presence of fetal infection and a higher IgG avidity test (>60%) and the absence of fetal infection. There was a statistically significant association (p=0.001) between fetal infection (amniotic fluid PCR) and neonatal infection. CONCLUSIONS: maternal acute toxoplasmosis frequency was lower than the Brazilian national parameters, whereas vertical transmission rate did not differ from the rates found in other studies. The IgG avidity test, when associated with gestational age and the examination date, was useful to evaluate the therapeutical options and to consider the risk of vertical transmission when performed before 12 weeks. Positive PCR in amniotic fluid showed a positive relationship with the worst neonatal prognosis, being a specific method in diagnosing intrauterine fetal infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(8):442-449
DOI 10.1590/S0100-72032005000800002
PURPOSE: to establish the frequency of acute toxoplasmosis in pregnant women, vertical transmission rate and the perinatal results of the infected fetuses and also to evaluate the relationship between the most used maternal-fetal diagnostic tests for toxoplasmosis during pregnancy and the relationship between age and acute toxoplasmosis infection during pregnancy. METHODS: longitudinal prospective study of 32,512 pregnant women attended by The Pregnancy Protection Program of the State of Mato Grosso do Sul - Brazil, from November 2002 to October 2003. ELISA (IgG and IgM) and IgG avidity test were performed for maternal diagnosis and amniotic fluid PCR for fetal investigation of the infection. The relationship between data was analyzed statistically by the chi2 or two-sided Fisher's exact test in contingency tables. RESULTS: a 0.42% frequency of acute Toxoplasma gondii infection among pregnant population was found, where 92% were previously exposed and 8% were susceptible. Among IgM-positive pregnant women, the age ranged from 14 to 39 years, with a mean of 23±5.9 years. There was no statistically significant relationship between age and maternal acute T. gondii infection (p=0.73). The vertical transmission rate was 3.9%. A statistically significant relationship was shown (p=0.001) between a lower avidity IgG test (<30%) and the presence of fetal infection and a higher IgG avidity test (>60%) and the absence of fetal infection. There was a statistically significant association (p=0.001) between fetal infection (amniotic fluid PCR) and neonatal infection. CONCLUSIONS: maternal acute toxoplasmosis frequency was lower than the Brazilian national parameters, whereas vertical transmission rate did not differ from the rates found in other studies. The IgG avidity test, when associated with gestational age and the examination date, was useful to evaluate the therapeutical options and to consider the risk of vertical transmission when performed before 12 weeks. Positive PCR in amniotic fluid showed a positive relationship with the worst neonatal prognosis, being a specific method in diagnosing intrauterine fetal infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
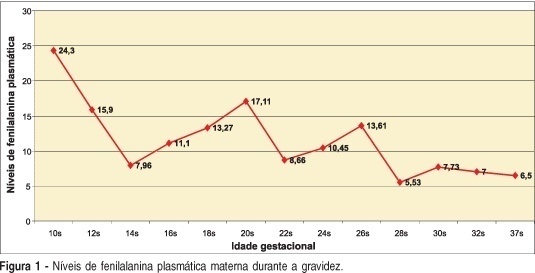
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.