Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):60-65
The aim of this study was to evaluate which risk factors may lead patients with gestational diabetes mellitus to cesarean delivery.
This was a retrospective, descriptive study. The subjects of the study were pregnant women with gestational diabetes mellitus attending a public maternity hospital in the south of Brazil. The primary outcomes assessed were based on maternal and fetal characteristics. The data were correlated using an odds ratio (OR) with a 95% confidence interval (95%CI), calculated using multinomial logistic regression.
A total of 392 patients with gestational diabetes mellitus were analyzed, and 57.4% of them had cesarean deliveries. Among the maternal characteristics, the mean age of the patients and the pregestational body mass index were greater when a cesarean delivery was performed (p = 0.029 and p < 0.01 respectively). Gestational age at birth, newborn weight, weight class according to gestational age, and Apgar score were not significant. The analysis of the OR showed that the chance of cesarean delivery was 2.25 times (95%CI = 1.49-2.39) greater if the pregnant woman was obese, 4.6 times (95%CI = 3.017-7.150) greater if she was a primigravida, and 5.2 times (95% CI = 2.702-10.003) greater if she had a previous cesarean delivery. The other parameters analyzed showed no differences.
The factors that led to an increase in the occurrence of cesarean deliveries included history of a prior cesarean section, first pregnancy, and obesity.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):60-65
The aim of this study was to evaluate which risk factors may lead patients with gestational diabetes mellitus to cesarean delivery.
This was a retrospective, descriptive study. The subjects of the study were pregnant women with gestational diabetes mellitus attending a public maternity hospital in the south of Brazil. The primary outcomes assessed were based on maternal and fetal characteristics. The data were correlated using an odds ratio (OR) with a 95% confidence interval (95%CI), calculated using multinomial logistic regression.
A total of 392 patients with gestational diabetes mellitus were analyzed, and 57.4% of them had cesarean deliveries. Among the maternal characteristics, the mean age of the patients and the pregestational body mass index were greater when a cesarean delivery was performed (p = 0.029 and p < 0.01 respectively). Gestational age at birth, newborn weight, weight class according to gestational age, and Apgar score were not significant. The analysis of the OR showed that the chance of cesarean delivery was 2.25 times (95%CI = 1.49-2.39) greater if the pregnant woman was obese, 4.6 times (95%CI = 3.017-7.150) greater if she was a primigravida, and 5.2 times (95% CI = 2.702-10.003) greater if she had a previous cesarean delivery. The other parameters analyzed showed no differences.
The factors that led to an increase in the occurrence of cesarean deliveries included history of a prior cesarean section, first pregnancy, and obesity.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):53-59
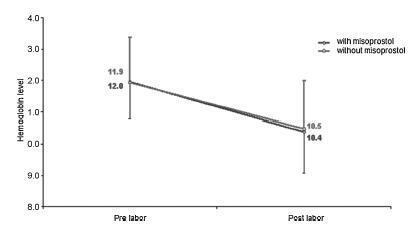
To evaluate blood loss during misoprostol-induced vaginal births and during cesarean sections after attempted misoprostol induction.
We conducted a prospective observational study in 101 pregnant women indicated for labor induction; pre- and postpartum hemoglobin levels were measured to estimate blood loss during delivery. Labor was induced by administering 25 μg vaginal misoprostol every 6 hours (with a maximum of 6 doses). The control group included 30 patients who spontaneously entered labor, and 30 patients who underwent elective cesarean section. Pre- and postpartum hemoglobin levels were evaluated using the analysis of variance for repeated measurements, showing the effects of time (pre- and postpartum) and of the group (with and withoutmisoprostol administration).
Therewere significant differences between pre- and postpartum hemoglobin levels (p < 0.0001) with regard to misoprostol-induced vaginal deliveries (1.6 ± 1.4 mg/dL), non-induced vaginal deliveries (1.4 ± 1.0 mg/dL), cesarean sections after attempted misoprostol induction (1.5 ± 1.0 mg/dL), and elective cesarean deliveries (1.8 ± 1.1 mg/dL). However, the differences were proportional between the groups with and without misoprostol administration, for both cesarean (p = 0.6845) and vaginal deliveries (p = 0.2694).
Labor induction using misoprostol did not affect blood loss during delivery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):53-59
To evaluate blood loss during misoprostol-induced vaginal births and during cesarean sections after attempted misoprostol induction.
We conducted a prospective observational study in 101 pregnant women indicated for labor induction; pre- and postpartum hemoglobin levels were measured to estimate blood loss during delivery. Labor was induced by administering 25 μg vaginal misoprostol every 6 hours (with a maximum of 6 doses). The control group included 30 patients who spontaneously entered labor, and 30 patients who underwent elective cesarean section. Pre- and postpartum hemoglobin levels were evaluated using the analysis of variance for repeated measurements, showing the effects of time (pre- and postpartum) and of the group (with and withoutmisoprostol administration).
Therewere significant differences between pre- and postpartum hemoglobin levels (p < 0.0001) with regard to misoprostol-induced vaginal deliveries (1.6 ± 1.4 mg/dL), non-induced vaginal deliveries (1.4 ± 1.0 mg/dL), cesarean sections after attempted misoprostol induction (1.5 ± 1.0 mg/dL), and elective cesarean deliveries (1.8 ± 1.1 mg/dL). However, the differences were proportional between the groups with and without misoprostol administration, for both cesarean (p = 0.6845) and vaginal deliveries (p = 0.2694).
Labor induction using misoprostol did not affect blood loss during delivery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):44-53
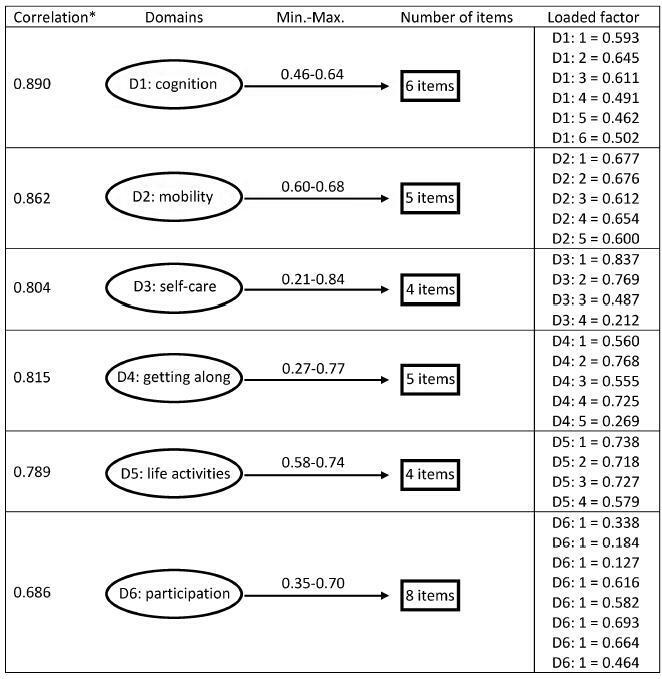
To validate the translation and adaptation to Brazilian Portuguese of 36 items from the World Health Organizaton Disability Assessment Schedule 2.0 (WHODAS 2.0), regarding their content and structure (construct), in a female population after pregnancy.
This is a validation of an instrument for the evaluation of disability and functioning and an assessment of its psychometric properties, performed in a tertiary maternity and a referral center specialized in high-risk pregnancies in Brazil. A sample of 638 women in different postpartum periods who had either a normal or a complicated pregnancy was included. The structure was evaluated by exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), while the content and relationships among the domains were assessed through Pearson's correlation coefficient. The sociodemographic characteristics were identified, and the mean scores with their standard deviations for the 36 questions of the WHODAS 2.0 were calculated. The internal consistency was evaluated byCronbach's α.
Cronbach's α was higher than 0.79 for both sets of questons of the questionnaire. The EFA and CFA for the main 32 questions exhibited a total variance of 54.7% (Kaiser-Meyer-Olkin [KMO] measure of sampling adequacy = 0.934; p < 0.001) and 53.47% (KMO = 0.934; p < 0.001) respectively. There was a significant correlation among the 6 domains (r = 0.571-0.876), and a moderate correlation among all domains (r = 0.476-0.694).
The version of the WHODAS 2.0 instrument adapted to Brazilian Portuguese showed good psychometric properties in this sample, and therefore could be applied to populations of women regarding their reproductive history.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(2):44-53
To validate the translation and adaptation to Brazilian Portuguese of 36 items from the World Health Organizaton Disability Assessment Schedule 2.0 (WHODAS 2.0), regarding their content and structure (construct), in a female population after pregnancy.
This is a validation of an instrument for the evaluation of disability and functioning and an assessment of its psychometric properties, performed in a tertiary maternity and a referral center specialized in high-risk pregnancies in Brazil. A sample of 638 women in different postpartum periods who had either a normal or a complicated pregnancy was included. The structure was evaluated by exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), while the content and relationships among the domains were assessed through Pearson's correlation coefficient. The sociodemographic characteristics were identified, and the mean scores with their standard deviations for the 36 questions of the WHODAS 2.0 were calculated. The internal consistency was evaluated byCronbach's α.
Cronbach's α was higher than 0.79 for both sets of questons of the questionnaire. The EFA and CFA for the main 32 questions exhibited a total variance of 54.7% (Kaiser-Meyer-Olkin [KMO] measure of sampling adequacy = 0.934; p < 0.001) and 53.47% (KMO = 0.934; p < 0.001) respectively. There was a significant correlation among the 6 domains (r = 0.571-0.876), and a moderate correlation among all domains (r = 0.476-0.694).
The version of the WHODAS 2.0 instrument adapted to Brazilian Portuguese showed good psychometric properties in this sample, and therefore could be applied to populations of women regarding their reproductive history.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):600-608
Female sexual dysfunction is a complex and common condition that affects women, and the relationship between sexual function and dyslipidemia is poorly studied. This study aims to assess this relationship in the reproductive life women in the menacme who use combined oral contraceptives (COCs) .
A total of 49 healthy women who were sexually active received COC pills that contained ethinylestradiol 30 mcg (EE30) plus levonorgestrel 150 mcg (LNG150). The women were divided into two groups according to their lipid profiles. Dyslipidemia was defined as a high-density lipoprotein (HDL) level < 50 mg/dL or a low-density lipoprotein (LDL) level > 130 mg/dL. Sexual function was assessed using the Female Sexual Function Index (FSFI) Questionnaire. Lipid and lipoprotein parameters were obtained at baseline and after the sixth cycle.
After six cycles of the COCs, the total cholesterol and LDL cholesterol levels in the women with a LDL level > 130 mg/dL decreased by 14.7% and 22.1% respectively. In the women with a HDL level < 50 mg/dL at baseline, the HDL level increased by 15.5% at the end of the study. The arousal and orgasm domains and the FSFI total scores significantly increased in women with and without dyslipidemia. The desire and satisfaction domains increased only in the group without dyslipidemia at the end of the treatment period.
The EE30/LNG150 formulation increased the sexual function and it was only positively correlated with the HDL cholesterol level. These data indicated a low correlation between sexual function and the changes in the lipid and lipoprotein metabolism.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):600-608
Female sexual dysfunction is a complex and common condition that affects women, and the relationship between sexual function and dyslipidemia is poorly studied. This study aims to assess this relationship in the reproductive life women in the menacme who use combined oral contraceptives (COCs) .
A total of 49 healthy women who were sexually active received COC pills that contained ethinylestradiol 30 mcg (EE30) plus levonorgestrel 150 mcg (LNG150). The women were divided into two groups according to their lipid profiles. Dyslipidemia was defined as a high-density lipoprotein (HDL) level < 50 mg/dL or a low-density lipoprotein (LDL) level > 130 mg/dL. Sexual function was assessed using the Female Sexual Function Index (FSFI) Questionnaire. Lipid and lipoprotein parameters were obtained at baseline and after the sixth cycle.
After six cycles of the COCs, the total cholesterol and LDL cholesterol levels in the women with a LDL level > 130 mg/dL decreased by 14.7% and 22.1% respectively. In the women with a HDL level < 50 mg/dL at baseline, the HDL level increased by 15.5% at the end of the study. The arousal and orgasm domains and the FSFI total scores significantly increased in women with and without dyslipidemia. The desire and satisfaction domains increased only in the group without dyslipidemia at the end of the treatment period.
The EE30/LNG150 formulation increased the sexual function and it was only positively correlated with the HDL cholesterol level. These data indicated a low correlation between sexual function and the changes in the lipid and lipoprotein metabolism.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):593-599
To evaluate the antifungal susceptibility profile of the aqueous extract of the bark of Schinus terebinthifolius Raddi against the strains of the genus Candida.
By using the disk diffusion method, 50 samples of the genus Candida (Candida albicans; Candida krusei; Candida glabrata; and Candida tropicalis), isolated from patients receiving treatment at Hospital Santa Casa de Misericórdia de São Paulo, and 1 American Type Culture Collection (ATCC) sample of each species were tested against: the isolated aqueous extract of the bark of Schinus terebinthifolius Raddi, isolated nystatin, and the association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi.
There were no significant differences regarding the different strains of Candida tested. In the presence of the aqueous extract of Schinus terebinthifolius Raddi, no inhibition halo was visible. Isolated nystatin formed an inhibition halo measuring respectively 18.50 mm and 19.50 mm for the Candida albicans species and the others referred to as non-Candida albicans (Candida krusei; Candida glabrata; and Candida tropicalis). The association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi resulted in inhibition halos measuring 14.25 mm and 16.50 mm respectively. The comparisons of these results are statistically significant (p < 0,001).
The aqueous extract of Schinus terebinthifolius Raddi showed no antifun-gal activity in vitro against the strains tested, whereas the association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi caused a decrease in the inhibition halo when compared with isolated nystatin.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):593-599
To evaluate the antifungal susceptibility profile of the aqueous extract of the bark of Schinus terebinthifolius Raddi against the strains of the genus Candida.
By using the disk diffusion method, 50 samples of the genus Candida (Candida albicans; Candida krusei; Candida glabrata; and Candida tropicalis), isolated from patients receiving treatment at Hospital Santa Casa de Misericórdia de São Paulo, and 1 American Type Culture Collection (ATCC) sample of each species were tested against: the isolated aqueous extract of the bark of Schinus terebinthifolius Raddi, isolated nystatin, and the association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi.
There were no significant differences regarding the different strains of Candida tested. In the presence of the aqueous extract of Schinus terebinthifolius Raddi, no inhibition halo was visible. Isolated nystatin formed an inhibition halo measuring respectively 18.50 mm and 19.50 mm for the Candida albicans species and the others referred to as non-Candida albicans (Candida krusei; Candida glabrata; and Candida tropicalis). The association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi resulted in inhibition halos measuring 14.25 mm and 16.50 mm respectively. The comparisons of these results are statistically significant (p < 0,001).
The aqueous extract of Schinus terebinthifolius Raddi showed no antifun-gal activity in vitro against the strains tested, whereas the association of nystatin and the aqueous extract of Schinus terebinthifolius Raddi caused a decrease in the inhibition halo when compared with isolated nystatin.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):585-588
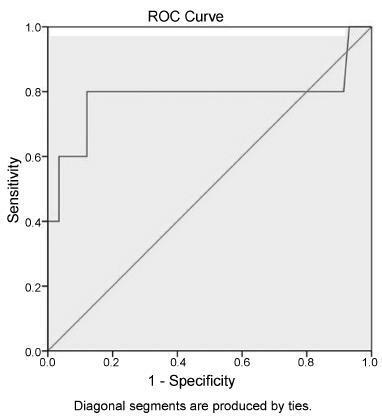
Analyzing if the sonographic evaluation of the cervix (cervical shortening) is a prognostic marker for vaginal delivery.
Women who underwent labor induction by using dinoprostone were enrolled. Before the induction and three hours after it, the cervical length was measured by ultrasonography to obtain the cervical shortening. The cervical shortening was introduced in logistic regression models among independent variables and for calculating receiver operating characteristic (ROC) curves.
Each centimeter in the cervical shortening increases the odds of vaginal delivery in 24.4% within 6 hours; in 16.1% within 24 hours; and in 10.5% within 48 hours. The best predictions for vaginal delivery are achieved for births within 6 and 24 hours, while the cervical shortening poorly predicts vaginal delivery within 48 hours.
The greater the cervical shortening 3 hours after labor induction, the higher the likelihood of vaginal delivery within 6, 24 and 48 hours.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):585-588
Analyzing if the sonographic evaluation of the cervix (cervical shortening) is a prognostic marker for vaginal delivery.
Women who underwent labor induction by using dinoprostone were enrolled. Before the induction and three hours after it, the cervical length was measured by ultrasonography to obtain the cervical shortening. The cervical shortening was introduced in logistic regression models among independent variables and for calculating receiver operating characteristic (ROC) curves.
Each centimeter in the cervical shortening increases the odds of vaginal delivery in 24.4% within 6 hours; in 16.1% within 24 hours; and in 10.5% within 48 hours. The best predictions for vaginal delivery are achieved for births within 6 and 24 hours, while the cervical shortening poorly predicts vaginal delivery within 48 hours.
The greater the cervical shortening 3 hours after labor induction, the higher the likelihood of vaginal delivery within 6, 24 and 48 hours.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):589-592
We speculate that genetic racial disparity exists in fetal life and can be detected by modern computerized cardiotocography (cCTG) .
This is a retrospective study comparing the results of the cCTG of pregnant patients at 37-42 weeks according to the parental ethnicity (black versus white). A cCTG was performed to analyze the variables of fetal heart rate (FHR). The cCTG variables analyzed were: percentage of signal loss; number of contractions; basal FHR; number of accelerations; number of decelerations; length of high variation episodes; short-term variability (STV); total trace duration time; and number of fetal active movements. Non-stress test (NST) parameters in the two groups were compared using the Mann-Whitney test for continuous data, and the Chi-square test for categorical variables.
We found a significantly lower number of active fetal movements (p 1/4 0.007) and longer periods of low variation (p 1/4 0.047) in the cCTG of black patients when compared with white patients.
In conclusion, identifying the factors responsible for the variance in the objective analysis of CTG results is important to improve the outcomes of patients. Our study lends further evidence as to the importance of ethnicity in clinical cCTG interpretation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):589-592
We speculate that genetic racial disparity exists in fetal life and can be detected by modern computerized cardiotocography (cCTG) .
This is a retrospective study comparing the results of the cCTG of pregnant patients at 37-42 weeks according to the parental ethnicity (black versus white). A cCTG was performed to analyze the variables of fetal heart rate (FHR). The cCTG variables analyzed were: percentage of signal loss; number of contractions; basal FHR; number of accelerations; number of decelerations; length of high variation episodes; short-term variability (STV); total trace duration time; and number of fetal active movements. Non-stress test (NST) parameters in the two groups were compared using the Mann-Whitney test for continuous data, and the Chi-square test for categorical variables.
We found a significantly lower number of active fetal movements (p 1/4 0.007) and longer periods of low variation (p 1/4 0.047) in the cCTG of black patients when compared with white patients.
In conclusion, identifying the factors responsible for the variance in the objective analysis of CTG results is important to improve the outcomes of patients. Our study lends further evidence as to the importance of ethnicity in clinical cCTG interpretation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):609-614
To assess depression, domestic violence and the use of substances in women with recurrent miscarriages.
The Abuse Assessment Screen (AAS), the Edinburgh Postnatal Depression Scale (EPDS) and the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) were used to assess violence, depression and the use of substances among women with recurrent miscarriages. The population corresponded to patients receiv-ing prenatal care from June to August 2014. Multiple logistic regression was used to assess the multivariable relationship between depression and sociodemographic, psychosocial and medical characteristics (p < 0,10).
The prevalence of depression was of 41.3% (95% confidence interval [CI] 1/4 28.3-55.7%). One third of the pregnant women (32.6%) reported emotional or physical violence, and 13% were classified as abusing or addicted to tobacco according to ASSIST. History of psychiatric diseases was associated with depression (p 1/4 0.005). Violence during life demonstrated a modest association (p 1/4 0.073) with depression, as well as the number of miscarriages (p 1/4 0.071).
Depression is a frequent disease among pregnant women with recurrent miscarriages. The results of this investigation suggest that a systematic assessment of depression and its associated conditions, such as domestic violence and the use of substances, should be part of the prenatal follow-up visits for women with recurrent miscarriages.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(12):609-614
To assess depression, domestic violence and the use of substances in women with recurrent miscarriages.
The Abuse Assessment Screen (AAS), the Edinburgh Postnatal Depression Scale (EPDS) and the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) were used to assess violence, depression and the use of substances among women with recurrent miscarriages. The population corresponded to patients receiv-ing prenatal care from June to August 2014. Multiple logistic regression was used to assess the multivariable relationship between depression and sociodemographic, psychosocial and medical characteristics (p < 0,10).
The prevalence of depression was of 41.3% (95% confidence interval [CI] 1/4 28.3-55.7%). One third of the pregnant women (32.6%) reported emotional or physical violence, and 13% were classified as abusing or addicted to tobacco according to ASSIST. History of psychiatric diseases was associated with depression (p 1/4 0.005). Violence during life demonstrated a modest association (p 1/4 0.073) with depression, as well as the number of miscarriages (p 1/4 0.071).
Depression is a frequent disease among pregnant women with recurrent miscarriages. The results of this investigation suggest that a systematic assessment of depression and its associated conditions, such as domestic violence and the use of substances, should be part of the prenatal follow-up visits for women with recurrent miscarriages.