Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(4):297-303
To evaluate the number of patients with early-stage breast cancer who could benefit from the omission of axillary surgery following the application of the Alliance for Clinical Trials in Oncology (ACOSOG) Z0011 trial criteria.
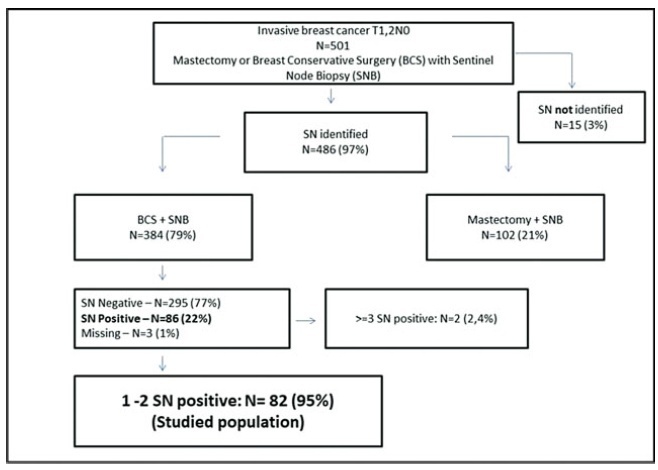
A retrospective cohort study conducted in the Hospital da Mulher da Universidade Estadual de Campinas. The study population included 384 women diagnosed with early-stage invasive breast cancer, clinically negative axilla, treated with breast-conserving surgery and sentinel lymph node biopsy, radiation therapy, chemotherapy and/or endocrine therapy, from January 2005 to December 2010. The ACOSOG Z0011 trial criteria were applied to this population and a statistical analysis was performed to make a comparison between populations.
A total of 384 patients underwent breast-conserving surgery and sentinel lymph node biopsy. Of the total number of patients, 86 women underwent axillary lymph node dissection for metastatic sentinel lymph nodes (SNLs). One patient underwent axillary node dissection due to a suspicious SLN intraoperatively, thus, she was excluded fromthe study. Among these patients, 82/86 (95.3%) had one to two involved sentinel lymph nodes andmet the criteria for the ACOSOG Z0011 trial with the omission of axillary lymph node dissection. Among the 82 eligible women, there were only 13 cases (15.9%) of lymphovascular invasion and 62 cases (75.6%) of tumors measuring up to 2 cm in diameter (T1).
The ACOSOG Z0011 trial criteria can be applied to a select group of SLNpositive patients, reducing the costs and morbidities of breast cancer surgery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(4):297-303
To evaluate the number of patients with early-stage breast cancer who could benefit from the omission of axillary surgery following the application of the Alliance for Clinical Trials in Oncology (ACOSOG) Z0011 trial criteria.
A retrospective cohort study conducted in the Hospital da Mulher da Universidade Estadual de Campinas. The study population included 384 women diagnosed with early-stage invasive breast cancer, clinically negative axilla, treated with breast-conserving surgery and sentinel lymph node biopsy, radiation therapy, chemotherapy and/or endocrine therapy, from January 2005 to December 2010. The ACOSOG Z0011 trial criteria were applied to this population and a statistical analysis was performed to make a comparison between populations.
A total of 384 patients underwent breast-conserving surgery and sentinel lymph node biopsy. Of the total number of patients, 86 women underwent axillary lymph node dissection for metastatic sentinel lymph nodes (SNLs). One patient underwent axillary node dissection due to a suspicious SLN intraoperatively, thus, she was excluded fromthe study. Among these patients, 82/86 (95.3%) had one to two involved sentinel lymph nodes andmet the criteria for the ACOSOG Z0011 trial with the omission of axillary lymph node dissection. Among the 82 eligible women, there were only 13 cases (15.9%) of lymphovascular invasion and 62 cases (75.6%) of tumors measuring up to 2 cm in diameter (T1).
The ACOSOG Z0011 trial criteria can be applied to a select group of SLNpositive patients, reducing the costs and morbidities of breast cancer surgery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(3):118-123
DOI 10.1590/S0100-72032014000300005
To assess the feasibility and diagnostic accuracy of preoperative ultrasound combined with ultrasound-guided fine-needle aspiration (US-FNA) cytology and clinical examination of axillary lymph node in patients with breast cancer.
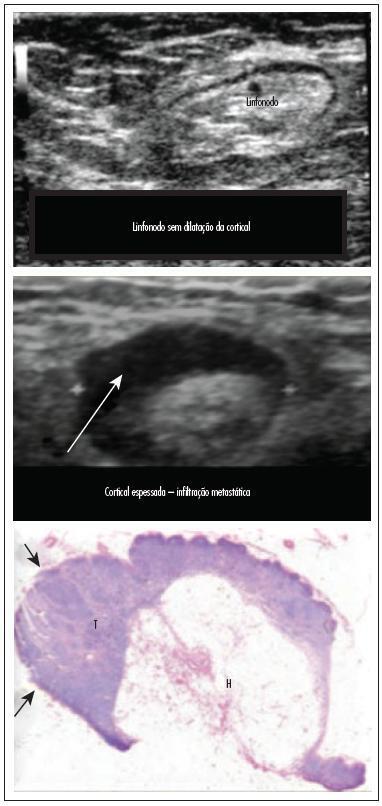
In this prospective study, 171 axillae of patients with breast cancer were evaluated by clinical examination and ultrasonography (US) with and without fine needle aspiration (FNA). Lymph nodes with maximum ultrasonographic cortical thickness > 2.3 mm were considered suspicious and submitted to US-FNA.
Logistic regression analysis showed no statistically significant correlation between clinical examination and pathologically positive axillae. However, in axillae considered suspicious by ultrasonography, the risk of positive anatomopathological findings increased 12.6-fold. Cohen's Kappa value was 0.12 for clinical examination, 0.48 for US, and 0.80 for US-FNA. Accuracy was 61.4% for clinical examination, 73.1% for US and 90.1% for US-FA. Receiver Operating Characteristics (ROC) analysis demonstrated that a cortical thickness of 2.75 mm corresponded to the highest sensitivity and specificity in predicting axillary metastasis (82.7 and 82.2%, respectively).
Ultrasonography combined with fine-needle aspiration is more accurate than clinical examination in assessing preoperative axillary status in women with breast cancer. Those who are US-FNA positive can be directed towards axillary lymph node dissection straight away, and only those who are US-FNA negative should be considered for sentinel lymph node biopsy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(3):118-123
DOI 10.1590/S0100-72032014000300005
To assess the feasibility and diagnostic accuracy of preoperative ultrasound combined with ultrasound-guided fine-needle aspiration (US-FNA) cytology and clinical examination of axillary lymph node in patients with breast cancer.
In this prospective study, 171 axillae of patients with breast cancer were evaluated by clinical examination and ultrasonography (US) with and without fine needle aspiration (FNA). Lymph nodes with maximum ultrasonographic cortical thickness > 2.3 mm were considered suspicious and submitted to US-FNA.
Logistic regression analysis showed no statistically significant correlation between clinical examination and pathologically positive axillae. However, in axillae considered suspicious by ultrasonography, the risk of positive anatomopathological findings increased 12.6-fold. Cohen's Kappa value was 0.12 for clinical examination, 0.48 for US, and 0.80 for US-FNA. Accuracy was 61.4% for clinical examination, 73.1% for US and 90.1% for US-FA. Receiver Operating Characteristics (ROC) analysis demonstrated that a cortical thickness of 2.75 mm corresponded to the highest sensitivity and specificity in predicting axillary metastasis (82.7 and 82.2%, respectively).
Ultrasonography combined with fine-needle aspiration is more accurate than clinical examination in assessing preoperative axillary status in women with breast cancer. Those who are US-FNA positive can be directed towards axillary lymph node dissection straight away, and only those who are US-FNA negative should be considered for sentinel lymph node biopsy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):483-499
DOI 10.1590/S0100-72032013001100002
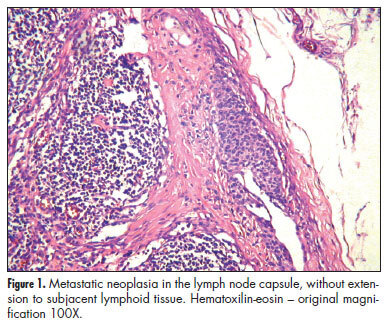
PURPOSE: To explore the relationship between morphological characteristics and histologic localization of metastasis within sentinel lymph nodes (SLN) and axillary spread in women with breast cancer. METHODS: We selected 119 patients with positive SLN submitted to complete axillary lymph node dissection from July 2002 to March 2007. We retrieved the age of patients and the primary tumor size. In the primary tumor, we evaluated histologic and nuclear grade, and peritumoral vascular invasion (PVI). In SLNs we evaluated the size of metastasis, their localization in the lymph node, number of foci, number of involved lymph nodes, and extranodal extension. RESULTS: Fifty-one (42.8%) patients had confirmed additional metastasis in non-sentinel lymph nodes (NLSN). High histologic grade, PVI, intraparenchymatous metastasis, extranodal neoplastic extension and size of metastasis were associated with positive NLSN. SLN metastasis affecting the capsule were associated to low risk incidence of additional metastasis. After multivariate analysis, PVI and metastasis size in the SLN remained as the most important risk factors for additional metastasis. CONCLUSIONS:The risk of additional involvement of NSLN is higher in patients with PVI and it increases progressively according the histologic localization in the lymph node, from capsule, where the afferent lymphatic channel arrives, to the opposite side of capsule promoting the extranodal extension. Size of metastasis greater than 6.0 mm presents higher risk of additional lymph node metastasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):483-499
DOI 10.1590/S0100-72032013001100002
PURPOSE: To explore the relationship between morphological characteristics and histologic localization of metastasis within sentinel lymph nodes (SLN) and axillary spread in women with breast cancer. METHODS: We selected 119 patients with positive SLN submitted to complete axillary lymph node dissection from July 2002 to March 2007. We retrieved the age of patients and the primary tumor size. In the primary tumor, we evaluated histologic and nuclear grade, and peritumoral vascular invasion (PVI). In SLNs we evaluated the size of metastasis, their localization in the lymph node, number of foci, number of involved lymph nodes, and extranodal extension. RESULTS: Fifty-one (42.8%) patients had confirmed additional metastasis in non-sentinel lymph nodes (NLSN). High histologic grade, PVI, intraparenchymatous metastasis, extranodal neoplastic extension and size of metastasis were associated with positive NLSN. SLN metastasis affecting the capsule were associated to low risk incidence of additional metastasis. After multivariate analysis, PVI and metastasis size in the SLN remained as the most important risk factors for additional metastasis. CONCLUSIONS:The risk of additional involvement of NSLN is higher in patients with PVI and it increases progressively according the histologic localization in the lymph node, from capsule, where the afferent lymphatic channel arrives, to the opposite side of capsule promoting the extranodal extension. Size of metastasis greater than 6.0 mm presents higher risk of additional lymph node metastasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):478-482
DOI 10.1590/S0100-72032012005000001
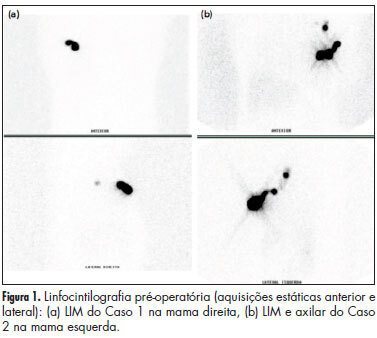
The sentinel lymph node biopsy is a standard treatment for patients with breast cancer and clinically negative axilla lymph node. The presence of an extra-axillary and intra-axillary (IM) sentinel lymph node (SLN) occurs in up to 2.6% of cases. In the presence of a metastatic IM SLN, axillary positivity may occur in up to 81% of cases. Due to the limited number of cases reported, there is no standard treatment for the association of metastatic SLN IM and non-metastatic axillary SLN . We add here two cases to the literature, one of them with metastatic disease in the axilla. The use of a nomogram demonstrated that the risk of axillary metastasis was less than 10% and the addition of these cases to the literature showed that in this situation the rate of axillary metastasis is 6.25%. We discuss the pros and cons of further axillary dissection in this situation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(10):478-482
DOI 10.1590/S0100-72032012005000001
The sentinel lymph node biopsy is a standard treatment for patients with breast cancer and clinically negative axilla lymph node. The presence of an extra-axillary and intra-axillary (IM) sentinel lymph node (SLN) occurs in up to 2.6% of cases. In the presence of a metastatic IM SLN, axillary positivity may occur in up to 81% of cases. Due to the limited number of cases reported, there is no standard treatment for the association of metastatic SLN IM and non-metastatic axillary SLN . We add here two cases to the literature, one of them with metastatic disease in the axilla. The use of a nomogram demonstrated that the risk of axillary metastasis was less than 10% and the addition of these cases to the literature showed that in this situation the rate of axillary metastasis is 6.25%. We discuss the pros and cons of further axillary dissection in this situation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):486-490
DOI 10.1590/S0100-72032010001000003
PURPOSE: to determine the efficacy of intraoperative injection of Dextran-500-99m-technetium (Tc) for the identification of the sentinel lymph node (SLN) in breast cancer and analyze time to label the SLN in the axillary region. METHODS: a prospective study between April 2008 and June 2009, which included 74 sentinel lymph node biopsies (SLNB) in patients with breast cancer in stages T1N0 and T2N0. After induction of anesthesia, 0.5 to 1.5 mCi of Dextran-500-99m-Tc filtered 0.22 µm in a volume of 5 mL was injected intraoperative using the subareolar technique for SLNB. After labeling with the radioisotope, 2 mL of patent blue was injected. The time elapsed between injection and the axillary hot spot, the in vivo and ex vivo counts of the hottest nodes, the background count, and the number of SLN identified were documented. Data were analyzed using descriptive statistics with SPSS program, version 18. RESULTS: we identified the SLN in 100% of cases. The rate of SLN identification with the probe was 98% (73/74 cases). In one case (1.35%) the SLN was labeled only with the blue dye. The mean dose of radioisotope injected was 0.97±0.22 mCi. The average time to label the SLN was 10.7 minutes (±5.7 min). We identified on average of 1.66 SLN labeled with the radioisotope. CONCLUSION: the procedure for SLN identification with an intraoperative injection of the radioisotope is oncologically safe and comfortable for the patient, providing agility to the surgical team.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):486-490
DOI 10.1590/S0100-72032010001000003
PURPOSE: to determine the efficacy of intraoperative injection of Dextran-500-99m-technetium (Tc) for the identification of the sentinel lymph node (SLN) in breast cancer and analyze time to label the SLN in the axillary region. METHODS: a prospective study between April 2008 and June 2009, which included 74 sentinel lymph node biopsies (SLNB) in patients with breast cancer in stages T1N0 and T2N0. After induction of anesthesia, 0.5 to 1.5 mCi of Dextran-500-99m-Tc filtered 0.22 µm in a volume of 5 mL was injected intraoperative using the subareolar technique for SLNB. After labeling with the radioisotope, 2 mL of patent blue was injected. The time elapsed between injection and the axillary hot spot, the in vivo and ex vivo counts of the hottest nodes, the background count, and the number of SLN identified were documented. Data were analyzed using descriptive statistics with SPSS program, version 18. RESULTS: we identified the SLN in 100% of cases. The rate of SLN identification with the probe was 98% (73/74 cases). In one case (1.35%) the SLN was labeled only with the blue dye. The mean dose of radioisotope injected was 0.97±0.22 mCi. The average time to label the SLN was 10.7 minutes (±5.7 min). We identified on average of 1.66 SLN labeled with the radioisotope. CONCLUSION: the procedure for SLN identification with an intraoperative injection of the radioisotope is oncologically safe and comfortable for the patient, providing agility to the surgical team.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(3):144-149
DOI 10.1590/S0100-72032010000300008
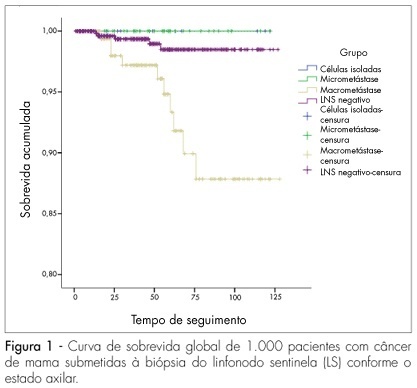
PURPOSE: to evaluate which clinical, pathological or immunohistochemical factors may be predictive of metastatic involvement of other lymph nodes in patients with breast carcinoma undergoing sentinel lymph node biopsy (SLNB). METHODS: a retrospective study carried out with 1,000 successive patients with SLNB from 1998 to 2008. Age, tumor size, histological grade, lymphovascular invasion, hormone receptor status and HER-2, size of metastasis and number of positive SLN were evaluated. The associations between the characteristics of the tumors and the types of metastases were evaluated through χ2 corrected likelihood ratio tests for insufficient samples. RESULTS: mean age was 57.6 years and mean tumor size was 1.85 cm. A total of 72.2% SLN were negative and 27.8% were positive, but in 61.9% of the cases, the SLN was the only positive one, with 78.4% having macrometastases, 17.3% micrometastases and 4.3% isolated tumor cells (CTI). Tumor size was predictive of metastases in non-sentinel lymph nodes. After 54 months of follow-up, there were no recurrences in patients with CTI, but one local recurrence and two systemic recurrences were observed in the micrometastasis group, as well as four local and 30 distant metastases in the macrometastasis group. CONCLUSIONS: among the clinical parameters studied, only tumor size was correlated with metastatic involvement in axillary lymph nodes. The size of the metastases and the number of positive SLN also directly increased the possibility of systemic recurrence. The different rates of recurrence indicate that the biological significance of these types of metastases is different and that patients with SLN metastases may also have different risks of metastatic involvement of other axillary lymph nodes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(3):144-149
DOI 10.1590/S0100-72032010000300008
PURPOSE: to evaluate which clinical, pathological or immunohistochemical factors may be predictive of metastatic involvement of other lymph nodes in patients with breast carcinoma undergoing sentinel lymph node biopsy (SLNB). METHODS: a retrospective study carried out with 1,000 successive patients with SLNB from 1998 to 2008. Age, tumor size, histological grade, lymphovascular invasion, hormone receptor status and HER-2, size of metastasis and number of positive SLN were evaluated. The associations between the characteristics of the tumors and the types of metastases were evaluated through χ2 corrected likelihood ratio tests for insufficient samples. RESULTS: mean age was 57.6 years and mean tumor size was 1.85 cm. A total of 72.2% SLN were negative and 27.8% were positive, but in 61.9% of the cases, the SLN was the only positive one, with 78.4% having macrometastases, 17.3% micrometastases and 4.3% isolated tumor cells (CTI). Tumor size was predictive of metastases in non-sentinel lymph nodes. After 54 months of follow-up, there were no recurrences in patients with CTI, but one local recurrence and two systemic recurrences were observed in the micrometastasis group, as well as four local and 30 distant metastases in the macrometastasis group. CONCLUSIONS: among the clinical parameters studied, only tumor size was correlated with metastatic involvement in axillary lymph nodes. The size of the metastases and the number of positive SLN also directly increased the possibility of systemic recurrence. The different rates of recurrence indicate that the biological significance of these types of metastases is different and that patients with SLN metastases may also have different risks of metastatic involvement of other axillary lymph nodes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(9):432-436
DOI 10.1590/S0100-72032008000900002
PURPOSE: sentinel lymph node biopsy in early-stage breast cancer patients has been substituting the total axillary lymph node is presented dissection. The technique of processing the sentinel lymph node and the aim of this study was to investigate the efficacy of occult metastasis identification based on the standard histological and immunohistochemical examination. METHODS: between 2002 and 2005, 266 sentinel lymph nodes were harvested from axillary biopsy of 170 patients with early stage breast cancer. All lymph nodes were considered to be negative according to standard intra-operative cytological assessment. Lymph nodes were transversally sectioned in four or five slices and embedded in paraffin blocks. Two paraffin-embedded tissue sections with 4 µm in thickness were mounted on glass slides and stained with hematoxylin-eosin and immunoperoxidase (cytokeratin AE1/AE3) techniques. RESULTS: standard histological examination identified metastasis in 22 patients (12.9%) and micrometastatic disease was observed in six of these patients (3.5%). The immunohistochemical examination identified metastatic disease in 16 patients (9.4%). Among them, isolated tumor cells were observed in 11 (6.5%) and micrometastases were identified in five (2.9%). CONCLUSIONS: the association of the standard histological examination and immunohistochemical technique increases the chances of sentinel lymph node metastasis identification.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(9):432-436
DOI 10.1590/S0100-72032008000900002
PURPOSE: sentinel lymph node biopsy in early-stage breast cancer patients has been substituting the total axillary lymph node is presented dissection. The technique of processing the sentinel lymph node and the aim of this study was to investigate the efficacy of occult metastasis identification based on the standard histological and immunohistochemical examination. METHODS: between 2002 and 2005, 266 sentinel lymph nodes were harvested from axillary biopsy of 170 patients with early stage breast cancer. All lymph nodes were considered to be negative according to standard intra-operative cytological assessment. Lymph nodes were transversally sectioned in four or five slices and embedded in paraffin blocks. Two paraffin-embedded tissue sections with 4 µm in thickness were mounted on glass slides and stained with hematoxylin-eosin and immunoperoxidase (cytokeratin AE1/AE3) techniques. RESULTS: standard histological examination identified metastasis in 22 patients (12.9%) and micrometastatic disease was observed in six of these patients (3.5%). The immunohistochemical examination identified metastatic disease in 16 patients (9.4%). Among them, isolated tumor cells were observed in 11 (6.5%) and micrometastases were identified in five (2.9%). CONCLUSIONS: the association of the standard histological examination and immunohistochemical technique increases the chances of sentinel lymph node metastasis identification.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(3):158-164
DOI 10.1590/S0100-72032007000300008
Axillary nodal metastasis is still the most important breast cancer prognostic factor. As in approximately 80% of the patients with tumors measuring less than 2 cm the axillary lymph nodes are negative, it has been proposed sentinel lymph node biopsy, reducing surgical morbidity in the patients with negative result. Recently, this technique has been widely used in Brazil, but there are two questions that need to be answered: what is the probability of a false-negative result (not diagnosing a positive lymph node) and if the understaging by false-negative result exposes the patient to the risk of axillary recurrence or even distant metastases, due to less effective surgical and adjuvant therapy. The literature shows that the false-negative rate varies from 5 to 10%, being the surgeon's experience the major factor that contributes to improved results. Although axillary relapse is rare, it is not yet possible to evaluate the long term effect of not removing positive lymph nodes, due to short follow-up. The recommendation is that sentinel lymph node biopsy should only be performed by surgeons with experience confirmed by a low false-negative rate.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(3):158-164
DOI 10.1590/S0100-72032007000300008
Axillary nodal metastasis is still the most important breast cancer prognostic factor. As in approximately 80% of the patients with tumors measuring less than 2 cm the axillary lymph nodes are negative, it has been proposed sentinel lymph node biopsy, reducing surgical morbidity in the patients with negative result. Recently, this technique has been widely used in Brazil, but there are two questions that need to be answered: what is the probability of a false-negative result (not diagnosing a positive lymph node) and if the understaging by false-negative result exposes the patient to the risk of axillary recurrence or even distant metastases, due to less effective surgical and adjuvant therapy. The literature shows that the false-negative rate varies from 5 to 10%, being the surgeon's experience the major factor that contributes to improved results. Although axillary relapse is rare, it is not yet possible to evaluate the long term effect of not removing positive lymph nodes, due to short follow-up. The recommendation is that sentinel lymph node biopsy should only be performed by surgeons with experience confirmed by a low false-negative rate.