. 2019;41(8):485-492
Themoment of admission for deliverymay be inappropriate for offering an intrauterine device (IUD) to women without prenatal contraception counseling. However, in countries with high cesarean rates and deficient prenatal contraception counseling, this strategy may reduce unexpected pregnancies and repeated cesarean sections.
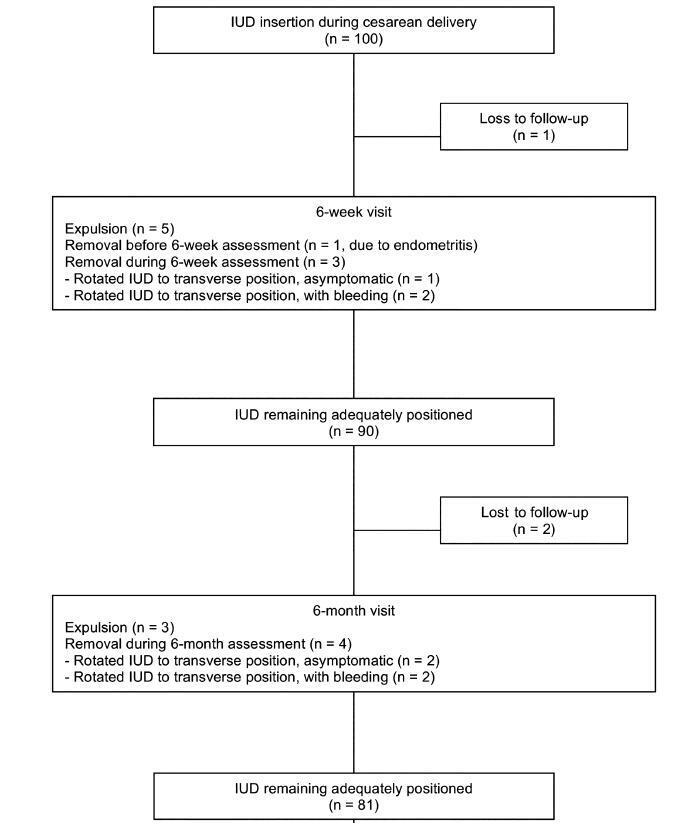
This was a prospective cohort study involving 100 women without prenatal contraception counseling. Postplacental IUD was offered after admission for delivery and placed during cesarean. The rates of IUD continuation, uterine perforation, and endometritis were assessed at 6 weeks and 6 months, and the proportion of women continuing with IUD at 6 months was assessed with respect to the number of previous cesareans.
Ninety-seven women completed the follow-up. The rate of IUD continuation was 91% at 6 weeks and 83.5% at 6 months. The expulsion/removal rate in the first 6 weeks was not different from that between 6 weeks and 6 months (9 vs 9.1%, respectively). There were 2 cases of endometritis (2.1%), and no case of uterine perforation. Among 81 women continuing with intrauterine device after 6-months, 31% had undergone only the cesarean section in which the IUD was inserted, 44% had undergone 2 and 25% had undergone 3 or more cesarean sections.
Two thirds of the women who continued with IUD at 6 months had undergone 2 ormore cesarean sections. Since offering trial of labor is unusual after 2 or more previous cesareans, we believe that offering IUD after admission for delivery may reduce the risk of repeated cesarean sections and its inherent risks.
Search
Search in:
Search
Search in:






Comments