Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
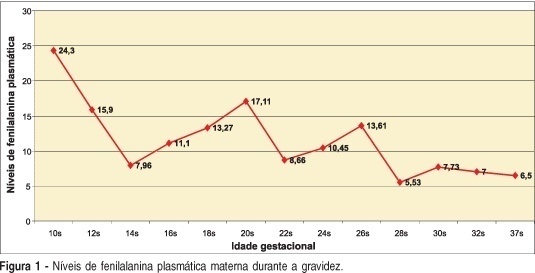
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(12):818-823
Cervical cancer (CC) is caused by persistent infection of human papillomavirus of high oncogenic risk (hr-HPV); however, several cofactors are important in its carcinogenesis, such as smoking, multiparity, and prolonged use of oral hormonal contraceptives (COCs). Worldwide, 16% of women use COCs, whereas in Brazil this rate is of ~ 30%. The safety and adverse effects of COCs are widely discussed in the literature, including the increase in carcinogenic risk. Due to the existence of several drugs, combinations, and dosages of COCs, it is hard to have uniform information in epidemiological studies. Our objective was to perform a narrative review on the role of COCs use in the carcinogenesis of cervical cancer. Several populational studies have suggested an increase in the incidence of cervical cancer for those who have used COCs for > 5 years, but other available studies reach controversial and contradictory results regarding the action of COCs in the development of CC.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(12):818-823
Cervical cancer (CC) is caused by persistent infection of human papillomavirus of high oncogenic risk (hr-HPV); however, several cofactors are important in its carcinogenesis, such as smoking, multiparity, and prolonged use of oral hormonal contraceptives (COCs). Worldwide, 16% of women use COCs, whereas in Brazil this rate is of ~ 30%. The safety and adverse effects of COCs are widely discussed in the literature, including the increase in carcinogenic risk. Due to the existence of several drugs, combinations, and dosages of COCs, it is hard to have uniform information in epidemiological studies. Our objective was to perform a narrative review on the role of COCs use in the carcinogenesis of cervical cancer. Several populational studies have suggested an increase in the incidence of cervical cancer for those who have used COCs for > 5 years, but other available studies reach controversial and contradictory results regarding the action of COCs in the development of CC.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):819-820
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):819-820
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):819-819
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):819-819
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):819-819
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(10):819-819
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):82-88
DOI 10.1590/S0100-72032009000200006
PURPOSE: to evaluate the effect of magnesium sulphate on the pulsatility index (PI) of the uterine, umbilical and fetal middle cerebral arteries, according to the persistency or not of the bilateral protodiastolic notch of the uterine arteries in severe pre-eclampsia. METHODS: a cohort study including 40 pregnant women with severe pre-eclampsia, 23 of them presenting bilateral protodiastolic notch, and 17, unilateral/absent notch. The patients were submitted to Doppler velocimetry before and 20 minutes after the intravenous administration of 6 g of magnesium sulphate. The examination was carried out with the patient in semi-Fowler position, the sonograms being obtained during fetal inactivity, in apnea and absent uterine contraction periods. All the exams were performed by two researchers, the average being considered as the final result. Wilcoxon's test was used to compare the PI, before and after magnesium sulphate in both groups. The difference between the two measurements (before and after magnesium sulphate) was compared between the groups (bilateral incision and unilateral/absent incision) using the Mann-Whitney test. RESULTS: there was a significant increase in the maternal heart rate (MHR) and decrease in the maternal blood pressure, and in the PI medians of the two uterine arteries and in the fetal middle cerebral artery, after magnesium sulphate in both groups. There was a significant decrease in the PI of the left uterine artery and in the umbilical artery, only in the protodiastolic unilateral/absent notch group. Nevertheless, it was not found any significant difference regarding the PI of the right uterine artery, or the cerebral/umbilical relationship, before and after magnesium sulphate in each group. No difference between the groups was found, before and after magnesium sulphate, for any of the studied outcomes. CONCLUSIONS: after the intravenous administration of 6 g of magnesium sulphate to patients with severe pre-eclampsia, a decrease in blood pressure and in the PI of the uterine, umbilical and fetal middle cerebral arteries occurs, besides the increase in the MHR, not influenced by the presence of bilateral protodiastolic notch in the uterine arteries.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):82-88
DOI 10.1590/S0100-72032009000200006
PURPOSE: to evaluate the effect of magnesium sulphate on the pulsatility index (PI) of the uterine, umbilical and fetal middle cerebral arteries, according to the persistency or not of the bilateral protodiastolic notch of the uterine arteries in severe pre-eclampsia. METHODS: a cohort study including 40 pregnant women with severe pre-eclampsia, 23 of them presenting bilateral protodiastolic notch, and 17, unilateral/absent notch. The patients were submitted to Doppler velocimetry before and 20 minutes after the intravenous administration of 6 g of magnesium sulphate. The examination was carried out with the patient in semi-Fowler position, the sonograms being obtained during fetal inactivity, in apnea and absent uterine contraction periods. All the exams were performed by two researchers, the average being considered as the final result. Wilcoxon's test was used to compare the PI, before and after magnesium sulphate in both groups. The difference between the two measurements (before and after magnesium sulphate) was compared between the groups (bilateral incision and unilateral/absent incision) using the Mann-Whitney test. RESULTS: there was a significant increase in the maternal heart rate (MHR) and decrease in the maternal blood pressure, and in the PI medians of the two uterine arteries and in the fetal middle cerebral artery, after magnesium sulphate in both groups. There was a significant decrease in the PI of the left uterine artery and in the umbilical artery, only in the protodiastolic unilateral/absent notch group. Nevertheless, it was not found any significant difference regarding the PI of the right uterine artery, or the cerebral/umbilical relationship, before and after magnesium sulphate in each group. No difference between the groups was found, before and after magnesium sulphate, for any of the studied outcomes. CONCLUSIONS: after the intravenous administration of 6 g of magnesium sulphate to patients with severe pre-eclampsia, a decrease in blood pressure and in the PI of the uterine, umbilical and fetal middle cerebral arteries occurs, besides the increase in the MHR, not influenced by the presence of bilateral protodiastolic notch in the uterine arteries.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(2):82-87
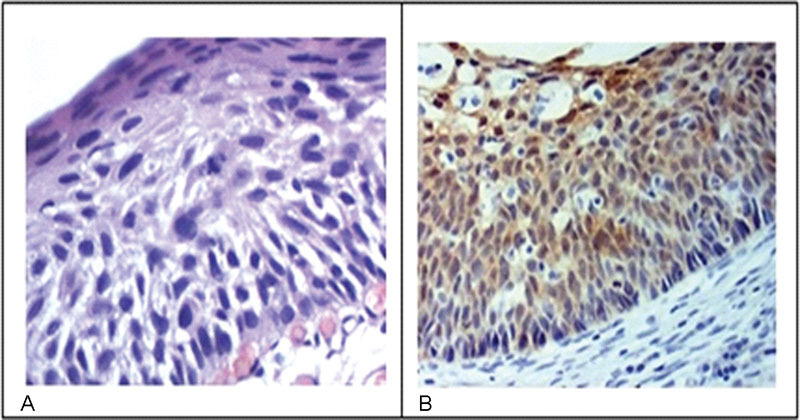
The aim of this study was to determine the expression of the immunohistochemical markers p16 and Ki-67 in cervical intraepithelial neoplasms and their influence on the level of agreement among different observers and for the same observer.
The study included 184 patients with cervical intraepithelial neoplasms previously confirmed through biopsies performed between 2005 and 2006. Three pathologists reviewed the biopsies by using hematoxylin-eosin staining to reach a consensus on the diagnosis. Subsequently, an immunohistochemical study analyzed the expression of p16 and Ki-67 in such cases.
The comparison among the reviewing pathologists revealed only moderate agreement (kappa = 0.44). The agreement improved when the differentiation of highgrade lesions (cervical intraepithelial neoplasm - CIN - 3) was analyzed (kappa = 0.59). p16 staining exhibited a high negative predictive value and sensitivity; however, the specificity was low. Overall, both qualitative and quantitative analyses of p16 and a quantitative analysis Ki-67 exhibited low accuracy. The agreement among diagnoses before immunohistochemistry was 0.47. The use of immunohistochemistry increased the agreement to 0.68.
Our study showed that the agreement among observers using traditional diagnostic criteria of cervical intraepithelial lesions can improve with the use of immunohistochemistry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(2):82-87
The aim of this study was to determine the expression of the immunohistochemical markers p16 and Ki-67 in cervical intraepithelial neoplasms and their influence on the level of agreement among different observers and for the same observer.
The study included 184 patients with cervical intraepithelial neoplasms previously confirmed through biopsies performed between 2005 and 2006. Three pathologists reviewed the biopsies by using hematoxylin-eosin staining to reach a consensus on the diagnosis. Subsequently, an immunohistochemical study analyzed the expression of p16 and Ki-67 in such cases.
The comparison among the reviewing pathologists revealed only moderate agreement (kappa = 0.44). The agreement improved when the differentiation of highgrade lesions (cervical intraepithelial neoplasm - CIN - 3) was analyzed (kappa = 0.59). p16 staining exhibited a high negative predictive value and sensitivity; however, the specificity was low. Overall, both qualitative and quantitative analyses of p16 and a quantitative analysis Ki-67 exhibited low accuracy. The agreement among diagnoses before immunohistochemistry was 0.47. The use of immunohistochemistry increased the agreement to 0.68.
Our study showed that the agreement among observers using traditional diagnostic criteria of cervical intraepithelial lesions can improve with the use of immunohistochemistry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(2):82-86
DOI 10.1590/SO100-720320140005040
To analyze the risk factors for urinary incontinence (UI) in older women practicing physical exercises (PE).
A total of 152 older women with a mean age of 68.6±5.8 years who regularly practiced PE participated in the study. The presence of UI and gynecological, obstetric, clinical, behavioral, hereditary and anthropometric risk factors was determined identified. It was also applied the Domain 4 of the International Physical Activity Questionnaire (IPAQ) to determine the level of physical activity and body mass index and waist circumference were measured. Data were analyzed using descriptive and inferential statistics, with the level of significance set at 5%.
The prevalence of UI in the sample was 32.2%. Among the factors evaluated, only the use of diuretics (OR=2.7; 95%CI 1.0-7.0) and a positive family history of urinary incontinence (OR=2.3; 95%CI 1.1-4.8) were associated with UI symptoms.
The use of diuretics is considered to be a modifiable risk factor for UI, whereas a family history is not considered to be a modifiable risk factor.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(2):82-86
DOI 10.1590/SO100-720320140005040
To analyze the risk factors for urinary incontinence (UI) in older women practicing physical exercises (PE).
A total of 152 older women with a mean age of 68.6±5.8 years who regularly practiced PE participated in the study. The presence of UI and gynecological, obstetric, clinical, behavioral, hereditary and anthropometric risk factors was determined identified. It was also applied the Domain 4 of the International Physical Activity Questionnaire (IPAQ) to determine the level of physical activity and body mass index and waist circumference were measured. Data were analyzed using descriptive and inferential statistics, with the level of significance set at 5%.
The prevalence of UI in the sample was 32.2%. Among the factors evaluated, only the use of diuretics (OR=2.7; 95%CI 1.0-7.0) and a positive family history of urinary incontinence (OR=2.3; 95%CI 1.1-4.8) were associated with UI symptoms.
The use of diuretics is considered to be a modifiable risk factor for UI, whereas a family history is not considered to be a modifiable risk factor.