Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(7):640-645
The present study seeks to identify the associated factors that increased primary cesarean delivery rates.
This was a cross-sectional study that evaluated the number of primary cesarean sections performed in the years 2006 and 2018 at the Hospital de Clínicas de Porto Alegre (HCPA, in the Portuguese acronym), through the collection of data from the medical records of the patients.
Advanced maternal age, twin pregnancy, and higher body mass index (BMI) became more frequent in 2018 in comparison with 2006. To mitigate the impact of confounding in comparisons among groups, we made an adjustment by propensity scores and detected significant differences when comparing both age groups on twin pregnancy rates, gestational diabetes mellitus, and thyroid disease.
Data from the present study can be used to prevent and improve the management of morbidities, impacting on better outcomes in obstetrical practice.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(7):640-645
The present study seeks to identify the associated factors that increased primary cesarean delivery rates.
This was a cross-sectional study that evaluated the number of primary cesarean sections performed in the years 2006 and 2018 at the Hospital de Clínicas de Porto Alegre (HCPA, in the Portuguese acronym), through the collection of data from the medical records of the patients.
Advanced maternal age, twin pregnancy, and higher body mass index (BMI) became more frequent in 2018 in comparison with 2006. To mitigate the impact of confounding in comparisons among groups, we made an adjustment by propensity scores and detected significant differences when comparing both age groups on twin pregnancy rates, gestational diabetes mellitus, and thyroid disease.
Data from the present study can be used to prevent and improve the management of morbidities, impacting on better outcomes in obstetrical practice.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):640-644
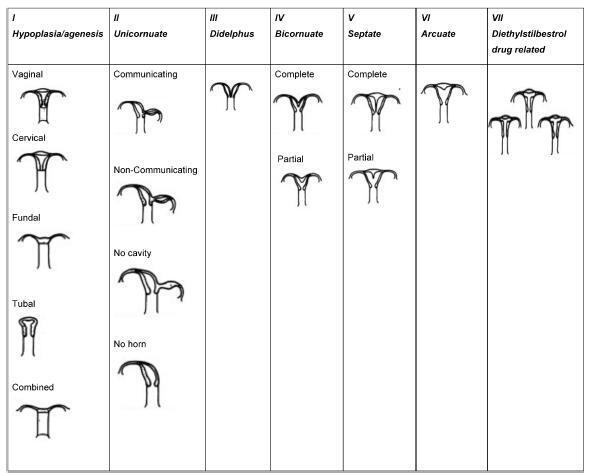
Approximately 1 in every 76,000 pregnancies develops within a unicornuate uterus with a rudimentary horn.Müllerian uterus anomalies are often asymptomatic, thus, the diagnosis is a challenge, and it is usually made during the gestation or due to its complications, such as uterine rupture, pregnancy-induced hypertension, antepartum, postpartum bleeding and intrauterine growth restriction (IUGR). In order to avoid unnecessary cesarean sections and the risks they involve, the physicians should consider the several approaches and for how long it is feasible to perform labor induction in suspected cases of pregnancy in a unicornuate uterus with a rudimentary horn, despite the rarity of the anomaly. This report describes a case of a unicornuate uterus in which a pregnancy developed in the non-communicating rudimentary horn and the consequences of the delayed diagnosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):640-644
Approximately 1 in every 76,000 pregnancies develops within a unicornuate uterus with a rudimentary horn.Müllerian uterus anomalies are often asymptomatic, thus, the diagnosis is a challenge, and it is usually made during the gestation or due to its complications, such as uterine rupture, pregnancy-induced hypertension, antepartum, postpartum bleeding and intrauterine growth restriction (IUGR). In order to avoid unnecessary cesarean sections and the risks they involve, the physicians should consider the several approaches and for how long it is feasible to perform labor induction in suspected cases of pregnancy in a unicornuate uterus with a rudimentary horn, despite the rarity of the anomaly. This report describes a case of a unicornuate uterus in which a pregnancy developed in the non-communicating rudimentary horn and the consequences of the delayed diagnosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(10):641-646
DOI 10.1590/S0100-72032002001000002
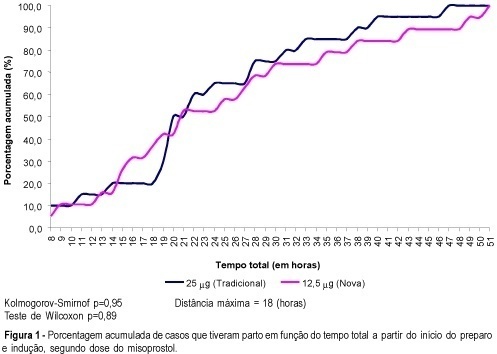
PURPOSE: to compare the effectiveness and safety of two different doses of misoprostol (12.5 mug and 25 mug) administered vaginally for cervical ripening and labor induction in term pregnancies with an indication for interruption. METHODS: this was a pilot randomized controlled single blinded trial, including 40 pregnant women treated with one of the two different doses of misoprostol. The independent variable was the dose of misoprostol and the main dependent variables were the mode of delivery, time between induction and delivery, perinatal complications and maternal side effects. The main control variables were maternal age, gestational age, literacy, parity, skin color and conditions of the cervix at the beginning of induction. For data analysis Student's t test, chi2, exact Fisher, Wilcoxon and Kolmogorov-Smirnof tests were used, besides survival analysis. RESULTS: the groups using 12.5 and 25 mug were similar and did not present any significant difference regarding time for onset of uterine contractions (20.9±20.4 and 16.6±9.8 h, respectively), time between onset of uterine contractions and delivery (7.8±3.4 and 6.9±5.0 h), vaginal delivery (65 and 80%) and maternal and perinatal side effects (similar Apgar scores and hyperstimulation syndrome in both groups). CONCLUSION: the higher percentage of vaginal births and the shorter time for delivery using 25 mug, although not significant, does not allow to recommend the dose of 12.5 mug as more advantageous for cervical ripening and labor induction in term pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(10):641-646
DOI 10.1590/S0100-72032002001000002
PURPOSE: to compare the effectiveness and safety of two different doses of misoprostol (12.5 mug and 25 mug) administered vaginally for cervical ripening and labor induction in term pregnancies with an indication for interruption. METHODS: this was a pilot randomized controlled single blinded trial, including 40 pregnant women treated with one of the two different doses of misoprostol. The independent variable was the dose of misoprostol and the main dependent variables were the mode of delivery, time between induction and delivery, perinatal complications and maternal side effects. The main control variables were maternal age, gestational age, literacy, parity, skin color and conditions of the cervix at the beginning of induction. For data analysis Student's t test, chi2, exact Fisher, Wilcoxon and Kolmogorov-Smirnof tests were used, besides survival analysis. RESULTS: the groups using 12.5 and 25 mug were similar and did not present any significant difference regarding time for onset of uterine contractions (20.9±20.4 and 16.6±9.8 h, respectively), time between onset of uterine contractions and delivery (7.8±3.4 and 6.9±5.0 h), vaginal delivery (65 and 80%) and maternal and perinatal side effects (similar Apgar scores and hyperstimulation syndrome in both groups). CONCLUSION: the higher percentage of vaginal births and the shorter time for delivery using 25 mug, although not significant, does not allow to recommend the dose of 12.5 mug as more advantageous for cervical ripening and labor induction in term pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(8):641-647
DOI 10.1590/S0100-72032004000800008
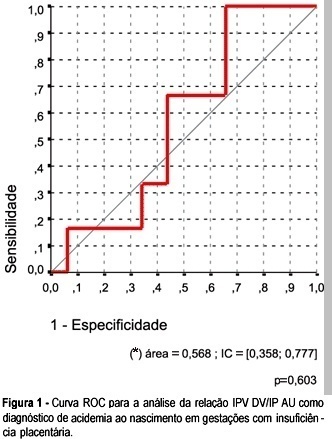
OBJECTIVE: to investigate whether it is possible to predict acidemia at birth in pregnancies with placental insufficiency using venous-arterial indices: pulsatility index for vein (PIV) of the ductus venosus (DV) over PI of the middle cerebral artery (MCA) and PIV of the DV over PI of the umbilical artery, and establish cut-off values for this prediction. PATIENTS AND METHODS: this was a prospective cross-sectional study involving forty-seven patients with placental insufficiency (umbilical artery resistance and pulsatility indices above the 95th percentile for gestational age) who were submitted to Dopplervelocimetry in the last 24 hours before delivery. All pregnancies were singleton, over 26 weeks of age and without structural or chromosome anomalies. Arterial cord blood was obtained for gasometry immediately after birth. Acidemia was defined as umbilical arterial pH < 7.20 in the absence of uterine contractions and pH < 7.15 in the presence of contractions. Metabolic or mixed acidemia at birth were considered pathological. A ROC curve was calculated for the venous-arterial indices: PIV DV/PI umbilical artery (UA) and PIV DV/PI MCA. A cut-off value was established and sensitivity, specificity, accuracy, positive and negative predictive values and positive and negative likelihood ratios were calculated. RESULTS: The DV/UA PI index was not a good predictor of acidemia at birth. The DV/MCA PI index was related to acidemia at birth (area under the curve 0,785, p = 0,004). The cut-off value was: 0,582, sensitivity 66,7%, specificity 77,1 and accuracy 74,5%. CONCLUSION: the PIV DV/PI MCA ratio is adequate for predicting acidemia at birth in pregnancies with placental insufficiency. The cut-off value was: 0,582.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(8):641-647
DOI 10.1590/S0100-72032004000800008
OBJECTIVE: to investigate whether it is possible to predict acidemia at birth in pregnancies with placental insufficiency using venous-arterial indices: pulsatility index for vein (PIV) of the ductus venosus (DV) over PI of the middle cerebral artery (MCA) and PIV of the DV over PI of the umbilical artery, and establish cut-off values for this prediction. PATIENTS AND METHODS: this was a prospective cross-sectional study involving forty-seven patients with placental insufficiency (umbilical artery resistance and pulsatility indices above the 95th percentile for gestational age) who were submitted to Dopplervelocimetry in the last 24 hours before delivery. All pregnancies were singleton, over 26 weeks of age and without structural or chromosome anomalies. Arterial cord blood was obtained for gasometry immediately after birth. Acidemia was defined as umbilical arterial pH < 7.20 in the absence of uterine contractions and pH < 7.15 in the presence of contractions. Metabolic or mixed acidemia at birth were considered pathological. A ROC curve was calculated for the venous-arterial indices: PIV DV/PI umbilical artery (UA) and PIV DV/PI MCA. A cut-off value was established and sensitivity, specificity, accuracy, positive and negative predictive values and positive and negative likelihood ratios were calculated. RESULTS: The DV/UA PI index was not a good predictor of acidemia at birth. The DV/MCA PI index was related to acidemia at birth (area under the curve 0,785, p = 0,004). The cut-off value was: 0,582, sensitivity 66,7%, specificity 77,1 and accuracy 74,5%. CONCLUSION: the PIV DV/PI MCA ratio is adequate for predicting acidemia at birth in pregnancies with placental insufficiency. The cut-off value was: 0,582.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(10):641-646
DOI 10.1590/S0100-72032000001000007
Purpose: to evaluate the influence of cigarette smoking on uteroplacental, fetoplacental and fetal blood flow by obstetric Doppler velocimetry of the uterine, umbilical and middle cerebral arteries. Method: a prospective study with 42 healthy pregnant women, 20 of whom were smokers and 24 nonsmokers. Ultrasound was performed initially to determine the gestation time. The pregnant women next underwent pulsed and color Doppler velocimetry of the uterine, umbilical and middle cerebral arteries at the 24th, 28th, 32nd, 36th, and 40th week. The smokers were instructed not to smoke for at least two hours before the test. Results: the mean resistance index (RI) of the right and left uterine arteries was greatest in the smoking group at the 36th week [mean (SD) = 0.501 (0.034)], (p = 0.002). The pulsatility index (PI) of the umbilical artery was greatest in the smoking group at the 28th week [mean (SD) = 1.135 (0.182)], (p = 0.008). No difference in the PI of the middle cerebral artery (MCA) was detected between the two groups. However, the MCA/umbilical PI ratio was lower in the smoking group at the 32nd [mean (SD) = 1.977 (0.291)], (p = 0.027), and 36th week [mean (SD) = 1.850 (0.465)], (p = 0.014). Conclusion: it was concluded that smoking increases resistance in the uteroplacental and fetoplacental circulation while simultaneously reducing resistance in the MCA, imitating a "brain-sparing" effect, most likely due to chronic hypoxia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(10):641-646
DOI 10.1590/S0100-72032000001000007
Purpose: to evaluate the influence of cigarette smoking on uteroplacental, fetoplacental and fetal blood flow by obstetric Doppler velocimetry of the uterine, umbilical and middle cerebral arteries. Method: a prospective study with 42 healthy pregnant women, 20 of whom were smokers and 24 nonsmokers. Ultrasound was performed initially to determine the gestation time. The pregnant women next underwent pulsed and color Doppler velocimetry of the uterine, umbilical and middle cerebral arteries at the 24th, 28th, 32nd, 36th, and 40th week. The smokers were instructed not to smoke for at least two hours before the test. Results: the mean resistance index (RI) of the right and left uterine arteries was greatest in the smoking group at the 36th week [mean (SD) = 0.501 (0.034)], (p = 0.002). The pulsatility index (PI) of the umbilical artery was greatest in the smoking group at the 28th week [mean (SD) = 1.135 (0.182)], (p = 0.008). No difference in the PI of the middle cerebral artery (MCA) was detected between the two groups. However, the MCA/umbilical PI ratio was lower in the smoking group at the 32nd [mean (SD) = 1.977 (0.291)], (p = 0.027), and 36th week [mean (SD) = 1.850 (0.465)], (p = 0.014). Conclusion: it was concluded that smoking increases resistance in the uteroplacental and fetoplacental circulation while simultaneously reducing resistance in the MCA, imitating a "brain-sparing" effect, most likely due to chronic hypoxia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):641-646
DOI 10.1590/S0100-72032001001000005
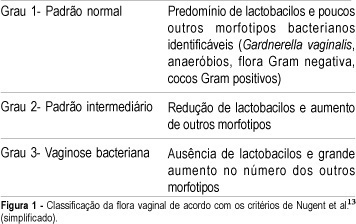
Purpose: to evaluate the prevalence of bacterial vaginosis (BV) in menopausal and in infertile outpatients and to analyze the current clinical diagnostic methods. Methods: we evaluated retrospectively 104 menopausal women and 86 with infertility. Characteristic vaginal discharge on gynecological examination, pH >4.5, positive KOH whiff test, and bacterial vaginosis by Gram test were considered positive. BV was established when at least 3 out of 4 criteria were found. Results: among the menopausal women, 29 patients (28.1%) were clinically positive for BV, 10 (9.6%) had positive whiff test, 68 (65.4%) vaginal pH >4.5, and 34 (32.7%) positive Gram test. For the infertile patients the figures were 20 (23.2%), 13 (15.1%), 61 (70.9%) and 26 (30.2%), respectively. According to our established criteria, BV was diagnosed in 14 menopausal (13.5%) and 15 infertile (17.4%) women. Conclusion: bacterial vaginosis prevalence was similar in both groups of patients. In addition, all diagnostic criteria should be followed in order to avoid underdiagnosing this pathology or treating an otherwise normal vaginal flora.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):641-646
DOI 10.1590/S0100-72032001001000005
Purpose: to evaluate the prevalence of bacterial vaginosis (BV) in menopausal and in infertile outpatients and to analyze the current clinical diagnostic methods. Methods: we evaluated retrospectively 104 menopausal women and 86 with infertility. Characteristic vaginal discharge on gynecological examination, pH >4.5, positive KOH whiff test, and bacterial vaginosis by Gram test were considered positive. BV was established when at least 3 out of 4 criteria were found. Results: among the menopausal women, 29 patients (28.1%) were clinically positive for BV, 10 (9.6%) had positive whiff test, 68 (65.4%) vaginal pH >4.5, and 34 (32.7%) positive Gram test. For the infertile patients the figures were 20 (23.2%), 13 (15.1%), 61 (70.9%) and 26 (30.2%), respectively. According to our established criteria, BV was diagnosed in 14 menopausal (13.5%) and 15 infertile (17.4%) women. Conclusion: bacterial vaginosis prevalence was similar in both groups of patients. In addition, all diagnostic criteria should be followed in order to avoid underdiagnosing this pathology or treating an otherwise normal vaginal flora.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(11):642-649
DOI 10.1590/S0100-72032005001100002
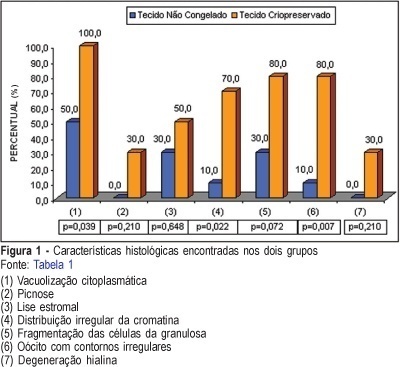
PURPOSE: to evaluate follicular preservation and histologic characteristics of the cryopreserved ovarian tissue and to compare with the fresh one, in rabbits. METHODS: ten adult female white rabbits were submitted to right oophorectomy. The dried ovary was dissected and the cortex was maintained with approximately 1.5 millimeter thickness. The tissue was fractionated into small sections, some reserved for control histologic study and others destined for cryopreservation. Six weeks later the ovarian tissue was thawed and evaluated histologically. After histologic processing, the control and the experimental samples were stained with hematoxylin and eosin and treated immunohistochemically by the PCNA technique for evaluation of DNA preservation. Histologic alterations present in the fresh and in the cryopreserved tissues were identified, and cryopreserved tissue viability was evaluated. RESULTS: in the cryopreserved tissue only primordial follicles persisted. Reversible alterations were identified: cytoplasmatic vacuolation (p=0,039), stromal lysis (p=0.648) and oocytes with irregular contours (p=0.007). Irreversible alterations: (hyalin degeneration and pyknosis) were found, but not at significant levels (p=0.210). The immunohistochemical analysis showed PCNA staining of follicles at different stages of development in the fresh tissue and primordial follicles in the cryopreserved tissue, indicating the presence of active DNA in both tissues. CONCLUSION: in the cryopreserved ovarian tissue the following were observed: survival of only primordial follicles; significant reversible histologic alterations (cytoplasmic vacuolation, stromal lysis and oocytes with irregular contours); irreversible alterations (hyalin degeneration and pyknosis), and PCNA staining of all follicles.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(11):642-649
DOI 10.1590/S0100-72032005001100002
PURPOSE: to evaluate follicular preservation and histologic characteristics of the cryopreserved ovarian tissue and to compare with the fresh one, in rabbits. METHODS: ten adult female white rabbits were submitted to right oophorectomy. The dried ovary was dissected and the cortex was maintained with approximately 1.5 millimeter thickness. The tissue was fractionated into small sections, some reserved for control histologic study and others destined for cryopreservation. Six weeks later the ovarian tissue was thawed and evaluated histologically. After histologic processing, the control and the experimental samples were stained with hematoxylin and eosin and treated immunohistochemically by the PCNA technique for evaluation of DNA preservation. Histologic alterations present in the fresh and in the cryopreserved tissues were identified, and cryopreserved tissue viability was evaluated. RESULTS: in the cryopreserved tissue only primordial follicles persisted. Reversible alterations were identified: cytoplasmatic vacuolation (p=0,039), stromal lysis (p=0.648) and oocytes with irregular contours (p=0.007). Irreversible alterations: (hyalin degeneration and pyknosis) were found, but not at significant levels (p=0.210). The immunohistochemical analysis showed PCNA staining of follicles at different stages of development in the fresh tissue and primordial follicles in the cryopreserved tissue, indicating the presence of active DNA in both tissues. CONCLUSION: in the cryopreserved ovarian tissue the following were observed: survival of only primordial follicles; significant reversible histologic alterations (cytoplasmic vacuolation, stromal lysis and oocytes with irregular contours); irreversible alterations (hyalin degeneration and pyknosis), and PCNA staining of all follicles.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(10):642-648
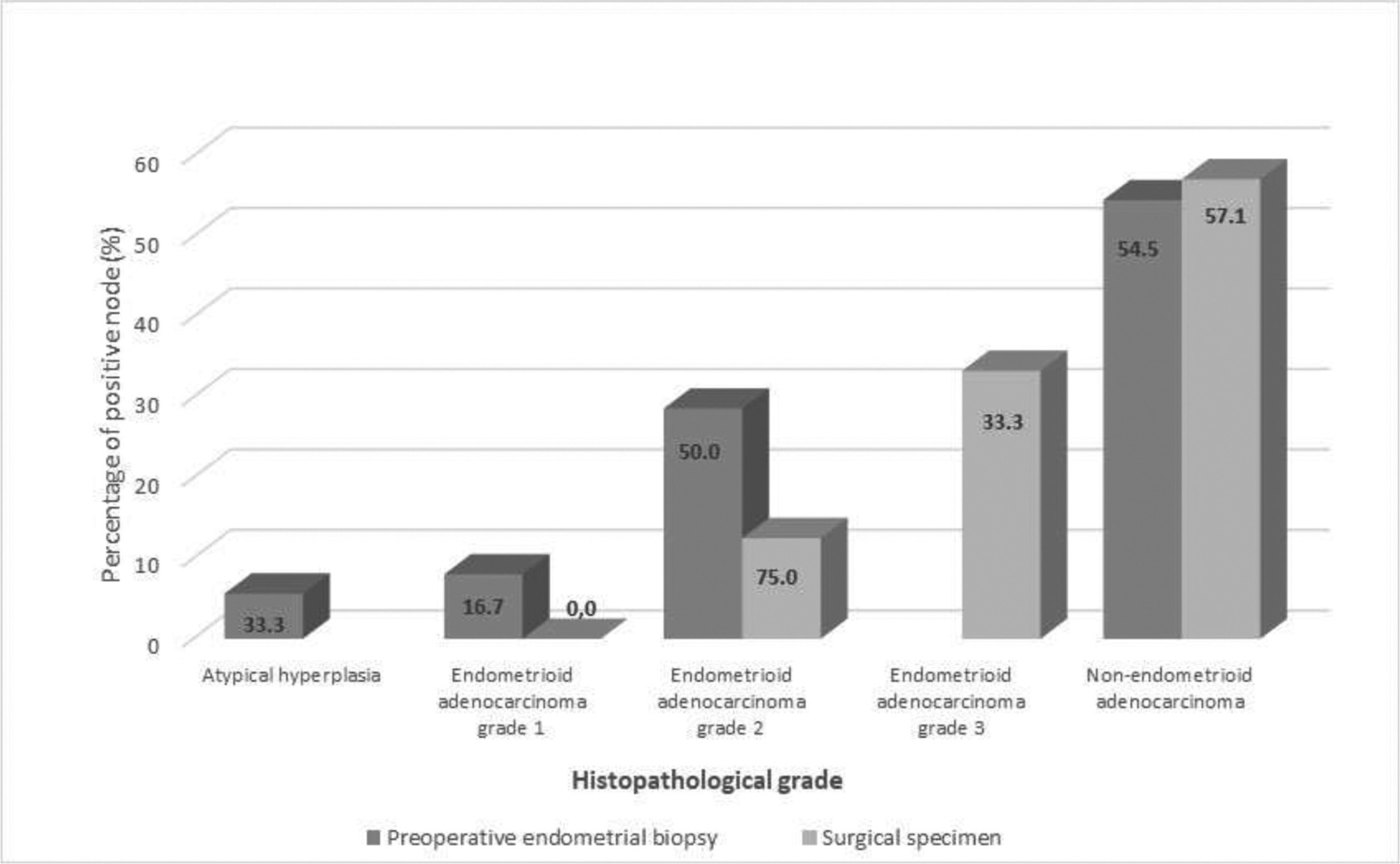
To evaluate the agreement between the histopathological diagnoses of preoperative endometrial samples and surgical specimens and correlate the agreement between the diagnoses with the impact on surgical management and the survival of patients with endometrial adenocarcinomas.
Sixty-two patients treated for endometrial cancer at a university hospital from 2002 to 2011 were retrospectively evaluated. The histopathological findings of preoperative endometrial samples and of surgical specimens were analyzed. The patients were subjected to hysterectomy as well as adjuvant treatment, if necessary, and clinical follow-up, according to the institutional protocol. Lesions were classified as endometrioid tumor (type 1) grades 1, 2, or 3 or non-endometrioid carcinoma (type 2).
The agreement between the histopathological diagnoses based on preoperative endometrial samples and surgical specimens was fair (Kappa: 0.40; p < 0.001). However, the agreement was very significant for tumor type and grade, in which a higher concordance occurred at a higher grade. The percentage of patients with lymph nodes affected was 19.2%;. Although most patients presenting with disease remission or cure were in the early stages (90.5%;), there were no significant differences between those patients who had a misdiagnosis (11/16; 68.8%;) and those who had a correct diagnosis (25/33; 75.8%;) based on preoperative endometrial sampling (p = 0.605).
Our findings corroborate the literature and confirm the under staging of preoperative endometrial samples based on histopathological assessment, especially for lower grade endometrial tumors. We suggest that the preoperative diagnosis should be complemented with other methods to better plan the surgical management strategy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(10):642-648
To evaluate the agreement between the histopathological diagnoses of preoperative endometrial samples and surgical specimens and correlate the agreement between the diagnoses with the impact on surgical management and the survival of patients with endometrial adenocarcinomas.
Sixty-two patients treated for endometrial cancer at a university hospital from 2002 to 2011 were retrospectively evaluated. The histopathological findings of preoperative endometrial samples and of surgical specimens were analyzed. The patients were subjected to hysterectomy as well as adjuvant treatment, if necessary, and clinical follow-up, according to the institutional protocol. Lesions were classified as endometrioid tumor (type 1) grades 1, 2, or 3 or non-endometrioid carcinoma (type 2).
The agreement between the histopathological diagnoses based on preoperative endometrial samples and surgical specimens was fair (Kappa: 0.40; p < 0.001). However, the agreement was very significant for tumor type and grade, in which a higher concordance occurred at a higher grade. The percentage of patients with lymph nodes affected was 19.2%;. Although most patients presenting with disease remission or cure were in the early stages (90.5%;), there were no significant differences between those patients who had a misdiagnosis (11/16; 68.8%;) and those who had a correct diagnosis (25/33; 75.8%;) based on preoperative endometrial sampling (p = 0.605).
Our findings corroborate the literature and confirm the under staging of preoperative endometrial samples based on histopathological assessment, especially for lower grade endometrial tumors. We suggest that the preoperative diagnosis should be complemented with other methods to better plan the surgical management strategy.