Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1011-1013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1011-1013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1014-1020
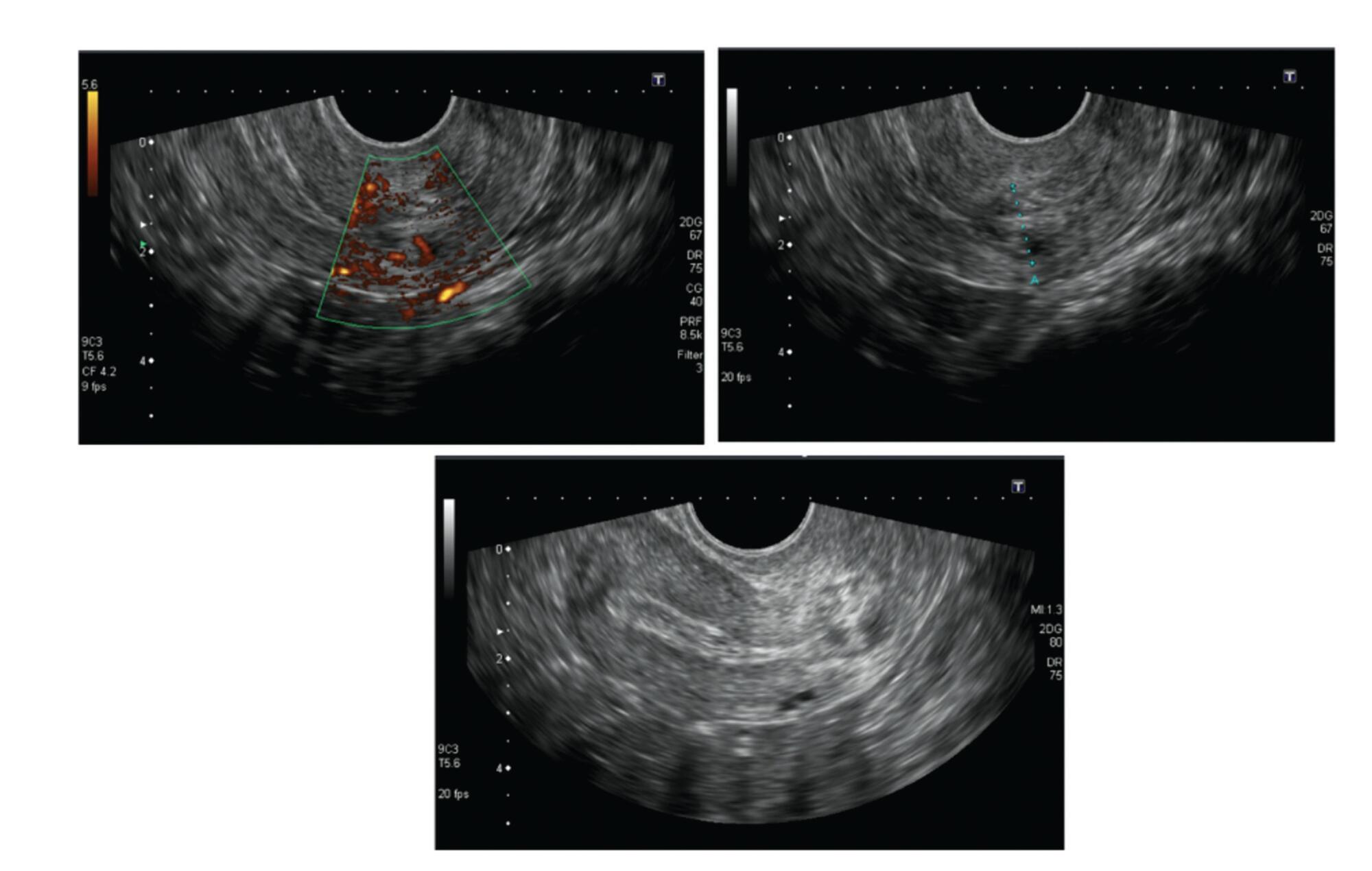
Cervical pregnancy is challenging for the medical community, as it is potentially fatal. The treatment can be medical or surgical; however, there are no protocols that establish the best option for each case. The objective of the present study was to describe the cases of cervical pregnancy admitted to a tertiary university hospital over a period of 18 years.
A retrospective study based on a review of the medical records of all cervical pregnancies admitted to the Women's Hospital at Universidade Estadual de Campinas, Southeastern Brazil, from 2000 to 2018.
We identified 13 cases of cervical pregnancy out of a total of 673 ectopic pregnancies; only 1 case was initially treated with surgery because of hemodynamic instability. Of the 12 cases treated conservatively, 7 were treated with single-dose intramuscular methotrexate, 1, with intravenous and intramuscular methotrexate, 1, with intravenous methotrexate, 1, with 2 doses of intramuscular methotrexate, and 2, with intra-amniotic methotrexate. Of these cases, one had a therapeutic failure that required a hysterectomy. Two women received blood transfusions. Four women required cervical tamponade with a Foley catheter balloon for hemostasis. There was no fatal outcome.
Cervical pregnancy is a rare and challenging condition from diagnosis to treatment. Conservative treatment was the primary method of therapy used, with satisfactory results. In cases of increased bleeding, cervical curettage was the initial treatment, and it was associated with the use of a cervical balloon for hemostasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1014-1020
Cervical pregnancy is challenging for the medical community, as it is potentially fatal. The treatment can be medical or surgical; however, there are no protocols that establish the best option for each case. The objective of the present study was to describe the cases of cervical pregnancy admitted to a tertiary university hospital over a period of 18 years.
A retrospective study based on a review of the medical records of all cervical pregnancies admitted to the Women's Hospital at Universidade Estadual de Campinas, Southeastern Brazil, from 2000 to 2018.
We identified 13 cases of cervical pregnancy out of a total of 673 ectopic pregnancies; only 1 case was initially treated with surgery because of hemodynamic instability. Of the 12 cases treated conservatively, 7 were treated with single-dose intramuscular methotrexate, 1, with intravenous and intramuscular methotrexate, 1, with intravenous methotrexate, 1, with 2 doses of intramuscular methotrexate, and 2, with intra-amniotic methotrexate. Of these cases, one had a therapeutic failure that required a hysterectomy. Two women received blood transfusions. Four women required cervical tamponade with a Foley catheter balloon for hemostasis. There was no fatal outcome.
Cervical pregnancy is a rare and challenging condition from diagnosis to treatment. Conservative treatment was the primary method of therapy used, with satisfactory results. In cases of increased bleeding, cervical curettage was the initial treatment, and it was associated with the use of a cervical balloon for hemostasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):102-106
DOI 10.1590/S0100-72032012000300002
PURPOSE: To assess the prevalence of obstetric risk factors and their association with unfavorable outcomes for the mother and fetus. METHODS: A longitudinal, descriptive and analytical study was conducted on 204 pregnant women between May 2007 and December 2008. Clinical and laboratory assessments followed routine protocols. Risk factors included socio-demographic aspects; family, personal and obstetric history; high pre-gestational body mass index (BMI); excessive gestational weight gain and anemia. Adverse outcomes included pre-eclampsia (4.5%), gestational diabetes mellitus (3.4%), premature birth (4.4%), caesarian birth (40.1%), high birth weight (9.8%) and low birth weight (13.8%). RESULTS: The average age was 26±6.4 years; the mothers were predominantly non-white (84.8%), 51.8% had incomplete or complete secondary level schooling, 67.2% were in a stable marital relationship and 51.0% had a regular paid job; 63.7% were admitted to the prenatal clinic during the second trimester and 16.7% during the first, with 42.6% being primiparous. A past history of chronic hypertension was reported by 2.9%, pre-eclampsia by 9.8%, excessive gestational weight gain by 15.2% and former gestational diabetes mellitus by 1.0%. In the current pregnancy, elevated pre-gestational BMI was found in 34.6%; 45.5% presented with excessive gestational weight gain, 25.3% with anemia and 47.3% with dyslipidemia. Of the 17.5% of cases with altered blood glucose, gestational diabetes mellitus was confirmed in 3.4% and proteinuria occurred in 16.4% of all cases. Adverse maternal fetal outcomes included pre-eclampsia (4.5%), gestational diabetes mellitus (3.4%), premature birth (4.4%), caesarean birth (40.1%) and high and low birth weight (9.8% and 13.8%, respectively). Independent predictors of adverse maternal fetal outcomes were identified by Poisson multivariate regression analysis: pre-gestational BMI>25 kg/m² was a predictor for pre-eclampsia (RR=17.17; 95%CI 2.14-137.46) and caesarian operation (RR=1.79; 95%CI 1.13-2.85), previous caesarean was a predictor for present caesarean operation (RR=2.28; 95%CI 1.32-3.92) and anemia and high gestational weight gain were predictors for high birth weight (RR=3.38; 95%CI 1.41-8.14 and RR=4.68; 95%CI 1.56-14.01, respectively). CONCLUSION: Pre-gestational overweight/obesity, previous caesarean, excessive weight gain and anemia were major risk factors for pre-eclampsia, caesarean operations and high birth weight.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):102-106
DOI 10.1590/S0100-72032012000300002
PURPOSE: To assess the prevalence of obstetric risk factors and their association with unfavorable outcomes for the mother and fetus. METHODS: A longitudinal, descriptive and analytical study was conducted on 204 pregnant women between May 2007 and December 2008. Clinical and laboratory assessments followed routine protocols. Risk factors included socio-demographic aspects; family, personal and obstetric history; high pre-gestational body mass index (BMI); excessive gestational weight gain and anemia. Adverse outcomes included pre-eclampsia (4.5%), gestational diabetes mellitus (3.4%), premature birth (4.4%), caesarian birth (40.1%), high birth weight (9.8%) and low birth weight (13.8%). RESULTS: The average age was 26±6.4 years; the mothers were predominantly non-white (84.8%), 51.8% had incomplete or complete secondary level schooling, 67.2% were in a stable marital relationship and 51.0% had a regular paid job; 63.7% were admitted to the prenatal clinic during the second trimester and 16.7% during the first, with 42.6% being primiparous. A past history of chronic hypertension was reported by 2.9%, pre-eclampsia by 9.8%, excessive gestational weight gain by 15.2% and former gestational diabetes mellitus by 1.0%. In the current pregnancy, elevated pre-gestational BMI was found in 34.6%; 45.5% presented with excessive gestational weight gain, 25.3% with anemia and 47.3% with dyslipidemia. Of the 17.5% of cases with altered blood glucose, gestational diabetes mellitus was confirmed in 3.4% and proteinuria occurred in 16.4% of all cases. Adverse maternal fetal outcomes included pre-eclampsia (4.5%), gestational diabetes mellitus (3.4%), premature birth (4.4%), caesarean birth (40.1%) and high and low birth weight (9.8% and 13.8%, respectively). Independent predictors of adverse maternal fetal outcomes were identified by Poisson multivariate regression analysis: pre-gestational BMI>25 kg/m² was a predictor for pre-eclampsia (RR=17.17; 95%CI 2.14-137.46) and caesarian operation (RR=1.79; 95%CI 1.13-2.85), previous caesarean was a predictor for present caesarean operation (RR=2.28; 95%CI 1.32-3.92) and anemia and high gestational weight gain were predictors for high birth weight (RR=3.38; 95%CI 1.41-8.14 and RR=4.68; 95%CI 1.56-14.01, respectively). CONCLUSION: Pre-gestational overweight/obesity, previous caesarean, excessive weight gain and anemia were major risk factors for pre-eclampsia, caesarean operations and high birth weight.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(3):102-106
DOI 10.1590/S0100-72032014000300002
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(3):102-106
DOI 10.1590/S0100-72032014000300002
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):102-103
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):102-103
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(3):102-109
To assess the prevalence of hypovitaminosis D, altered arterial blood pressure, and serum levels of glucose and lipids in community-dwelling women in the city of Ribeirão Preto, in the southeast of Brazil.
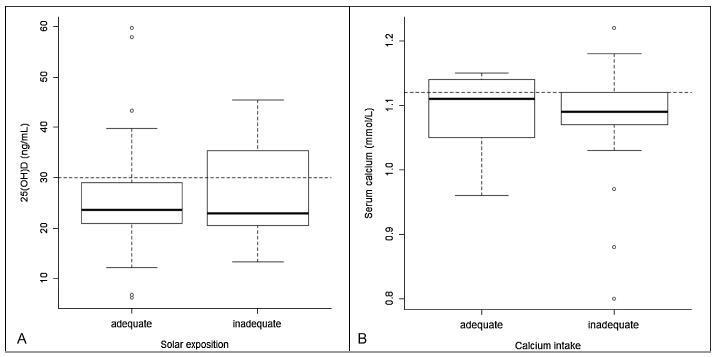
Thiswas a cross-sectional studyof women aged40-70years old.Calciumintake and level of sun exposure were assessed by means of a questionnaire. A blood sample was used to determine glucose, lipid profile and 25-hydroxyvitaminD(25[OH]D) concentration.
Ninety-one women were enrolled (age = 54.2 ± 7.1 years). Themean serum 25(OH)D concentration was 25.7 ± 8.9 ng/mL. A total of 24 (26.4%) women had 25 (OH)D levels < 20 ng/mL. Seventy women (76.9%) had 25(OH)D levels < 30 ng/mL. Seventy-five women (90.4%) had inadequate calcium intake, and 61 women (67%) had appropriate sun exposure, 49 of whom (80.3%) had serum 25(OH)D levels < 30 ng/mL.
This study indicates that even in community-dwelling women, living in a city with high sun exposure, serum levels of 25(OH)D > 30 ng/ml are hardly reached. Thus, it is probable that other intrinsic factors besides sun exposure may regulate the levels of vitamin D.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(3):102-109
To assess the prevalence of hypovitaminosis D, altered arterial blood pressure, and serum levels of glucose and lipids in community-dwelling women in the city of Ribeirão Preto, in the southeast of Brazil.
Thiswas a cross-sectional studyof women aged40-70years old.Calciumintake and level of sun exposure were assessed by means of a questionnaire. A blood sample was used to determine glucose, lipid profile and 25-hydroxyvitaminD(25[OH]D) concentration.
Ninety-one women were enrolled (age = 54.2 ± 7.1 years). Themean serum 25(OH)D concentration was 25.7 ± 8.9 ng/mL. A total of 24 (26.4%) women had 25 (OH)D levels < 20 ng/mL. Seventy women (76.9%) had 25(OH)D levels < 30 ng/mL. Seventy-five women (90.4%) had inadequate calcium intake, and 61 women (67%) had appropriate sun exposure, 49 of whom (80.3%) had serum 25(OH)D levels < 30 ng/mL.
This study indicates that even in community-dwelling women, living in a city with high sun exposure, serum levels of 25(OH)D > 30 ng/ml are hardly reached. Thus, it is probable that other intrinsic factors besides sun exposure may regulate the levels of vitamin D.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):102-102
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):102-102
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):102-102
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(2):102-102