Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(1):01-03
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(1):01-03
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(1):01-04
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(1):01-04
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):01-02
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):01-02
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):03-10
To evaluate the association between pain intensity in the active phase of the first stage of labor with the use or not of nonpharmacological methods for pain relief in a real-life scenario.
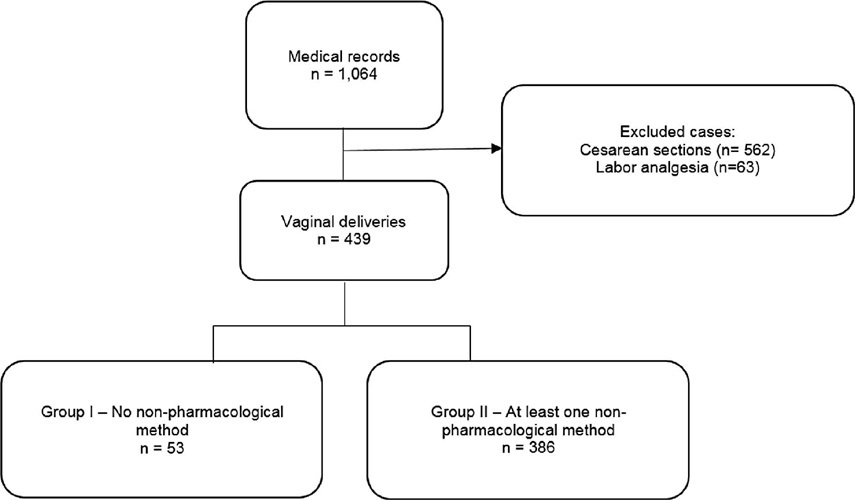
This was an observational cross-sectional study. The variables analyzed were obtained by a questionnaire with the mothers (up to 48 hours postpartum) to investigate the intensity of pain during labor using the visual analog scale (VAS). The nonpharmacological pain relief methods routinely used in obstetric practice were evaluated by consulting medical records. The patients were separated into two groups: Group I – patients who did not use nonpharmacological methods for pain relief and Group II –patients who used these methods.
A total of 439 women who underwent vaginal delivery were included; 386 (87.9%) used at least 1 nonpharmacological method and 53 (12.1%) did not. The women who did not use nonpharmacological methods had significantly lower gestational age (37.2 versus 39.6 weeks, p < 0.001) and shorter duration of labor (24 versus 114 min, p < 0.001) than those who used the methods. There was no statistically significant difference in the pain scale score using the VAS between the group that used nonpharmacological methods and the group that did not (median 10 [minimum 2– maximum 10] versus 10 [minimum 6–maximum 10] p = 0.334).
In a real-life setting, there was no difference in labor pain intensity between the patients who used nonpharmacological methods and those who did not use them during the active phase of labor.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):03-10
To evaluate the association between pain intensity in the active phase of the first stage of labor with the use or not of nonpharmacological methods for pain relief in a real-life scenario.
This was an observational cross-sectional study. The variables analyzed were obtained by a questionnaire with the mothers (up to 48 hours postpartum) to investigate the intensity of pain during labor using the visual analog scale (VAS). The nonpharmacological pain relief methods routinely used in obstetric practice were evaluated by consulting medical records. The patients were separated into two groups: Group I – patients who did not use nonpharmacological methods for pain relief and Group II –patients who used these methods.
A total of 439 women who underwent vaginal delivery were included; 386 (87.9%) used at least 1 nonpharmacological method and 53 (12.1%) did not. The women who did not use nonpharmacological methods had significantly lower gestational age (37.2 versus 39.6 weeks, p < 0.001) and shorter duration of labor (24 versus 114 min, p < 0.001) than those who used the methods. There was no statistically significant difference in the pain scale score using the VAS between the group that used nonpharmacological methods and the group that did not (median 10 [minimum 2– maximum 10] versus 10 [minimum 6–maximum 10] p = 0.334).
In a real-life setting, there was no difference in labor pain intensity between the patients who used nonpharmacological methods and those who did not use them during the active phase of labor.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(1):04-08
To evaluate the accuracy of fetal weight prediction by ultrasonography labor employing a formula including the linear measurements of femur length (FL) and mid-thigh soft-tissue thickness (STT).
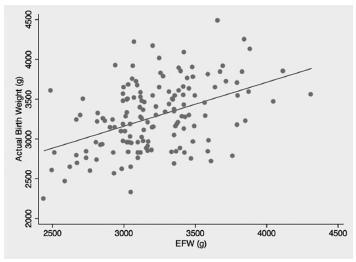
We conducted a prospective study involving singleton uncomplicated term pregnancies within 48 hours of delivery. Only pregnancies with a cephalic fetus admitted in the labor ward for elective cesarean section, induction of labor or spontaneous labor were included. We excluded all non-Caucasian women, the ones previously diagnosed with gestational diabetes and the ones with evidence of ruptured membranes. Fetal weight estimates were calculated using a previously proposed formula [estimated fetal weight = [1] 1687.47 + (54.1 x FL) + (76.68 x STT). The relationship between actual birth weight and estimated fetal weight was analyzed using Pearson's correlation. The formula's performance was assessed by calculating the signed and absolute errors. Mean weight difference and signed percentage error were calculated for birth weight divided into three subgroups: < 3000 g; 3000-4000g; and > 4000 g.
We included for analysis 145 cases and found a significant, yet low, linear relationship between birth weight and estimated fetal weight (p < 0.001; R2 = 0.197) with an absolute mean error of 10.6%. The lowest mean percentage error (0.3%) corresponded to the subgroup with birth weight between 3000 g and 4000 g.
This study demonstrates a poor correlation between actual birth weight and the estimated fetal weight using a formula based on femur length and mid-thigh soft-tissue thickness, both linear parameters. Although avoidance of circumferential ultrasound measurements might prove to be beneficial, it is still yet to be found a fetal estimation formula that can be both accurate and simple to perform.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(1):04-08
To evaluate the accuracy of fetal weight prediction by ultrasonography labor employing a formula including the linear measurements of femur length (FL) and mid-thigh soft-tissue thickness (STT).
We conducted a prospective study involving singleton uncomplicated term pregnancies within 48 hours of delivery. Only pregnancies with a cephalic fetus admitted in the labor ward for elective cesarean section, induction of labor or spontaneous labor were included. We excluded all non-Caucasian women, the ones previously diagnosed with gestational diabetes and the ones with evidence of ruptured membranes. Fetal weight estimates were calculated using a previously proposed formula [estimated fetal weight = [1] 1687.47 + (54.1 x FL) + (76.68 x STT). The relationship between actual birth weight and estimated fetal weight was analyzed using Pearson's correlation. The formula's performance was assessed by calculating the signed and absolute errors. Mean weight difference and signed percentage error were calculated for birth weight divided into three subgroups: < 3000 g; 3000-4000g; and > 4000 g.
We included for analysis 145 cases and found a significant, yet low, linear relationship between birth weight and estimated fetal weight (p < 0.001; R2 = 0.197) with an absolute mean error of 10.6%. The lowest mean percentage error (0.3%) corresponded to the subgroup with birth weight between 3000 g and 4000 g.
This study demonstrates a poor correlation between actual birth weight and the estimated fetal weight using a formula based on femur length and mid-thigh soft-tissue thickness, both linear parameters. Although avoidance of circumferential ultrasound measurements might prove to be beneficial, it is still yet to be found a fetal estimation formula that can be both accurate and simple to perform.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):04-10
To assess the association between dietary glycemic index (GI) and excess weight in pregnant women in the first trimester of pregnancy.
A cross-sectional study in a sample of 217 pregnant women was conducted at the maternal-fetal outpatient clinic of the Hospital Geral de Fortaleza, Fortaleza, state of Ceará, Brazil, for routine ultrasound examinations in the period between 11 and 13 weeks + 6 days of gestation.Weight and height were measured and the gestational body mass index (BMI) was calculated. The women were questioned about their usual body weight prior to the gestation, considering the prepregnancy weight. The dietary GI and the glycemic load (GL) of their diets were calculated and split into tertiles. Analysis of variance (ANOVA) or Kruskal-Walls and chi-squared (χ2) statistical tests were employed. A crude logistic regression model and a model adjusted for confounding variables known to influence biological outcomes were constructed. A p-value < 0.05 was considered significant for all tests employed.
The sample group presented a high percentage of prepregnancy and gestational overweight (39.7% and 40.1%, respectively). InthetertilewiththehigherGIvalue, therewasa lower dietary intake of total fibers (p = 0.005) and of soluble fibers (p = 0.008). In the third tertile, the dietary GI was associated with overweight in pregnant women in the first trimester of gestation, both in the crude model and in the model adjusted for age, total energy intake, and saturated fatty acids. However, this association was not observed in relation to the GL.
A high dietary GI was associated with excess weight in women in the first trimester of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):04-10
To assess the association between dietary glycemic index (GI) and excess weight in pregnant women in the first trimester of pregnancy.
A cross-sectional study in a sample of 217 pregnant women was conducted at the maternal-fetal outpatient clinic of the Hospital Geral de Fortaleza, Fortaleza, state of Ceará, Brazil, for routine ultrasound examinations in the period between 11 and 13 weeks + 6 days of gestation.Weight and height were measured and the gestational body mass index (BMI) was calculated. The women were questioned about their usual body weight prior to the gestation, considering the prepregnancy weight. The dietary GI and the glycemic load (GL) of their diets were calculated and split into tertiles. Analysis of variance (ANOVA) or Kruskal-Walls and chi-squared (χ2) statistical tests were employed. A crude logistic regression model and a model adjusted for confounding variables known to influence biological outcomes were constructed. A p-value < 0.05 was considered significant for all tests employed.
The sample group presented a high percentage of prepregnancy and gestational overweight (39.7% and 40.1%, respectively). InthetertilewiththehigherGIvalue, therewasa lower dietary intake of total fibers (p = 0.005) and of soluble fibers (p = 0.008). In the third tertile, the dietary GI was associated with overweight in pregnant women in the first trimester of gestation, both in the crude model and in the model adjusted for age, total energy intake, and saturated fatty acids. However, this association was not observed in relation to the GL.
A high dietary GI was associated with excess weight in women in the first trimester of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(1):04-10
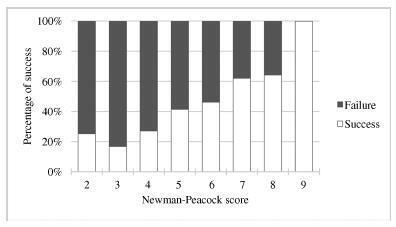
External cephalic version (ECV) is a maneuver that enables the rotation of the non-cephalic fetus to a cephalic presentation. The Newman-Peacock (NP) index, which was proposed by Newman et al. in a study published in 1993, was described as a prediction tool of the success of this procedure; it was validated in a North-American population, and three prognostic groups were identified.
To evaluate the value of the NP score for the prediction of a successful ECV in a Portuguese obstetrical population, and to evaluate maternal and fetal safety.
We present an observational study conducted from 1997-2016 with pregnant women at 36-38 weeks of pregnancy who were candidates for external cephalic version in our department. Demographic and obstetrical data were collected, including the parameters included in the NP index (parity, cervical dilatation, estimated fetal weight, placental location and fetal station). The calculation of the NP score was performed, and the percentages of success were compared among the three prognostic groups and with the original study by Newman et al. The performance of the score was determined using the Student t-test, the Chi-squared test, and a receiver operating characteristic (ROC) curve.
In total, 337 women were included. The overall success rate was of 43.6%. The univariate analysis revealed that multiparity, posterior placentation and a less engaged fetus were factors that favored a successful maneuver (p < 0.05). Moreover, a higher amniotic fluid index was also a relevant predictive factor (p < 0.05). The Newman-Peacock score had a poorer performance in our population compared with that of the sample of the original study, but we still found a positive relationship between higher scores and higher prediction of success (p < 0.001). No fetal or maternal morbidities were registered.
The Newman-Peacock score had a poorer performance among our population compared to its performance in the original study, but the results suggest that this score is still a useful tool to guide our clinical practice and counsel the candidate regarding ECV.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(1):04-10
External cephalic version (ECV) is a maneuver that enables the rotation of the non-cephalic fetus to a cephalic presentation. The Newman-Peacock (NP) index, which was proposed by Newman et al. in a study published in 1993, was described as a prediction tool of the success of this procedure; it was validated in a North-American population, and three prognostic groups were identified.
To evaluate the value of the NP score for the prediction of a successful ECV in a Portuguese obstetrical population, and to evaluate maternal and fetal safety.
We present an observational study conducted from 1997-2016 with pregnant women at 36-38 weeks of pregnancy who were candidates for external cephalic version in our department. Demographic and obstetrical data were collected, including the parameters included in the NP index (parity, cervical dilatation, estimated fetal weight, placental location and fetal station). The calculation of the NP score was performed, and the percentages of success were compared among the three prognostic groups and with the original study by Newman et al. The performance of the score was determined using the Student t-test, the Chi-squared test, and a receiver operating characteristic (ROC) curve.
In total, 337 women were included. The overall success rate was of 43.6%. The univariate analysis revealed that multiparity, posterior placentation and a less engaged fetus were factors that favored a successful maneuver (p < 0.05). Moreover, a higher amniotic fluid index was also a relevant predictive factor (p < 0.05). The Newman-Peacock score had a poorer performance in our population compared with that of the sample of the original study, but we still found a positive relationship between higher scores and higher prediction of success (p < 0.001). No fetal or maternal morbidities were registered.
The Newman-Peacock score had a poorer performance among our population compared to its performance in the original study, but the results suggest that this score is still a useful tool to guide our clinical practice and counsel the candidate regarding ECV.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(1):05-09
DOI 10.1590/SO100-720320140005130
To describe maternal and neonatal outcomes in pregnant women undergoing hemodialysis in a referral center in Brazilian Southeast side.
Retrospective and descriptive study, with chart review of all pregnancies undergoing hemodialysis that were followed-up at an outpatient clinic of high- risk prenatal care in Southeast Brazil.
Among the 16 women identified, 2 were excluded due to follow-up loss. In 14 women described, hypertension was the most frequent cause of chronic renal failure (half of cases). The majority (71.4%) had performed hemodialysis treatment for more than one year and all of them underwent 5 to 6 hemodialysis sessions per week. Eleven participants had chronic hypertension, 1 of which was also diabetic, and 6 of them were smokers. Regarding pregnancy complications, 1 of the hypertensive women developed malignant hypertension (with fetal growth restriction and preterm delivery at 29 weeks), 2 had acute pulmonary edema and 2 had abruption placenta. The mode of delivery was cesarean section in 9 women (64.3%). All neonates had Apgar score at five minutes above 7.
To improve perinatal and maternal outcomes of women undergoing hemodialysis, it is important to ensure multidisciplinary approach in referral center, strict control of serum urea, hemoglobin and maternal blood pressure, as well as close monitoring of fetal well-being and maternal morbidities. Another important strategy is suitable guidance for contraception in these women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(1):05-09
DOI 10.1590/SO100-720320140005130
To describe maternal and neonatal outcomes in pregnant women undergoing hemodialysis in a referral center in Brazilian Southeast side.
Retrospective and descriptive study, with chart review of all pregnancies undergoing hemodialysis that were followed-up at an outpatient clinic of high- risk prenatal care in Southeast Brazil.
Among the 16 women identified, 2 were excluded due to follow-up loss. In 14 women described, hypertension was the most frequent cause of chronic renal failure (half of cases). The majority (71.4%) had performed hemodialysis treatment for more than one year and all of them underwent 5 to 6 hemodialysis sessions per week. Eleven participants had chronic hypertension, 1 of which was also diabetic, and 6 of them were smokers. Regarding pregnancy complications, 1 of the hypertensive women developed malignant hypertension (with fetal growth restriction and preterm delivery at 29 weeks), 2 had acute pulmonary edema and 2 had abruption placenta. The mode of delivery was cesarean section in 9 women (64.3%). All neonates had Apgar score at five minutes above 7.
To improve perinatal and maternal outcomes of women undergoing hemodialysis, it is important to ensure multidisciplinary approach in referral center, strict control of serum urea, hemoglobin and maternal blood pressure, as well as close monitoring of fetal well-being and maternal morbidities. Another important strategy is suitable guidance for contraception in these women.